Download presentation
Presentation is loading. Please wait.

1
CASE PRESENTATION Dr. Matu K - MBChB Dr. Ndanya S –Consultant Orthopedic Surgeon Embu Level V Hospital- Surgical Department

2
BIODATA NAME : D N AGE :48 YEARS GENDER :MALE OCCUPATION : BUSINESSMAN DATE OF ADMISSION:04/04/2016.

3
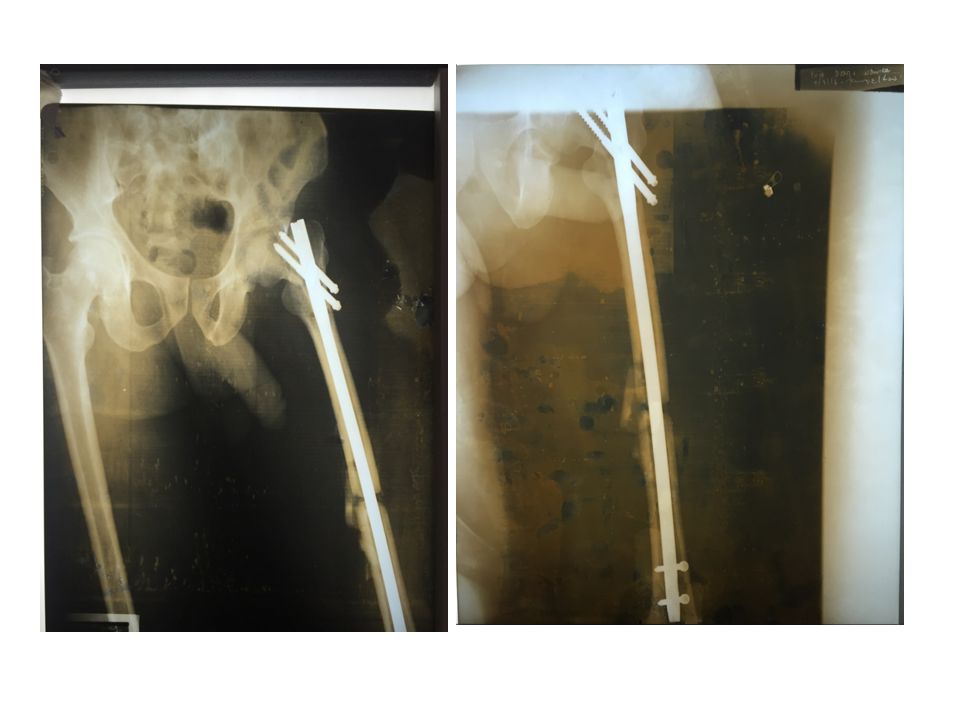
HISTORY SUMMARY Multiple fractures- Lt Femur -midshaft & neck fractures Lt proximal radius and ulna # Sustained following a head on collision between a motorcycle and a vehicle on 12/12/2015. Admitted at a Hospital where Intramedullary nailing was done. Two weeks later, nail was changed to a reconstruction nail secondary to undiagnosed # neck of femur.

4
Patient reportedly developed sepsis, discharging wounds at the points of screw insertion about 3 weeks Post OP. Daily cleaning and dressing was done and patient covered on antibiotics for about four months Due to financial constraints and emotional stress, patient reportedly declined ORIF for the upper limb fractures and a back slab was put thereof. Due to the same financial constraints the patient requested transfer to Embu level 5 near his home place

5
CHALLENGES – Chronic osteomyelitis left femur with implant insitu – Left femur shaft fracture non union with large gap – Left neck of femur # non union with displaced proximal screws – Non-union fracture Lt proximal 1/3 radius and ulna. – Anemia & Cachexia – Emotionally & financially drained patient in a resource poor centre with many limitations.

10
INVESTIGATIONS FHG done. Patient anemic with Hb 6.7 g/dl. – Esr 64mm/hr U/E/C done on admission were within normal range. HIV- NR Check plain radiographs taken. Pus swabs taken for m/c/s- Staphylococcus aureus isolated – sensitive to Kanamycin and Minocycline.

11
MANAGEMENT Antibiotics- Emperical IV Flucloxacillin later changed to Kanamycin after results of the sensitivity Analgesic-Ibuprofen. PPI- Omeprazole IV rehydration. Daily cleaning and dressing.

12
Patient transfused 5 pints of blood Hematinics- Ranferon. He developed deafness following 2 weeks of kanamycin use. Kanamycin was stopped. He is currently on IV Meropenem. The 2 proximal screws were removed on 19th 05 2016 since they were causing the patient severe hip pain. Screws were loose. Pain resolved. Fracture of upper limbs immobilized in a rigid orthopedic splint.

13
CURRENT STATUS Patient has markedly improved. Pus discharge decreased tremendously with daily cleaning and dressing and meropenem administration. Patient not anaemic. Last check Hb was 10.0 g/dl. Patient has added weight and his emotional status improved. Patient’s hearing is improving

14
PLAN Insertion of K nail with antibiotic impregnated bone cement Head of femur removal and spacer placement. For possible total hip replacement at a later stage. Plating for radius & Ulnar fractures. Occupational therapy & Physiotherapy.

Similar presentations