Download presentation
Presentation is loading. Please wait.

1
E VIDENCE - BASED APPROACH TO THE MANAGEMENT OF ADHD STFM / FMEC 2013 Saturday, Nov. 2 nd NE Regional Meeting Sutton Hamilton MD Inspira Family Medicine Residency

2
ADHD What does research tell us about effective treatment strategies? What does research tell us about how to best evaluate children who may have ADHD?

3
ADHD – CORE SYMPTOMS Inattention. Nearly universal. Hyperactivity. AKA, “behavioral disinhibition.” Impulsivity.

4
ADHD Almost certainly best considered “dimensional” (not “categorical.”) That is – we all have some degree of inattention, hyperactivity and impulsivity. The “disease” state depends on the degree of each and the impairment generated.

5
ADHD ADHD is highly heritable, with about 70% of individuals with AHDH having a parent who meets diagnostic criteria. Genetics play a large role and details of inheritance are slowly being elucidated.

6
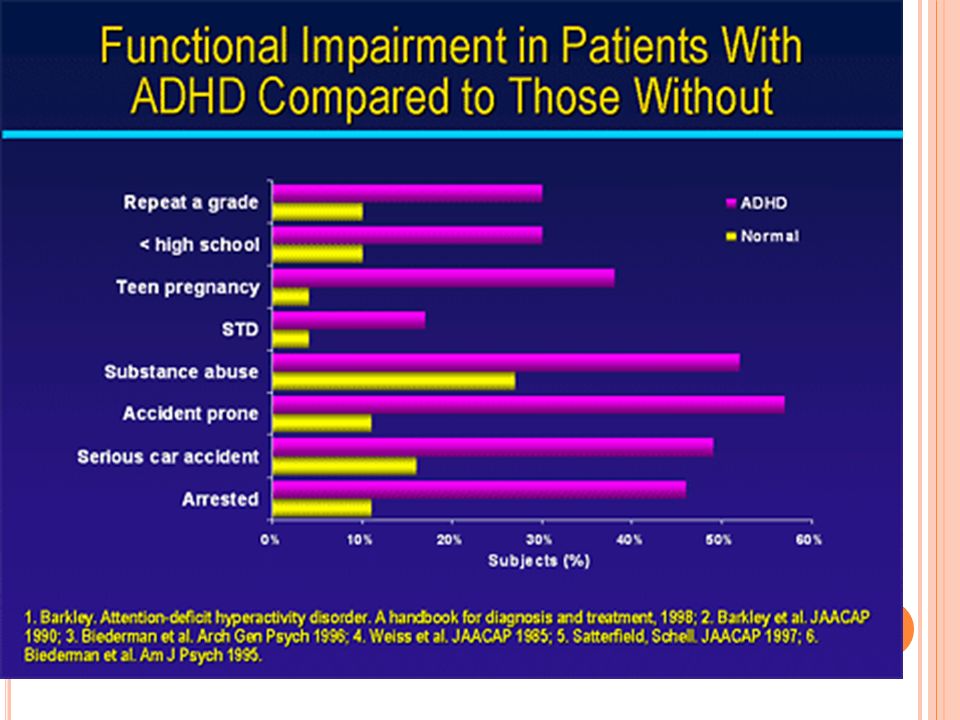
ADHD AND LIFE EXPECTANCY Life expectancy is decreased in individuals with ADHD through Increased accident proneness (youth) Speeding and auto accidents (adolescence/young adulthood) Crime Suicide attempts Use and abuse of substances (alcohol, tobacco) Increased risk-taking behavior (generally)
 Speeding and auto accidents (adolescence/young adulthood) Crime Suicide attempts Use and abuse of substances (alcohol, tobacco) Increased risk-taking behavior (generally)")
8
P REVALENCE OF C OMORBID D ISORDERS FOR C HILDREN WITH ADHD VS. T HOSE W ITHOUT (N=61,779) Learning Disability: 46.1% vs. 5.3% Conduct Disorder: 27.4% vs. 1.8% Anxiety : 17.8% vs. 2.1% Depression : 13.9% vs. 1,4%
 Learning Disability: 46.1% vs. 5.3% Conduct Disorder: 27.4% vs. 1.8% Anxiety : 17.8% vs. 2.1% Depression : 13.9% vs. 1,4%.")
9
O UR APPROACH Assessment: ADHD: NICHQ Vanderbilt Affect: Pediatric Symptom Checklist Academics: teacher contact, NJ ASK

10
A SSESSMENT : ACCURACY OF DIAGNOSIS, DIFFERENTIAL DIAGNOSIS, CO - EXISTING CONDITIONS Use a standardized, validated instrument that seeks information from at least 2 sources. NICHQ Vanderbilt Assessment Scale SNAP IV ADHD Rating Scale IV

11
A SSESSMENT : V ANDERBILT A SSESSMENT S CALE Available free for download. Good data on its accuracy as a diagnostic instrument. Seeks information from parent, teacher. Includes follow-up forms to give “objective” information about the child’s progress, response to medication.

13
P EDIATRIC S YMPTOM C HECKLIST - PSC Anxiety and depression are common in children who present for assessment for ADHD. PSC has been extensively researched. Free for download. Some propose using the PSC at every visit! Can be completed by the parent or the adolescent.

14
Jellinek M 1999 Pediatrics: 21,065 children screened at 395 practices with PSC Demonstrated the feasibility in primary care

15
A CADEMIC INFORMATION Goals: Judge degree of impairment Identify weakness or areas of strength Initiate processes for the identification of learning disabilities ( typically = reading disability, AKA dyslexia )
")
16
A CADEMIC I NFORMATION Sources Report Cards State-based standardized testing Verbal report from teacher IEP?

17
T REATMENT The Multimodal treatment Study of Children Response for Children with Attention- Deficit/Hyperactivity Disorder. N=579 children randomized to four groups Community Care Behavioral Treatment only Medication Combined care (medication + behavioral)
.")
19
W HAT CAN WE CONCLUDE FROM THE MTA? MTA-delivered care produced significantly greater improvements compared with “community care.”

21
H OW DO WE BEST EMULATE THE CARE GIVEN IN THE MTA? MTA patients were treated at significantly higher doses of MPH ( 32.8mg/day vs. 18.7mg/day) MTA visits were longer (30 min. vs. 18 min) and much more frequent ( 8.8 visits/year vs. 2.3 visits /year) MTA care included monthly contact with teachers to guide medication adjustments
 MTA visits were longer (30 min. vs. 18 min) and much more frequent ( 8.8 visits/year vs. 2.3 visits /year) MTA care included monthly contact with teachers to guide medication adjustments.")
22
O THER OBSERVATIONS FROM THE MTA THAT SHOULD SHAPE OUR PRACTICE In general, behavioral management added very little to outcomes. That said, some sub-groups benefited significantly from behavioral intervention. Subjects with anxiety ( about 1/3 ) benefitted from combined care Subjects with ODD and Conduct disorder + anxiety with pronounced benefit of combined care.
 benefitted from combined care Subjects with ODD and Conduct disorder + anxiety with pronounced benefit of combined care..")
23
MTA: M EDICATION USE AT 36 MONTHS Behavioral: 14% 45% Combined: 91% 91% Community 60% 62%

24
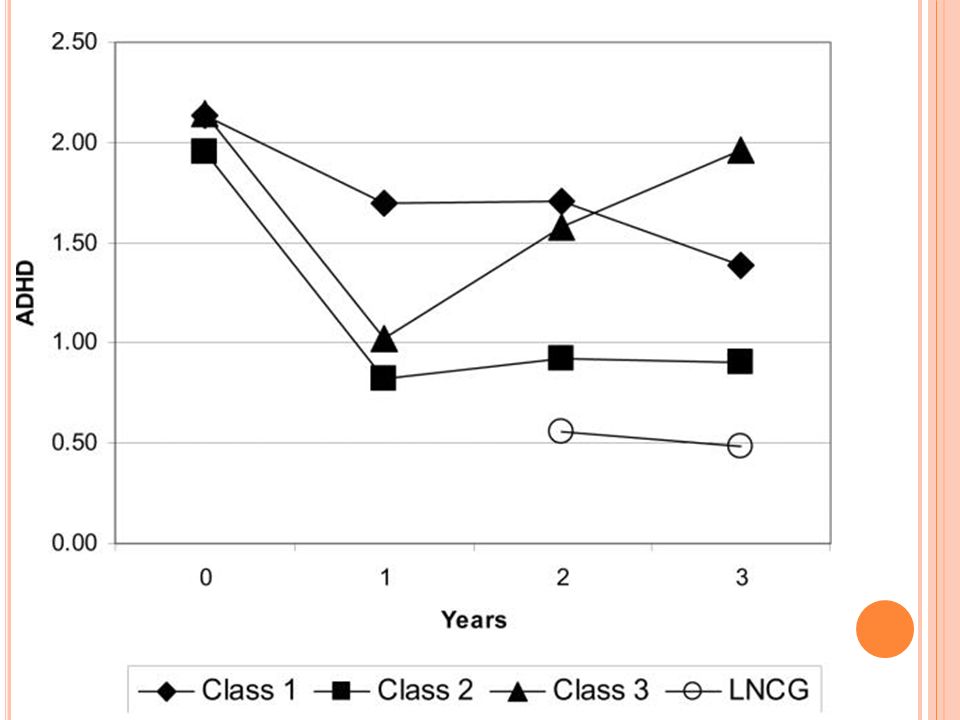
MTA AT 24 MONTHS, 36 MONTHS AND AT 8 YEARS “ by 36 months, the earlier advantage of having had 14 months of the medication algorithm was no longer apparent, possibly due to age-related decline in ADHD symptoms, changes in medication management intensity.” At 36 months an onward, there was no detectible effect of original group assignment. Instead, ADHD severity and trajectory predicted outcomes

25
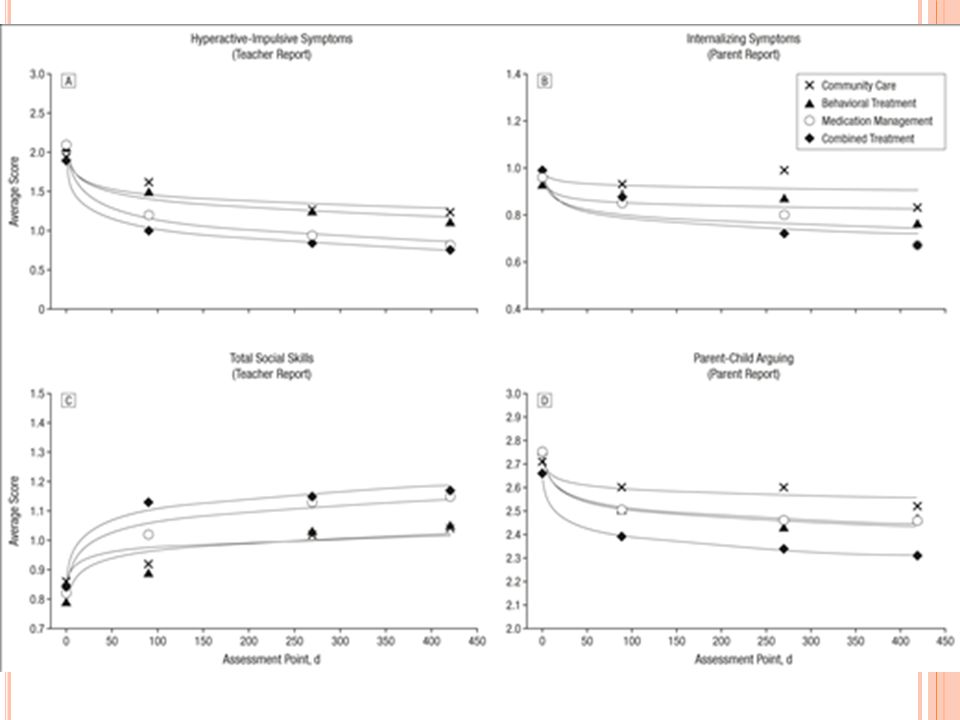
O NE MORE SLIDE ABOUT GENERALIZATIONS FROM THE MTA When outcomes besides ADHD were examined, treatments that included behavioral therapy did better than those that did not. Reporting… less oppositional/aggressive symptoms Less internalizing symptoms Better social skills (teacher reported) Better parent-teacher relations Better reading achievement. Higher parent and teacher satisfaction
 Better parent-teacher relations Better reading achievement. Higher parent and teacher satisfaction.")
26
T EN TAKE - HOME POINTS 1. Use a validated instrument to begin your assessment for ADHD (e.g. Vanderbilt) 2. Use the PSC to screen for affective disorders. 3. Investigate academic performance, particularly reading. Push for evaluation for additional services if suspicion for reading disability.
 2. Use the PSC to screen for affective disorders. 3. Investigate academic performance, particularly reading. Push for evaluation for additional services if suspicion for reading disability..")
27
T EN TAKE - HOME POINTS 4.The MTA demonstrated that intensive medical management produced substantially greater improvement in ADHD behavior than did “community care. 5.Push the dose of MPH, monitoring carefully for side effects and for symptom resolution. 6.See your patients on order of 8x / year to generate response rates like that seen in the MTA.

29
T EN TAKE - HOME POINTS Know that the effectiveness of medical therapy for ADHD beyond 14 months is not known. Children in the combined or intensive medical management group were indistinguishable at 36 months after the study’s completion.

31
Select References: MTA Cooperative Group. A 14-Month Randomized Clinical Trial of Treatment Strategies for Attention- Deficit/Hyperactivity Disorder. Arch Gen Psych 1999; 56: 1073-1086 Jensen PS, Arnold LE, Swanson JM, Vitiello B. et. al. 3-Year Follow-up of the NIMH MTA Study. J Am Acad Child Adol Psych 2007; 46:989-1002 The MTA at 8 Years: Prospective Follow-up of Children Treated for Combined-Type ADHD in a Multisite Study. J Am Acad Chlid Adol Psych 2009; 48:484-500

Similar presentations




 NIMH-funded R01 New York University – Howard Abikoff, PI.>")

 Psychosocial Interventions.>")















