Download presentation
Presentation is loading. Please wait.

1
Efficiently dealing with new FDA information on drug safety Warnings, Shortages, Withdrawals – Oh My! Efficiently dealing with new FDA information on drug safety Karly Pippitt, MD Karen Gunning, PharmD University of Utah Family Medicine Residency

2
Ambulatory Safety: a lingering problemAmbulatory Safety: a lingering problem 1999 IOM report – not much happened 2011 JAMA editorial with 5 core aims to improve ambulatory safety: 1.Basic epidemiologic data needed to delineate problem. 2.Identify an early achievable goal 3.Engage patients and their families 4.Link to inpatient initiatives 5.Further develop practice based research networks to investigate/impact patient safety Wynia MK, Classen DC. Improving ambulatory patient safety JAMA 2011; 306:2504 - 2505

3
Objectives At the conclusion of the discussion, participants will be able to: Determine barriers to communication and strategies to overcome barriers in developing alternative drug therapy plans for patients after warnings, shortages, and/or withdrawals. Given an example drug safety warning, medication market withdrawal, or drug shortage develop a plan of action for dissemination of information to provider and patients.

4
Shortages – What the Heck? Drug shortages 2001 – 2011 Source: University of Utah Drug Information Service http://www.washingtonpost.com/politics/obama-issues-executive-order-aimed-at-curbing-drug-shortages/2011/10/31/gIQAPor4ZM_story.html

5
How to find out what is on shortage... http://www.fda.gov/Drugs/DrugSafety/DrugShortages/de fault.htm http://www.fda.gov/Drugs/DrugSafety/DrugShortages/de fault.htm http://www.ashp.org/shortages http://www.ashp.org/shortages

6
Other information sourcesOther information sources Local pharmacies Wholesaler or higher level issue Acute or chronic? Reason for shortage?

7
Market Withdrawals: Here today, gone tomorrow Propoxyphene Midrin Rosiglitazone

8
Key safety issues with market withdrawals What is the most appropriate alternative for the individual patient? Opportunity for medication discontinuation? Optimization of therapy? Re-evaluation of indication Proactive vs reactive?

9
Warnings and precautions and scary things – oh my! Simvastatin Citalopram Pediatric acetaminophen liquid preparations http://www.fda.gov/Safety/MedWatch/ucm168422.htm

10
Simvastatin chaosSimvastatin chaos Do not use Simvastatin 80 mg in new patients Continue in pts already on it if they have been taking it > 1 year Risk: myopathy/rhabdo Seems to be associated with a genetic variant in simvastatin handling that increases simvastatin concentrations. So – if you need more than 40 mg of simvastatin – switch to: Atorvastatin 40 mg daily OR Rosuvastatin 10 mg – 20 mg daily BUT – the drug interactions mess... www.fda.gov

11
Simvastatin Dosing Limitation WarningsSimvastatin Dosing Limitation Warnings DrugSimvastatin max dose Amiodarone20 mg Amlodipine20 mg Ranolazine20 mg Diltiazem 10 mg Verapamil 10 mg ____________________________________ Contraindicated drugs: Itraconazole, Ketoconazole,Posaconazole,Erythromycin, Clarithromycin,Telithromycin,HIV protease inhibitors, Nefazodone, Gemfibrozil, Cyclosporine, Danazol www.fda.gov

12
FDA - CitalopramFDA - Citalopram Concern: Dose-dependent association between citalopram use and increased QT interval and arrhythmias Doses > 40 mg not associated with clinical benefit in trials – so don’t use Risk Factors: Patients with existing heart conditions, such as congestive heart failure or bradyarrhythmias, or those with hypokalemia or hypomagnesemia are especially at risk for this effect www.fda.gov

13
FDA - CitalopramFDA - Citalopram No more than 20 mg in patients with hepatic impairment or in patients greater than 60 years old Do not use citalopram in patients with congenital long QT syndrome Do not use with persistent QTc > 500 msec www.fda.gov

14
Simvastatin 80 mg Simvastatin with contraindicated medications Citalopram Our Plan of AttackOur Plan of Attack

16
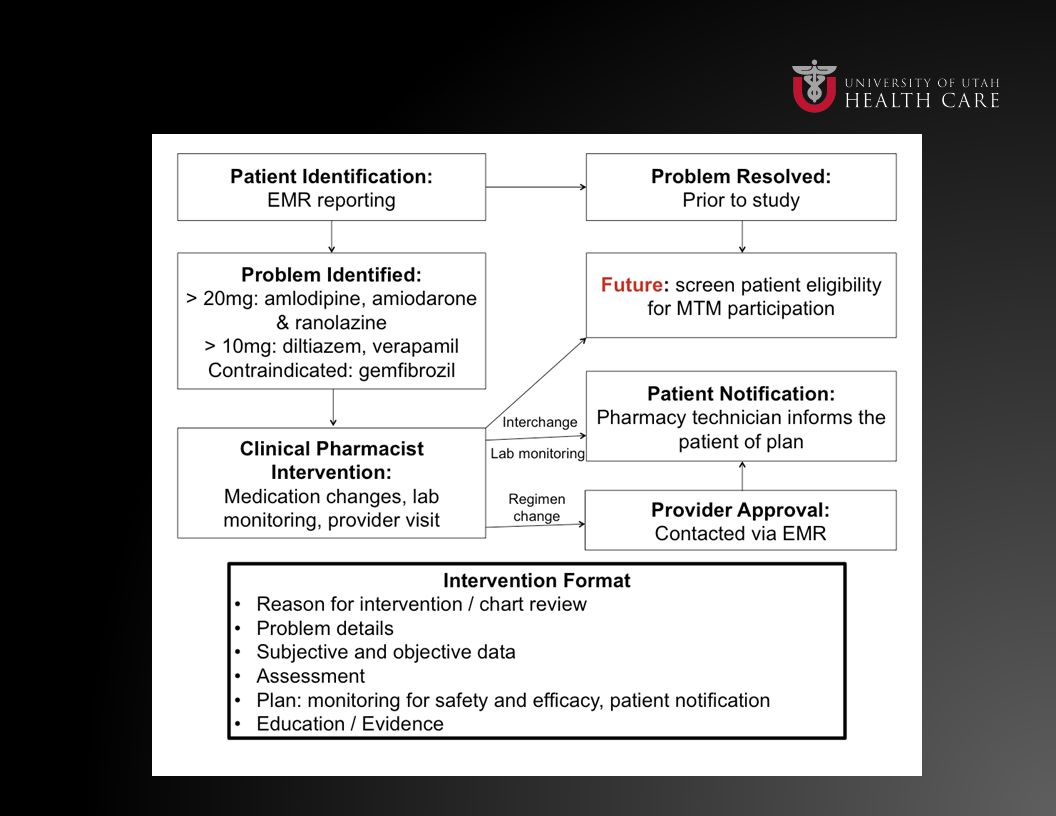
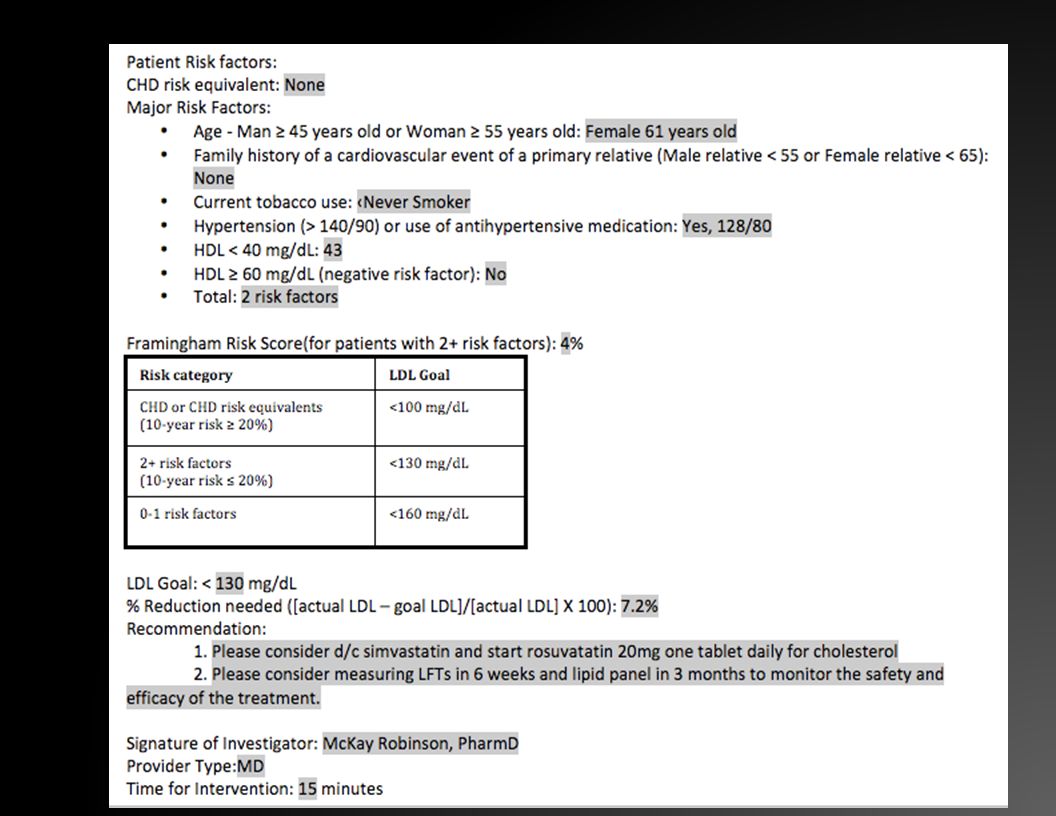
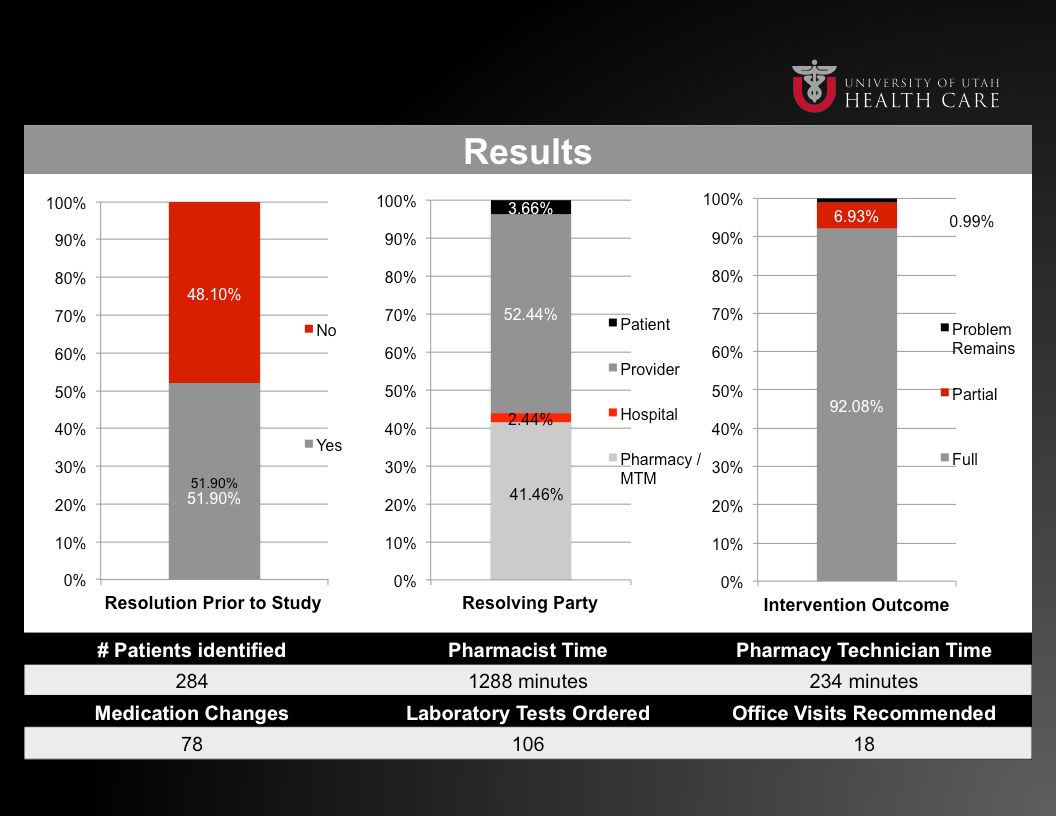
Our attempt - SimvastatinOur attempt - Simvastatin

19
Simvastatin – Residency ClinicSimvastatin – Residency Clinic Following initial warning re: 80mg dose, data pull 3 rd year FM resident on pharmacotherapy rotation Reviewed charts and contacted providers 2 days, ~4 hours Clinical Pharmacist and RNs called patients and pharmacies

20
Simvastatin – Residency ClinicSimvastatin – Residency Clinic ~6 months later, 4 th year FM honors student Simvastain 80 mg Simvastatin + contraindicated medications Take home point: continuous process, not single point in time

21
Our try CitalopramOur try Citalopram Patient <60 years of age on citalopram 60 mg Symptoms controlled and pt on dose for > 4 months Decrease citalopram dose to 40 mg daily and evaluate response in 4 weeks Symptoms controlled, but on dose for < 4 months Switch to another high dose SSRI* and evaluate in 4 weeks Symptoms uncontrolled Select an agent from another class: SNRI $ or bupropion # - titrate dose and evaluate in 2 weeks

22
*SSRI high dose options (can switch over directly, no cross-taper needed) Sertraline: 150-200 mg daily start at 50 mg/day and increase dose by 50 mg daily every week Fluoxetine: 60-80 mg daily, start at 20 mg/day and increase dose by 20 mg daily every week Paroxetine: 40-50 mg daily, start at 20 mg/day and increase by 10 mg daily every week Can switch over directly, no cross-taper needed $SNRI switch options (can consider cross-tapering dose of citalopram during initiation but not necessary) Venlafaxine: start at 75 mg daily and titrate up by 75 mg daily weekly to target dose of 150-225 mg/day Duloxetine: start at 30 mg daily, increase to target dose of 60 mg/day after 1 week #Bupropion (consider cross-taper of citalopram with initiation of bupropion): Immediate release: start at 100 mg BID and increase to 100 mg TID after 1 week Sustained release: start at 100 mg daily, titrate up to 300 mg/day in divided doses after 1 week Citalopram
 Sertraline: mg daily start at 50 mg/day and increase dose by 50 mg daily every week Fluoxetine: mg daily, start at 20 mg/day and increase dose by 20 mg daily every week Paroxetine: mg daily, start at 20 mg/day and increase by 10 mg daily every week Can switch over directly, no cross-taper needed $SNRI switch options (can consider cross-tapering dose of citalopram during initiation but not necessary) Venlafaxine: start at 75 mg daily and titrate up by 75 mg daily weekly to target dose of mg/day Duloxetine: start at 30 mg daily, increase to target dose of 60 mg/day after 1 week #Bupropion (consider cross-taper of citalopram with initiation of bupropion): Immediate release: start at 100 mg BID and increase to 100 mg TID after 1 week Sustained release: start at 100 mg daily, titrate up to 300 mg/day in divided doses after 1 week Citalopram")
23
Citalopram Patient >60 years of age on citalopram 30-60 mg Symptoms controlled and pt on dose for > 4 months Taper citalopram dose to 20 mg daily over 1-3 weeks, evaluate response in 4 weeks Symptoms controlled, but on dose for < 4 months Switch to another high dose SSRI* and evaluate in 4 weeks Symtptoms uncontrolled Select an agent from another class: SNRI $ or bupropion # - titrate dose and evaluate in 2 weeks

24
*SSRI high dose options (can switch over directly, no cross-taper needed)- Sertraline: 100-200 mg daily start 25 mg/day and increase dose by 25 mg daily every week Fluoxetine: 60-80 mg daily, start 10-20 mg/day and increase dose by 10-20 mg daily weekly as tolerated Paroxetine: 40 mg daily, start at 10 mg/day and increase by 10 mg daily every week $SNRI switch options (can consider cross-tapering dose of citalopram during initiation but not necessary) Venlafaxine: start at 37.5-75 mg daily and titrate up by 37.5-75 mg daily weekly to target dose of 150-225 mg/day Duloxetine: start at 20-30 mg daily, increase to target dose of 60 mg/day after 1 week #Bupropion (consider cross-taper of citalopram with initiation of bupropion): Immediate release: start at 100 mg BID and increase to 100 mg TID Sustained release: start at 100 mg daily, titrate up to 300 mg/day in divided doses Citalopram
- Sertraline: mg daily start 25 mg/day and increase dose by 25 mg daily every week Fluoxetine: mg daily, start mg/day and increase dose by mg daily weekly as tolerated Paroxetine: 40 mg daily, start at 10 mg/day and increase by 10 mg daily every week $SNRI switch options (can consider cross-tapering dose of citalopram during initiation but not necessary) Venlafaxine: start at mg daily and titrate up by mg daily weekly to target dose of mg/day Duloxetine: start at mg daily, increase to target dose of 60 mg/day after 1 week #Bupropion (consider cross-taper of citalopram with initiation of bupropion): Immediate release: start at 100 mg BID and increase to 100 mg TID Sustained release: start at 100 mg daily, titrate up to 300 mg/day in divided doses Citalopram")
25
Acetaminophen pediatric liquid: A giant mess ISSUE: The FDA has requested manufacturers change to a standard and single acetaminophen concentration of 160 mg / 5 ml to reduce overdoses from the use of the 80 mg / 0.8 mL infant drops PROBLEM: Some manufacturers complied – some did not – creating a mess at the drugstore

26
Acetaminophen pediatric liquid: A giant mess http://www.fda.gov/ForConsumers/ConsumerUpdates/ucm284563.htm?utm_campaign=Google2&utm_ source=fdaSearch&utm_medium=website&utm_term=acetaminophen

27
How could you approach this warning in your system? With people around you – spend the next few minutes discussing how this might affect your practice, and how you can be proactive to maintain patient safety. Ideas?

28
Acknowledgments McKay Robinson, PharmD Lee Audd, MSIV Russell Anderson, MD (FM resident) Breanne Chipman, PharmD student
 Breanne Chipman, PharmD student")
Similar presentations


>")
 or citalopram 20 mg (10 -60 mg) Exercise, Pt education: response expectations, followup ~ 1.>")





 Tablets Risk-Benefit Issues Victor F. C. Raczkowski, M.D. Director, Division of Gastrointestinal and Coagulation Drug Products.>")









