Download presentation
Presentation is loading. Please wait.

2
Simon Baudouin Senior Lecturer in Critical Care University of Newcastle

3
Conventional definitions ◦ Type 1 PaO 2 < 8 kPa on air ◦ Type 2 PaO 2 6 kPa Not helpful! ◦ Ultimately all severely ill patients become hypercapnic without intervention Acute Chronic Acute on chronic Reach ITU v intubate in EAU

4
Hypoxaemia – V/Q mismatch & shunt Hypercapnia ◦ Hypoventilation ◦ Increase in deadspace ventilation ◦ V/Q mismatch

5
Uk National COPD audit 2003; Thorax 2006;61:837-842 234 UK acute hospitals 40 consecutive acute COPD admissions 7259 patients 90 day readmission rate 31.4%!

6
16-47% hypercapnia Half will need ventilatory support - Plant et al, Thorax, 2000; 55: 550-554 -1 year survey in Leeds 983 admissions 2.2% ICU admissions 73% hospital mortality in ICU admissions 70 NIV patients/year/250,000 population

7
Explanation of hypoxaemia and hypercapnia Multiple inert gas elimination Broad V/Q distribution Hypercapnia = ventilation to under-perfused units Hypoxaemia = shunting Respiratory muscle fatigue? Altered central drive?

8
Hypoxaemia is usually correctable with low flow O 2 The optimal target SaO 2 is unknown > 90% - O 2 dissociation curve > 85% (ARDS net) One small study (n = 36) 6.6hPa v 9.0 hPa -no difference (underpowered) High flow O 2 will worsen Hypercapnia Change to controlled O 2 will reduce PaCO 2
 One small study (n = 36) 6.6hPa v 9.0 hPa -no difference (underpowered) High flow O 2 will worsen Hypercapnia Change to controlled O 2 will reduce PaCO 2")
10
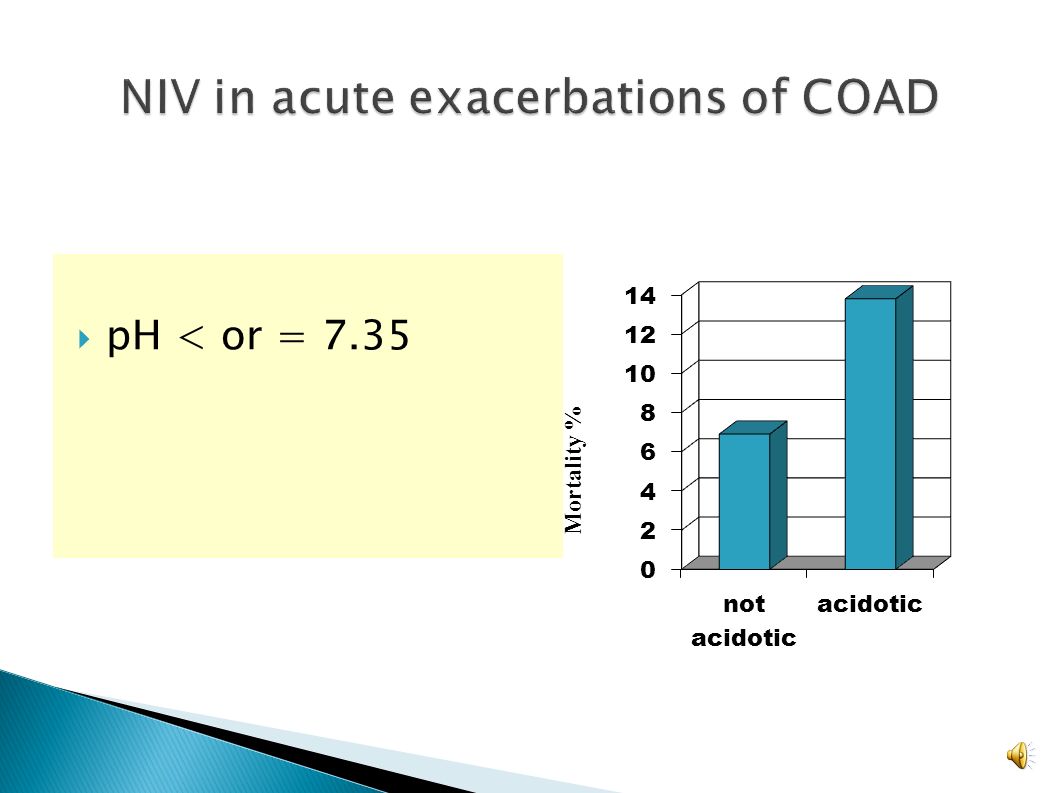
pH < or = 7.35 Mortality %

11
Randomised controlled trials in NIV Early use of non-invasive ventilation for acute exacerbations of chronic obstructive pulmonary disease on general respiratory wards: a multicentre, randomised, controlled trial. Plant et al. Lancet, 2000; 355: 1931-35 14 UK Hospitals n = 236 Mortality p = 0.05 Intubation p = 0.02

12
BMJ 2003;326:185-190 Typical UK hospital will avoid 3-9 ICU admissions/year Save £12,000- 53,000

13
“The use of non-invasive positive pressure ventilation in the emergency department” RCT 6/12 study NIV vs. conventional support 87 screened -34 “immediate” intubation -27 entered -11 conventional -16 NIV Wood. Chest, 1998; 113: 1339-46

14
Time to intubation Standard 4.8 hrs NIV 26.0 hrs NIV in A&E

15
Should all patients receive NIV in a critical care area? No RCTs Majority of trials are in Critical Care areas Plant

17
Recommendations of the COAD and NIV Standards of Care sub-committees of the British Thoracic Society, RCP & Modernisation Agency Every acute admissions unit should have an NIV service

18
-Failure rate 7-50% -delay intubation Acidosis APACHE II -Indications for HDU admission For intubation if NIV fails Initial pH 7.25 or less Worsening pH on NIV

19
Patient choice Failure of NIV Usually obvious clinically ◦ Fatigued “awful looking” patient ◦ Worsening hypercapnia and LOC ◦ A&E arrest/peri-arrest situation

20
Patient/ventilator interactions Weaning Tracheostomy Nutrition The “unweanable” patient

21
Rapid trial of extubation (onto NIV) Early tracheostomy Regular Sedation cessation Weaning protocols A little progress every day!
 Early tracheostomy Regular Sedation cessation Weaning protocols A little progress every day!")
22
N=43 (most with COAD failed wean for 3 days Shorter ICU & hospital LOS Less need for tracheostomy 90 day survival Am J Respir Crit Care Med 2003;168:70-6

24
COPD admissions will increase NIV is effective in both survival and prevention of intubation Outcome of ventilation in COPD is no worse than in other conditions Patient choice and informed decisions

25
Previously fit 24 year old women First pregnancy No problems until week 35 “Cough and cold” “Shivery” Increasingly breathless over 24 hours Brought to maternity ward by husband Clearly very unwell SaO2 air 79% RR 35/min Crackles ++ Foetus alive Critical Care outreach called

27
Early corticosteroids in severe influenza A/H1N1 pneumonia and acute respiratory distress syndrome. Am J Respir Crit Care Med. 2011 May 1;183(9):1200-6. French national registry – no benefit; possible early harm European SICM database Cox analysis no benefit from steroids
: French national registry – no benefit; possible early harm European SICM database Cox analysis no benefit from steroids.")
28
Critical Care obstetric intensivist Separate the two patients Foetus is viable Ventilation for the Mother is inevitable Experience from other units Urgent Caesarean section Ventilated with Critical Care ventilator during section Healthy girl delivered Mother transferred to critical care unit

29
Substitute for the respiratory muscle pump Complex multi- functional machines Efficacy established during polio epidemics 1960s Led to development of modern, centralised critical care services

30
Broncho- pulmonary dysplasia Well + Tierney 1974 - rats ventilated with peak airway pressures 45 cm H 2 O developed pulmonary oedema Carlton 1990 - Lung overexpansion increases lymph flow in lambs Lymph flow ml/Kg

31
Mortality at 180 days Protection 31.0% Conventional 39.8% P = 0.007

32
Normal lung Partial collapse/floodingComplete collapse recruitable

33
5 cm PEEP

34
N = 1000 60 day mortality Liberal v conservative fluid

35
Improved oxygenation Increased ventilator free days No increase in shock or dialysis

36
N = 549 How much PEEP? Higher versus lower PEEP in patients with ARDS New Engl J Med 2004;351:327-336 Lower PEEP = 8 cm H 2 O Higher PEEP = 13 cm H 2 O

37
Often improves oxygenation Proposed mechanisms -recruitment of dorsal collapsed lung units -improved respiratory mechanics -increased secretion drainage -decreased injury from mechanical forces

38
Prone positioning in ARDS N=304 N=791

39
Initial improvement in PaO2/SaO2 to 90% Gradual fall to SaO2 84% CXR – no mechanical cause

40
Rescue = desperation Rescue = no high grade evidence Rescue = risks as well as possible benefits ◦ Oscillator ventilation ◦ ECMO

41
Rate 60 – 100 bpm TV below anatomic deadspace Alveoalar derecruitment & overdistention limited

42
Large, multi-centre RCT Conventional v high frequency ventilation Complete recruitment 2012 Over 800 patients

43
ECMO

45
Outcome in 1 ECMO centre (Glenfields) Protocolised care Experienced experts Average outcome in 92 conventional centres 11 referral centres Non protocolised care Variable experience Variable clinical cover/team
 Protocolised care Experienced experts Average outcome in 92 conventional centres 11 referral centres Non protocolised care Variable experience Variable clinical cover/team")
46
Hypoxaemia is the greatest immediate threat Severe oxygen induced hypercapnia is rare Oxygen induced hypercapnia only occurs in chronic respiratory failure Previously well patients with hypercapnia are severely ill Hypercapnia does not equate to COPD

Similar presentations



 for severe sepsis and septic shock treatment>")


















