Download presentation
Presentation is loading. Please wait.

1
Sarcoidosis

2
SARCOIDOSIS Definition: Idiopathic systemic disorder characterized by accumulation of lymphocytes and monocytes in many organs forming noncaseating, epitheloid granuloma and subsequent conformational changes in the involved organs Etiology: unknown Extent of involvement : systemic Clinical course : variable from asymptomatic disease with spontaneous resolution to progressive disease with organ system failure Symptoms: dependent on site of involvement 1

3
Typically affects young adults between 20-60 years of age
Most frequently affects the lungs but some can present with extrathoracic manisfestation. Diffuse interstitial lung disease is the classic type of lung involvement Common presenting respiratory symptoms includes: Cough Dyspnoea Chest pain Also can present with systemic symptoms like fatigue, anorexia and skin lesion

4
Diagnosis: Chest radiograph
Bilateral hilar adenopathy is a classic finding in sarcoidosis Hilar may be symmetrically enlarged or the right may be slightly more prominent CXR findings are organized into stages (I-IV) which gives an anatomic guide to lung involvement
 which gives an anatomic guide to lung involvement.")
5
Diagnosis: Chest radiograph
Stage I Presence of bilateral hilar adenopathy which is often accompanied by paratracheal node enlargement. Regression of hilar nodes within 1-3 years occur in 75% of patients Stage II Consist of bilateral hilar adenopathy and reticular opacities (upper lung zone more than lower) Usually have mild to moderate symptoms (cough, dyspnea, fever and fatigue)
 Usually have mild to moderate symptoms (cough, dyspnea, fever and fatigue)")
6
Stage I Stage II

7
Diagnosis: Chest radiograph
Stage III Consist of reticular opacities with shrinking hilar nodes Predominantly distributed in upper zones Stage IV Reticular opacities with evidence of volume loss Marked traction bronchiectasis, extensive calcification and cavitation may also be seen

8
Stage III Stage IV

9
Diagnosis: Chest radiograph
HRCT can detect parenchymal and mediastinal abnormalities not seen on CXR. Eg: Hilar and mediastinal lymphadenopathy Beaded or irregular thickening of bronchovascular bundles Nodules along bronchi, vessels and subpleural regions Bronchial wall thickening Ground glass opacification Parenchymal masses or nodular consolidation, occasionally with cavitation Fibrosis with distortion of the lung architecture and traction bronchiectasis

10
Pulmonary Function Test
PFTs & 6MWT are used to assess the severity of respiratory impairment and monitor course of disease PFTs usually shows a restrictive pattern with a reduction in DLCO Serum ACE Activity elevated in % due to macrophage activity, but nonspecific Lacks diagnostic specificity and poor prognostic value in identifying patients with progressive disease

11
Bronchoscopy Bronchoscopy with BAL, endobronchial biopsy and transbronchial biopsy are tradiotnal methods for minimally invasive diagnosis of sarcoidosis BAL demonstrates: a reduced number of CD8 cells elevated CD4 to CD8 ratio increased amount of activated T cells, CD4 cells and immunoglobulins EUS or EBUS has a high diagnostic yield in patients with mediastinal adenopathy and a clinical suspicion of sarcoidosis

12
Kveim test Kveim test, Nickerson-Kveim or Kveim-Siltzbach test
Splenic cells from patients with sarcoidosis is injected intradermally to evoke a sarcoid granulomatous response over 3 weeks. Not commonly performed due to concerns on disease transmission

13
Extrapulmonary features
Periperal lymph node involvement Myocardial involvement 5-10% arrhythmias, heart failure (restrictive type), conduction abnormalities Occular involvement Anterior/posterior uveitis Conjunctivitis Skin plaques, papules, subcutaneous nodules keloid formation in atrophic scars erythema nodosum Lupus pernio - violaceous, chronic and disfiguring lesions of the ears, nose and cheeks
, conduction abnormalities. Occular involvement. Anterior/posterior uveitis. Conjunctivitis. Skin. plaques, papules, subcutaneous nodules. keloid formation in atrophic scars. erythema nodosum. Lupus pernio - violaceous, chronic and disfiguring lesions of the ears, nose and cheeks.")
14
Extrapulmonary features
Neurological disease – facial palsy Other organs eg: Liver Joints Splenomegaly Lacrimal gland Parotid gland Bone involvement Sarcoid dactylitis

15
Lupus Pernio

16
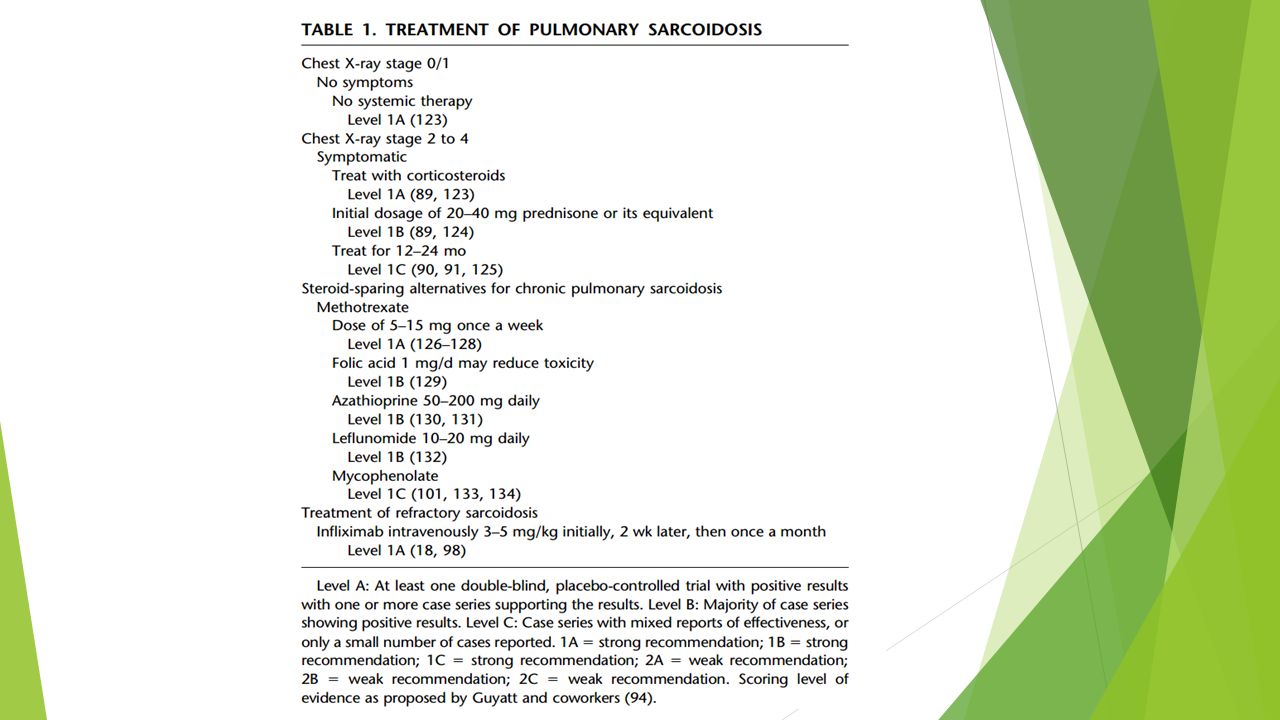
TREATMENT Corticosteroids Cytotoxic agents:
methotrexate, azathioprine, chlorambucil, cyclophosphamide Other agents : antimalarials, ketoconazole, NSAID’s • Infliximab

17
Treatment Treatment of sarcoidosis is usually limited to symptomatic patients Treatment decision have to consider that patients may have spontaneous resolution of the disease Criteria for institution of glucocorticoid therapy Disabling symptoms (Fever, Arhtralgias, Cough, Dyspnoea, Chest discomfort, Exercise limitation) Organ dysfunction/derangement Abnormal tests (Hypercalcaemia, Abnormal LFTs) Ancillary criteria (Elevated levels of BAL lymphocytes
 Organ dysfunction/derangement. Abnormal tests (Hypercalcaemia, Abnormal LFTs) Ancillary criteria (Elevated levels of BAL lymphocytes.")
Similar presentations
 Infections (pneumonia, airways disease)>")
















 r Thin elastin-rich connective component containing.>")

