Download presentation
Presentation is loading. Please wait.

1
رئيس شعبة الجراحة العامة الأولى بمستشفى الأسد الجامعي
سرطان المعدة Gastric Cancer الأستاذ الدكتور حمود حامد رئيس شعبة الجراحة العامة الأولى بمستشفى الأسد الجامعي

2
Epidemiology second leading cause of cancer death and fourth most common cancer worldwide Overall declining Histologic pattern is shifting from predominantly intestinal type (distal) to diffuse type (proximal / cardia ( Gastric cancer. In: NCCN Clinical Practice Guidelines in Oncology. V National Comprehensive Cancer Network;2013
 to diffuse type (proximal / cardia ( Gastric cancer. In: NCCN Clinical Practice Guidelines in Oncology. V. 2 National Comprehensive Cancer Network;2013.")
3
Endemic areas persist

4
Factor increasing or decreasing gastric CA
Increase risk Family history Diet (high in nitrates, salt, fat) Familial polyposis Gastric adenomas Hereditary nonpolyposis colorectal cancer Helicobacter pylori infection Atrophic gastritis, intestinal metaplasia ,dysplasia Previous gastrectomy or gastrojejunostomy (>10 y ago) Tobacco use Decrease risk Diet (high fresh fruit and vegetable intake) Vitamin C GASTRIC ADENOCARCINOMA AND OTHER GASTRIC NEOPLASMS,MAINGOT ABDOMINAL OPERATION 12TH EDITION 2013
 Familial polyposis. Gastric adenomas. Hereditary nonpolyposis colorectal cancer. Helicobacter pylori infection. Atrophic gastritis, intestinal metaplasia ,dysplasia. Previous gastrectomy or gastrojejunostomy. (>10 y ago) Tobacco use. Decrease risk. Diet (high fresh fruit and vegetable intake) Vitamin C. GASTRIC ADENOCARCINOMA AND OTHER GASTRIC NEOPLASMS,MAINGOT ABDOMINAL OPERATION 12TH EDITION")
5
Standard Controversial Work-up/Staging CT chest, abdomen/pelvis PET-CT
Endoscopic Ultrasound EUS Controversial Laparoscopy Peritoneal washing RECOMMENDED IN ALL STAGE IB-III STOMACH CANCERS Gastric cancer: ESMO–ESSO–ESTRO Clinical Practice Guidelines for dignosis,treatment and follow up 2014

6
Gastric Cancer-surgical controversies
Resection Margins Extent of Lymphadenectomy Role of Sentinel Lymph Node Biopsy Minimally-Invasive Resection Endoscopic Mucosal Resection (EMR) Laparoscopic Resection
 Laparoscopic Resection.")
7
Surgical Margins

8
Subtotal vs. Total Gastrectomy?
Factors Influencing Operation Extent of disease Histological type Diffuse – total gastrectomy Intestinal – potentially subtotal gastrectomy Location (for intestinal type) Lower – subtotal gastrectomy(near-total) Upper, mid – total gastrectomy < 2 cm of GE junction- Esophagogastrectomy
 Lower – subtotal gastrectomy(near-total) Upper, mid – total gastrectomy. < 2 cm of GE junction- Esophagogastrectomy.")
9
D1 vs. D2 Resection – Where do we stand?
Definitions Theoretical Considerations Review of Clinical Trials Controversy Japanese vs. Western Data Proposed Approaches Conventional Utilizing the Maruyama Index

10
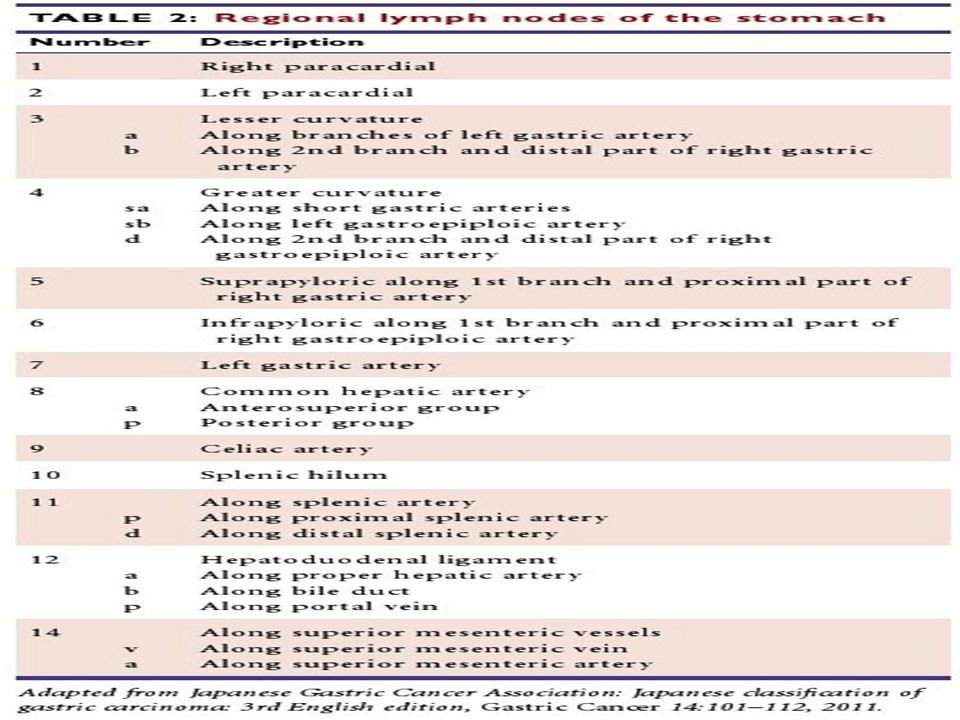
Lymph Node Stations (Japanese)
")
14
Synopsis of Definitions - D1 vs. D2
7 station left gastric

15
Synopsis of Definitions – D1 vs. D2
D2 Lymphadenectomy (“Radical Lymphadenectomy”) Additional tissue (en bloc): Greater and lesser omentum Superior leaf of mesocolon Pancreatic capsule Lymph nodes: Infra/supraduodenal areas Hepatic and common hepatic arteries Celiac artery Splenic artery Organs Distal pancreatectomy (station 11 lymph nodes) Splenectomy (station 10 lymph nodes
 Additional tissue (en bloc): Greater and lesser omentum. Superior leaf of mesocolon. Pancreatic capsule. Lymph nodes: Infra/supraduodenal areas. Hepatic and common hepatic arteries. Celiac artery. Splenic artery. Organs. Distal pancreatectomy (station 11 lymph nodes) Splenectomy (station 10 lymph nodes.")
18
Radical Lymphadenectomy (D2) Theoretical Considerations
Asian trials D2 lead to superior outcomes compared to D1 West, a Dutch and a UK Medical ResearchCouncil (MRC) trial Failed to demonstrate any initial survival advantage with D2 resection. the 15-year follow-up results from the Dutch trial demonstrated fewer locoregional recurrences and gastric cancer-related deaths with D2 resection A recent meta-analysis of 12 randomised controlled trials (RCTs) no overall survival (OS) benefit for D2 lymphadenectomy Songun I, Putter H, Kranenbarg EM, et al. Surgical treatment of gastric cancer:15-year follow-up results of the randomised nationwide Dutch D1D2 trial. Lancet Oncol 2010;11:439–49. Jiang L, Yang KH, Guan QL, et al. Survival and recurrence free benefits withdifferent lymphadenectomy for resectable gastric cancer: a meta-analysis. JSurg Oncol 2013;107:807–14.
 trial. Failed to demonstrate any initial survival advantage with D2 resection. the 15-year follow-up results from the Dutch trial demonstrated fewer locoregional recurrences and gastric cancer-related deaths with D2 resection. A recent meta-analysis of 12 randomised controlled trials (RCTs) no overall survival (OS) benefit for D2 lymphadenectomy. Songun I, Putter H, Kranenbarg EM, et al. Surgical treatment of gastric cancer:15-year follow-up results of the randomised nationwide Dutch D1D2 trial. Lancet Oncol 2010;11:439–49. Jiang L, Yang KH, Guan QL, et al. Survival and recurrence free benefits withdifferent lymphadenectomy for resectable gastric cancer: a meta-analysis. JSurg Oncol 2013;107:807–14.")
19
Radical Lymphadenectomy (D2) Theoretical Considerations
Pros More Accurate Staging (Prognostic Information) Lymph node status likely to influence adjuvant therapy Better Locoregional Control More extensive surgery Removes occult nodal disease Improved Survival Retrospective Japanese data No Excess Morbidity/Mortality Japanese experience
 Lymph node status likely to influence adjuvant therapy. Better Locoregional Control. More extensive surgery. Removes occult nodal disease. Improved Survival. Retrospective Japanese data. No Excess Morbidity/Mortality. Japanese experience.")
20
Radical Lymphadenectomy (D2) Theoretical Considerations
The current consensus view in the West D2 dissection should be the standard procedure carried out in specialised ,high-volume centres with appropriate surgical expertise. Dikken JL, van Sandick JW, Allum WH, et al. Differences in outcomes ofoesophageal and gastric cancer surgery across Europe. Br J Surg2013

21
Radical Lymphadenectomy (D2) Theoretical Considerations
Advanced disease not amenable to more radical locoregional surgery No “true” survival advantage Survival advantage of radical surgery merely an artifact of more accurate staging by nodal clearance “Stage migration” Western data does not support Japanese experience Excess morbidity/mortality/cost Western data

22
Minimally Invasive Resection
Types : Laparoscopic Intraperitoneal distal gastrectomy(long-term outcomes, reduced nodal harvest) Total gastrectomy( operative morbidity, technique of anastomosis) Ongoing trials in Japan,China,Korea(open versus laparoscopic surgery in early gastric cancer) Endoscopic Mucosal Resection (EMR) Memon MA, Khan S, Yunus RM, et al. Meta-analysis of laparoscopic and open distal gastrectomy for gastric carcinoma. Surg Endosc 2008;22:1781–9n Haverkamp L, Weijs TJ, van der Sluis PC, et al. Laparoscopic total gastrectom versus open total gastrectomy for cancer: a systematic review and metaanalysis Surg Endosc 2013;27:1509–20.
 Total gastrectomy( operative morbidity, technique of anastomosis) Ongoing trials in Japan,China,Korea(open versus laparoscopic surgery in early gastric cancer) Endoscopic Mucosal Resection (EMR) Memon MA, Khan S, Yunus RM, et al. Meta-analysis of laparoscopic and open distal gastrectomy for gastric carcinoma. Surg Endosc 2008;22:1781–9n. Haverkamp L, Weijs TJ, van der Sluis PC, et al. Laparoscopic total gastrectom versus open total gastrectomy for cancer: a systematic review and metaanalysis. . Surg Endosc 2013;27:1509–20.")
23
Endoscopic Mucosal Resection
Selection Criteria Histology/Differentiation Well and/or moderately differentiated adenocarcinoma Or papillary adenocarcinoma Confined to the mucosa Without evidence of venous or lymphatic involvement Size Less than 2 cm Ulcer status None grossly on endoscopy None microscopically No clinical evidence of lymph node involvement Gastric cancer: ESMO–ESSO–ESTRO Clinical Practice Guidelines for diagnosis, treatment and follow-up2014

24
Chemoradiation Therapy
Adjuvant Chemoradiation Therapy The North AmericanLandmark Intergroup 0116 Trial 556 randomized patients Vs. Surgery Alone 5-FU based regimen with concurrent XRT Improvement: Locoregional recurrence Median survival Overall survival Standard of care for stage IB and higher in the United States,

25
adjuvant chemoTherapy
6% absolute benefit for 5-FU-based chemotherapy compared with surgery alone(meta-analysis) Asian trials CLASSIC trial adjuvant capecitabine–oxaliplatin Vs. Surgery Alone Improvement: disease-free survival Overall survival in Europe remains limited: lack of benefit and routine use of perioperative chemotherapy Paoletti X, Oba K, Burzykowski T, et al. Benefit of adjuvant chemotherapy for resectable gastric cancer: a meta-analysis. JAMA 2010;303:1729–37 Sasako M, Sakuramoto S, Katai H, et al. Five-year outcomes of a randomized phase III trial comparing adjuvant chemotherapy with S-1 versus surgery alone in stage II or III gastric cancer. J Clin Oncol 2011;29:4387–93. for gastric cancer after D2 gastrectomy: final results from the CLASSIC trial Noh SH, Park SR, Yang HK, et al. Adjuvant capecitabine and oxaliplatin (XELOX). Ann Oncol 2013;24:iv
 Asian trials. CLASSIC trial. adjuvant capecitabine–oxaliplatin. Vs. Surgery Alone. Improvement: disease-free survival. Overall survival. in Europe. remains limited: lack of benefit and routine use of perioperative chemotherapy. Paoletti X, Oba K, Burzykowski T, et al. Benefit of adjuvant chemotherapy for resectable gastric cancer: a meta-analysis. JAMA 2010;303:1729–37. Sasako M, Sakuramoto S, Katai H, et al. Five-year outcomes of a randomized phase III trial comparing adjuvant chemotherapy with S-1 versus surgery. alone in stage II or III gastric cancer. J Clin Oncol 2011;29:4387–93. for gastric cancer after D2 gastrectomy: final results from the CLASSIC trial Noh SH, Park SR, Yang HK, et al. Adjuvant capecitabine and oxaliplatin (XELOX). Ann Oncol 2013;24:iv14. .")
26
Chemoradiation Therapy
Neoadjuvant Chemotherapy MAGIC Trial 503 randomized patients Vs. Surgery Alone epirubicin, cisplatin, continuous 5-FU Stage II or greater non-metastatic disease Post-op chemotherapy Improvements: Progression-free survival Overall survivalrate from 23% to 36%, with manageable toxic effects Neoadjuvant chemoradiation Therapy Ongoing Studies Currently useful in borderline resectable patients Cunningham D, Allum WH, Stenning SP, et al. Perioperative chemotherapyversus surgery alone for resectable gastroesophageal cancer. N Engl J Med2006

27
advanced/metastatic disease
Patients with stage IV disease should be considered for palliative Chemotherapy improves survival compared with best supportive care alone a small number of advanced disease patients may be deemed to be operable followin a good response to systemic therapy. Wagner AD, Grothe W, Haerting J, et al. Chemotherapy in advanced gastric cancer: a systematic review and meta-analysis based on aggregate data. J Clin Oncol 2006;24:2903–9. c

Similar presentations




FACS(hon) Professor of Surgery President ECCO - the European Cancer Organization Past-President European.>")

















