Download presentation
Presentation is loading. Please wait.

1
Clinical Pathology: an introduction Dewi Wulandari Clinical Pathology Department Faculty of Medicine, University of Indonesia Cipto Mangunkusumo Hospital Jakarta

2
Introduction Clinical pathology = laboratory medicine Is the medical disipline in which clinical laboratory science and technology are applied to the care of patients Role of clinical pathology: Screening & risk factor determination Confirm or rule out the possibilities of differential diagnosis Monitoring Prognosis determination Complication identification.

3
Better Clinical Decision Medical history Physical finding Appropriate Laboratory tests

4
Clinical Pathology Services Clinical pathology, comprises : Hematology & hemostasis Clinical chemistry Urinalysis & body fluid analysis Microbiology Flow cytometry & molecular biology POCT (Point-of-Care Testing)
")
5
Hematology Hematology = the study of blood blood cells : erythrocytes (RBCs), leukocytes (WBCs), thrombocytes (Platelets). The routine hematology screening test for the blood : complete blood count (CBC) includes : Hb, Ht, RBC count, WBC count, Plt count, percentage differential of the WBC present. The results of CBC are useful in diagnosing anemia, leukemia, infectious processes of several etiologies. Other tests in hematology : Microscopic examination of stained blood film, ESR, reticulocyte count, & bone marrow.
 includes : Hb, Ht, RBC count, WBC count, Plt count, percentage differential of the WBC present. The results of CBC are useful in diagnosing anemia, leukemia, infectious processes of several etiologies. Other tests in hematology : Microscopic examination of stained blood film, ESR, reticulocyte count, & bone marrow..")
6
Hematology The results of CBC are useful in diagnosing anemia, leukemia, infectious processes of several etiologies. Decreased count of blood cells, may be related to : Blood loss Impaired of blood cells productions Increased of blood destruction/consumption Increased count of blood cells : Increased need Malignancies of hematopoietic system Reactive conditions

7
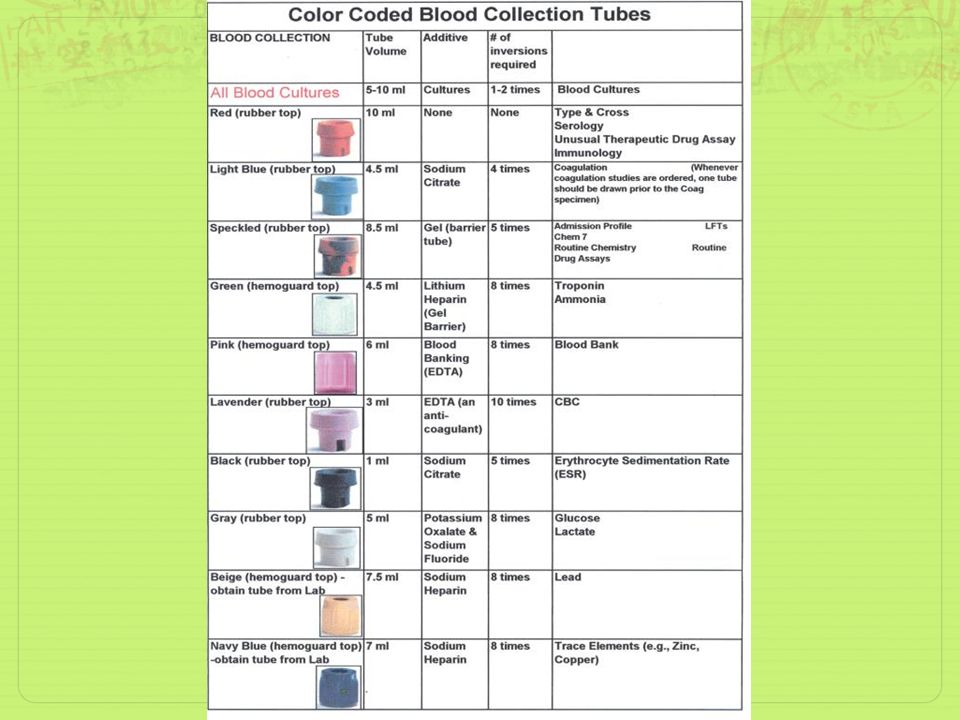
Hematology Anticoagulants : Prevent coagulation of blood Proper proportion to the blood Specific type for specific procedure

9
Diagnosis of Anemia Normocytic Anemia Macrocytic Microcytic Normal/increase Low Serum Ferritin Reticulocyte count ACD Thalassemia ACD Thalassemia Iron deficiency Increase Not increase Hemolytic Blood loss Hemolytic Blood loss Marrow hypoplasia Leukemia Infiltration Marrow hypoplasia Leukemia Infiltration Blood B12 & folate B12 and/or folate deficiency

10
Hemostasis & Coagulation To assess bleeding and clotting problems. To identify potential bleeding & thrombosis disorder To monitor anticoagulant therapy Tests most often performed : PT APTT D-dimer Bleeding time

11
Coagulation Cascade

12
Hemostasis & Coagulation PT (Prothrombin time) : Measures the activity of extrinsic pathway Screens for deficiencies of factor I, II, V, VII, and X For oral anticoagulant monitoring Convert to INR for monitoring APTT (Activated Partial Thromboplastin Time) Screen procedure for factor deficiencies of intrinsic & common pathways Prolonged in deficiencies of factor VIII, IX, XI, and XII For Heparin treatment monitoring, but not for LMWH
 : Measures the activity of extrinsic pathway Screens for deficiencies of factor I, II, V, VII, and X For oral anticoagulant monitoring Convert to INR for monitoring APTT (Activated Partial Thromboplastin Time) Screen procedure for factor deficiencies of intrinsic & common pathways Prolonged in deficiencies of factor VIII, IX, XI, and XII For Heparin treatment monitoring, but not for LMWH")
13
Hemostasis & Coagulation D-dimer : Cross-linked fibrin degradation product Marker for coagulation activation May increase in : thromboembolism & DIC Bleeding time Screen procedure for capilar integrity, platelet count and platelet function. Prolonged in von Willebrand disease, thrombocytopenic purpura, abnormal capillary integrity Normal in : hemophilia & other defect of clotting mechanism.

14
Urinalysis One of the most screening test done in clinical laboratories. Provide information for the detection of the diseases related to kidney & urinary tract. By evaluating 3 component part of urinalysis : Physical characteristics (color, clarity, specific gravity) Chemical constituent Microscopic examination of urine sediment
 Chemical constituent Microscopic examination of urine sediment.")
15
Chemical constituent of urine

16
Urinalysis Useful for diagnosis & monitoring of : Metabolic diseases (e.g. Diabetes Mellitus) Kidney disease Infection of the urinary tract
 Kidney disease Infection of the urinary tract.")
17
Clinical Chemistry Performs quantitative analytical procedure on body fluid, serum, or plasma Routine tests, include : Liver function tests Renal function tests Lipid profile Blood glucose tests Blood gas & electrolyte Cardiac markers

18
Liver Function Tests Abnormal biochemical tests for liver function may suggest : Hepatocellular damage Cholestasis Excretory function Biosynthesis function In the suspicion of viral hepatitis : hepatitis viral marker may be added

19
CategoryLaboratory assayComments Hepatocellular damage ASTFound in liver, cardiac muscle, skeletal muscle, kidney, brain, pancreas ALTFound primarily in liver CholestasisALPMay also increase in period of growth & pregnancy GGTSensitive for small liver insult (e.g. alcohol consumption), may also increase in hepatocellular damage Liver Excretory function Serum bilirubinProduct of heme catabolism Jaundice : > 1.5mg/dl Unconjugated bilirubin : hepatic jaundice Conjugaetd bilirubin : post hepatic jaundice Biosynthetic function Total protein, albumin, globulin Altered rasio albumin/globulin Coagulation factorsPT is the most sensitive test for liver synthetic fuction CholinesteraseSpecific for liver synthetic function
, may also increase in hepatocellular damage Liver Excretory function Serum bilirubinProduct of heme catabolism Jaundice : > 1.5mg/dl Unconjugated bilirubin : hepatic jaundice Conjugaetd bilirubin : post hepatic jaundice Biosynthetic function Total protein, albumin, globulin Altered rasio albumin/globulin Coagulation factorsPT is the most sensitive test for liver synthetic fuction CholinesteraseSpecific for liver synthetic function.")
20
Renal Function Tests Ureum / Blood Urea Nitrogen Waste product of protein breakdown Convert by the liver from ammonia to urea Determined by : dietary protein & renal excretory function Ureum = 2.14 x BUN Uremia : abnormally high urea nitrogen in the blood Azotemia : increased of plasma concentration of urea & creatinine

21
Renal Function Tests Prerenal azotemia : Result of poor perfusion of the kidney Normal renal function Renal azotemia : Decreased glomerular filtration rate as result of intrinsic kidney disease Postrenal azotemia : Result of any type of obstruction Urea is reabsorbed into the circulation Obstruction : stones, enlarged prostate gland, tumor

22
Creatinine Result from spontaneous formation from creatine and creatine phosphate Produced in constant rate, and related to muscle mass Clearence of creatinine from the plasma by the kidney = indicator for glomerular filtration rate Clearence of creatinine : Measured Predicted : Calculated by Cockroft-Gault Modification

23
Creatinine Clearance of creatinine (CCT) = U/P x V x 1.73/A (ml/min) U : urine creatinine concentration (mg/dl) P : plasma creatinine concentration (mg/dl) V : volume of urine excreted/min [24 hrs urine collected (ml)/(24x60 min)] 1.73 : standard body surface area A : patients body surface area (height & body weight are used with a nomogram) Cockroft-Gault Modification equation : C CR (ml/min) = (140-age) x weight x(0.85 if female) 72 x S cr
![Creatinine Clearance of creatinine (CCT) = U/P x V x 1.73/A (ml/min) U : urine creatinine concentration (mg/dl) P : plasma creatinine concentration (mg/dl) V : volume of urine excreted/min [24 hrs urine collected (ml)/(24x60 min)] 1.73 : standard body surface area A : patients body surface area (height & body weight are used with a nomogram) Cockroft-Gault Modification equation : C CR (ml/min) = (140-age) x weight x(0.85 if female) 72 x S cr](http://images.slideplayer.com/39/10967031/slides/slide_23.jpg "Creatinine Clearance of creatinine (CCT) = U/P x V x 1.73/A (ml/min) U : urine creatinine concentration (mg/dl) P : plasma creatinine concentration (mg/dl) V : volume of urine excreted/min [24 hrs urine collected (ml)/(24x60 min)] 1.73 : standard body surface area A : patients body surface area (height & body weight are used with a nomogram) Cockroft-Gault Modification equation : C CR (ml/min) = (140-age) x weight x(0.85 if female) 72 x S cr")
24
Blood Glucose Glucose is the primary source of energy. Insulin regulates the concentration of blood glucose. Normal blood concentration range : 70 – 110 mg/dl. Hypoglicemia : < 50 mg/dl, Hyperglicemia :most frequently caused by Diabetes Mellitus Blood glucose concentration : increased rapidly after carbohydrate-rich meal. Return to normal : 1 ½ - 2 hrs (postprandial level)
.")
25
HbA1c = glycosylated hemoglobin. Formed by binding of glucose to amino group of Hb A protein. Total amount of HbA1c is related to average glucose concentration over the 4 – 6 weeks before measurement. As glycemic control for diabetes patients. Not for diagnosis.

26
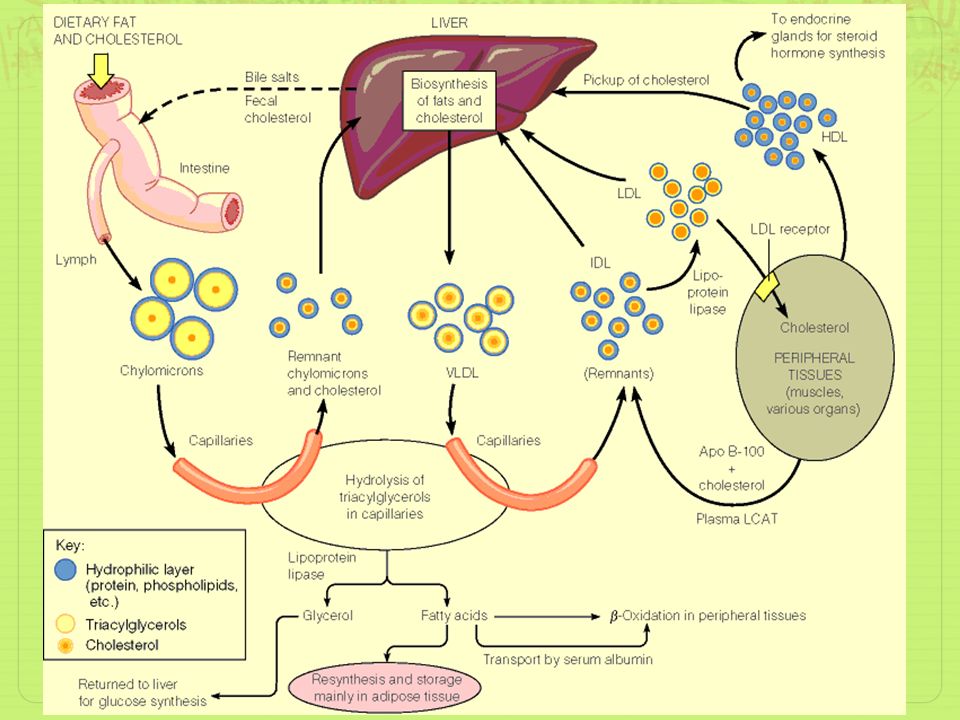
Lipid profile

28
Includes : Triglyceride, Total cholesterol, HDL, chol, LDL chol. TG = chylomicron exogenoeus pathway influenced by recent meal Total cholesterol, Chol HDL, Chol LDL endogen lipid metabolism not influenced by recent meal LDL chol : direct measurement or calculated by Friedewald equation : Chol LDL = 1/5 (Total chol – HDL chol – TG) Preparation : fasting 10 + 2 hrs. Hyperlipidemia risk factor for MCI, metabolic syndrome
 Preparation : fasting hrs. Hyperlipidemia risk factor for MCI, metabolic syndrome.")
29
Cardiac Markers Biochemical markers for acute cardiac events. Recommended to use serial sampling Acute myocardial injury : Myoglobin, Troponins, CK isoenzymes

30
Immunology & Serology Performs analytical procedures on body fluid, serum, or plasma based on antigen-antibody procedure Tests, include : Serology tests for infectious diseases Immune system disorders (autoimmunity, hypersensitivity, immunodeficiency)
")
31
Serologic tests for infectious diseases May detect antigen of the pathogen, or antibody Provide specific & sensitive tests More rapid than microorganism culture “Window period”

32
Tests for Immune System Hypersensitivity : IgE total & IgE specific Eosinophil count Autoimmunity : ANA dsDNA RF Complement Immunodeficiency : Lymphocyte subset

33
Microbiology Performs tests to : microorganisms identification + antimicrobial susceptibility test Specimens for microbiology testing : Blood Urine Sputum Body fluids Swab (throat, wounds, etc.) Secrete & discharge
 Secrete & discharge")
34
Microbiology Routine tests, include : Aerobic culture Anaerobic culture Gram staining Acid-fast staining Wet mount tests Antimicrobial susceptibility test Room sterility tests

35
POCT Point-of-Care Testing : laboratory assays performed near the patient (bed-site) Advantages : Smaller blood specimen required Faster turnaround time Reduction of length of hospital stay Patient convenient Improved patient care management Disadvantages : QC management difficult Lack of record Unable to repeat
 Advantages : Smaller blood specimen required Faster turnaround time Reduction of length of hospital stay Patient convenient Improved patient care management Disadvantages : QC management difficult Lack of record Unable to repeat")
36
POCT POCT analyzer : Glucose Urea Blood gas Electrolyte (Na, K, Cl, Mg) Coagulation Frequently located In ICU Emergency department Operation theatre
 Coagulation Frequently located In ICU Emergency department Operation theatre")
Similar presentations




>")
>")


 Compounds>")








>")

