Download presentation
Presentation is loading. Please wait.

1
Immune-deficiencies for batch 17-MBBS Yr 1 Dr. P. K. Rajesh. M.D

2
Primary immunodeficiency disease: PIDD-A disorder caused by an inherited flaw in the immune system that increases the susceptibility to infections. Note Secondary or acquired immune deficiency diseases are caused by infectious (eg-HIV- AIDS), chemical or radiological agents. Secondary-to another cause Dr.P.K.Rajesh.M.D
, chemical or radiological agents. Secondary-to another cause Dr.P.K.Rajesh.M.D.")
3
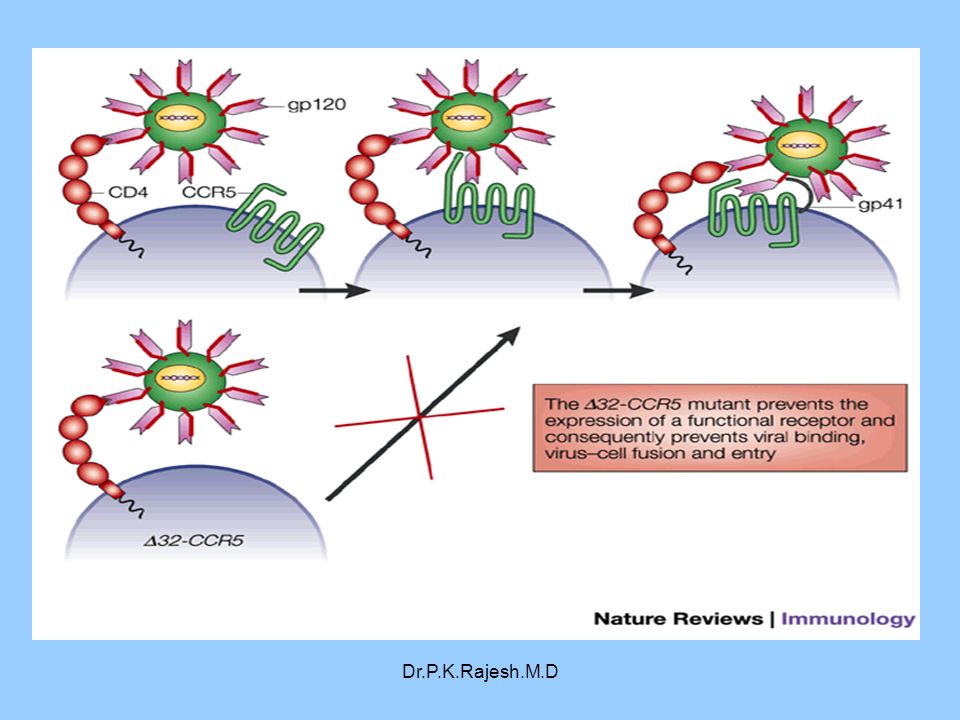
Lecture 10: Immune-deficiencies OBJECTIVES: The objectives of this lecture are to define primary and secondary immunodeficiency classify immunodeficiencies according to the specific immune component deficient discuss the role of CD4 receptors and chemokines in AIDS introduce the conditions that can lead to opportunistic infection

4
GOOD TEACHING IS ONE-FOURTH PREPARATION AND THREE- FOURTHS PURE THEATRE. GAIL GODWIN GAIL GODWIN Education is what survives when what has been learned has been forgotten. B. F. SkinnerB. F. Skinner An education isn't how much you have committed to memory, or even how much you know. It's being able to differentiate between what you know and what you don't. Anatole FranceAnatole France Dr.P.K.Rajesh.M.D Medical education is all about being able to differentiate between what you NEED TO know and what you don't NEED TO KNOW at each phase of study. PERUMBILAVIL RAJESH U R ADV2 STIC 2OUTCOMES

5
Learning outcomes At the end of the lecture, student should be able to: define to distinguish between primary and secondary immunodeficiency. classify immunodeficiency diseases according to the specific immune component. discuss the role of CD4 in AIDS. identify the factors that lead to opportunistic infection. Outcomes 1 and 2 most important for this lecture Outcomes 3 and 4 introduced in this lecture- more will feature later

6
Dr.P.K.Rajesh.M.D Primary immunodeficiency 1.Disorders of Specific Immunity B cell defects Cellular immunodeficiency Combined ID 2.Disorders of complement 3.Disorders of Phagocytosis

7
Humoral / B-cell Defects

8
Dr.P.K.Rajesh.M.D B cell defects Bruton’s X-linked agammaglobulinemia Transient hypogamma, infancy Common variable ID Selective Immunoglobulin def ID with Hyper Ig M

9
Dr.P.K.Rajesh.M.D

10
. Cell-Mediated/T cell Immunity

11
Dr.P.K.Rajesh.M.D

12
Cellular ID Thymic hypoplasia (Di George’s syndrome) Chr.mucocutaneous candidiasis
 Chr.mucocutaneous candidiasis")
13
Dr.P.K.Rajesh.M.D Nezelof syndrome ( Cellular ID with abnormal Ig synt) Wiskott-Aldrich Syndrome Combined ID
 Wiskott-Aldrich Syndrome Combined ID")
14
Phagocytic Disorders

15
Dr.P.K.Rajesh.M.D

16
Disorders of Phagocytosis Neutropenia Lazy leucocyte syndrome Job’s syndrome Leucocyte adhesion deficiency Myeloperoxidase deficiency Chronic granulomatous disease –Defect in NADPH oxidase –Reduced H202 production Chediak Higashi syndrome Less number of phagocytes Severely Impaired chemotaxis Reduced chemotactic response Reduced migration into tissues Reduced ability to store materials in lysosomes and or release

17
Complement Disorders

18
Revisited, when u do haematology

19
Use this when you revise

20
Dr.P.K.Rajesh.M.D

21
Don’t mug this up- lecture on microbes and immunity coming up later

22
Dr.P.K.Rajesh.M.D MBBS Batch 13 reported 2 cases of Di George from SP in one year

23
Case Presentation D. George is a 2 year old male brought in by his parents Wiskott and Aldrich because of concerns about recurrent infections. They state he has been sick many times over the last two years. He has been in the hospital twice with some sort of infection. He has also had frequent upper respiratory infections and has had Otitis Media 7 times in the last two years.

24
Case contd The parents of D. George are very concerned. They wonder is there something wrong with him. Is it normal to have this many infections? Could there be something wrong with his immune system? How are you going to figure this out? Does he need testing?

25
Diagnostic Work Up Antibody Defects –Quantitative - Immunoglobulin levels –Functional - Antibody Titers to immunizations T cell –Quantitative – CBC, Abs lymphocyte count –Functional – Skin tests for antigens (Mumps, candida, etc.) Phagocyte –Quantitative – CBC, Abs neutrophil count –Functional – NBT test Complement –Quantitative – C3, C4 –Functional – CH50
 Phagocyte –Quantitative – CBC, Abs neutrophil count –Functional – NBT test Complement –Quantitative – C3, C4 –Functional – CH50")
26
Prevalence Most children with recurrent infections don’t have primary immunodeficiency –90% have secondary cause When immunodeficiency occurs –Antibody/B cell issue 54% –Combined B/T cell 23% –Other deficiencies rare (complement deficiency is only 2%) Over 100 immunodeficiency syndromes have been described.
 Over 100 immunodeficiency syndromes have been described.")
27
Distribution of Immunodeficiencies

28
Dr.P.K.Rajesh.M.D

30
Secondary ID Immunosuppressive therapy Corticosteroids Radiotherapy Diabetes mellitus Prolonged antibiotic therapy HIV-AIDS

31
Dr.P.K.Rajesh.M.D References Medical Immunology. Richard.P.Stites NMS Immunology Self directed learning 1)How does HIV infection result in AIDS? 2)How do doctors manage patients with these disorders? (The principles) 3)What if these disorders are not diagnosed and these children are vaccinated?
How does HIV infection result in AIDS. 2)How do doctors manage patients with these disorders. (The principles) 3)What if these disorders are not diagnosed and these children are vaccinated .")
32
Dr.P.K.Rajesh.M.D Email rajesh.perumbilavil@gmail.com

Similar presentations
















 Soheila Alyasin M.D. AssOCIAT Professor of Pediatrics Division of Immunology and Allergy.>")


