Download presentation
Presentation is loading. Please wait.

1
CHRONIC BLISTERING DERMATOSES Özlem Akın, M.D. Yeditepe University Hospital Department of Dermatology

2
CHRONIC BLISTERING DERMATOSES In the noninherited chronic blistering (vesicular or bullous) dermatoses, the cause of blistering is an autoimmune reaction Pattern od immunofluorescence is critical in establishing the diagnosis Antibodies are bound in perilesional skin and at the site of the earliest lesions Lesional skin often fails to demonstrate deposits, and lower extremity skin may be prone to false-negative reactions Salt-split skin preperations are usefull in determining the site of deposition of the antibodies A 1 M solution of NaCl predictably splits skin at the level of the lamina lucida Localization of immune deposits to the roof or floor of this spilt is diagnostically usefull Immunoprecipitation and immunoblotting have helped to define the molecular targets of the antibodies
 dermatoses, the cause of blistering is an autoimmune reaction Pattern od immunofluorescence is critical in establishing the diagnosis Antibodies are bound in perilesional skin and at the site of the earliest lesions Lesional skin often fails to demonstrate deposits, and lower extremity skin may be prone to false-negative reactions Salt-split skin preperations are usefull in determining the site of deposition of the antibodies A 1 M solution of NaCl predictably splits skin at the level of the lamina lucida Localization of immune deposits to the roof or floor of this spilt is diagnostically usefull Immunoprecipitation and immunoblotting have helped to define the molecular targets of the antibodies")
3
Pemphigus Vulgaris Characterized by mucosal erosions, and thin- walled, relatively flaccid, easily ruptured bullae that appear on apparently normal skin and mucous membranes or on erythematous bases The fluid in the bullae is clear at first but may become hemorrhagic or even seropurulent The bullae rupture to form erotions Denuded areas soon become partially or totally covered with crusts that have little or no tendency to heal When they finally heal, lesions often leave hyperpigmented patches with no scarring M=F Usually in 5. or 6. decades

4
Pemphigus Vulgaris Usually appears first in the mouth (60% of cases) or at the site of a burn or other skin injury Other common sites include the groin, scalp, face, neck, axillae, and genitals Nikolsky sign is present (intact epidermis shearing away from the underlying dermis leaving a moist surface) Sign is elicited by slight pressure, twisting or rubbing The “bulla-spread phenomenon” (Asboe-Hansen sign) is elicited by pressure on an intact bulla, gently forcing the fluid to spread under the adjacent skin
 or at the site of a burn or other skin injury Other common sites include the groin, scalp, face, neck, axillae, and genitals Nikolsky sign is present (intact epidermis shearing away from the underlying dermis leaving a moist surface) Sign is elicited by slight pressure, twisting or rubbing The bulla-spread phenomenon (Asboe-Hansen sign) is elicited by pressure on an intact bulla, gently forcing the fluid to spread under the adjacent skin")
5
Pemphigus Vulgaris Short-lived bullae quickly rupture to involve most of the mucosa with painful erosions The lesions extend onto the lips and form heavy, fissured crusts on the vermilion Involvement of the throat produces hoarseness and difficulty in swallowing The mouth odor is offensiveness Esophagus may be involved, and sloughing of the entire lining in the form of a cast (esophagitis dissecans superficialis) may occur, evenwhen the cutaneous disease appears to be well controlled The conjunctiva, nasal mucosa, vagina, penis, and anus may also be involved Widespread cutaneous disease may cause death through sepsis or fluid and electrolyte imbalance
 may occur, evenwhen the cutaneous disease appears to be well controlled The conjunctiva, nasal mucosa, vagina, penis, and anus may also be involved Widespread cutaneous disease may cause death through sepsis or fluid and electrolyte imbalance")
7
Pemphigus Vulgaris Diagnosis Histology Immunofluorescence pattern of perilesional skin Indirect ımmunofluorescence (IIF) testing of serum Enzyme-linked immunosorbent assay testing for anti-desmoglein (Dsg)1 and –Dsg3 autoantibodies As in other autoimmune diseases, specific antibodies may be present in relatives of patients who do not manifest any signs of diasease
 testing of serum Enzyme-linked immunosorbent assay testing for anti-desmoglein (Dsg)1 and –Dsg3 autoantibodies As in other autoimmune diseases, specific antibodies may be present in relatives of patients who do not manifest any signs of diasease")
8
Pemphigus Vulgaris Histopathology Suprabasilar acantholysis with intraepidermal blister formation An Asboe-Hansen modification of the Nikolsky test may be used to extend the bulla beyond its original margin to where secondary regenerative changes have not taken place DIF demonstrates intercellular IgG in perilesional skin C3 may also be present Staining is uniform, not granular IIF shows a similar pattern of staining Positive tests may be confirmed with ELISA assays for the antibody

9
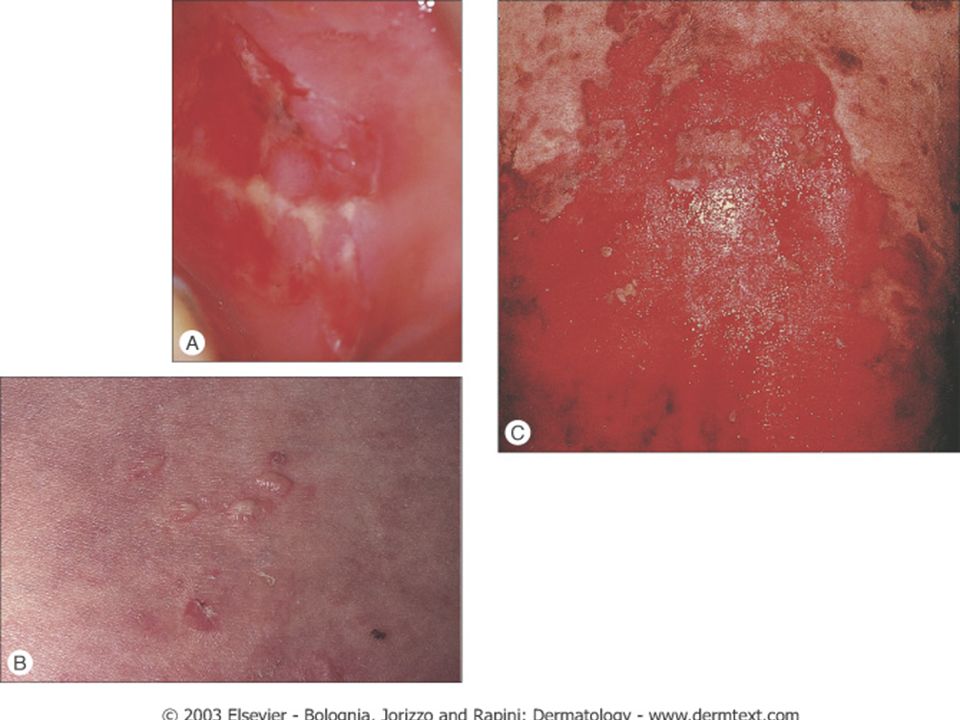
Histology of pemphigus vulgaris. A Blisters in the skin show suprabasilar acantholysis with a few acantholytic cells in the blister cavity. B The border of a blister on the buccal mucosa shows intraepithelial separation in the lower part of the mucosal epithelia.

10
Direct Immunofluorescence (DIF)
")
11
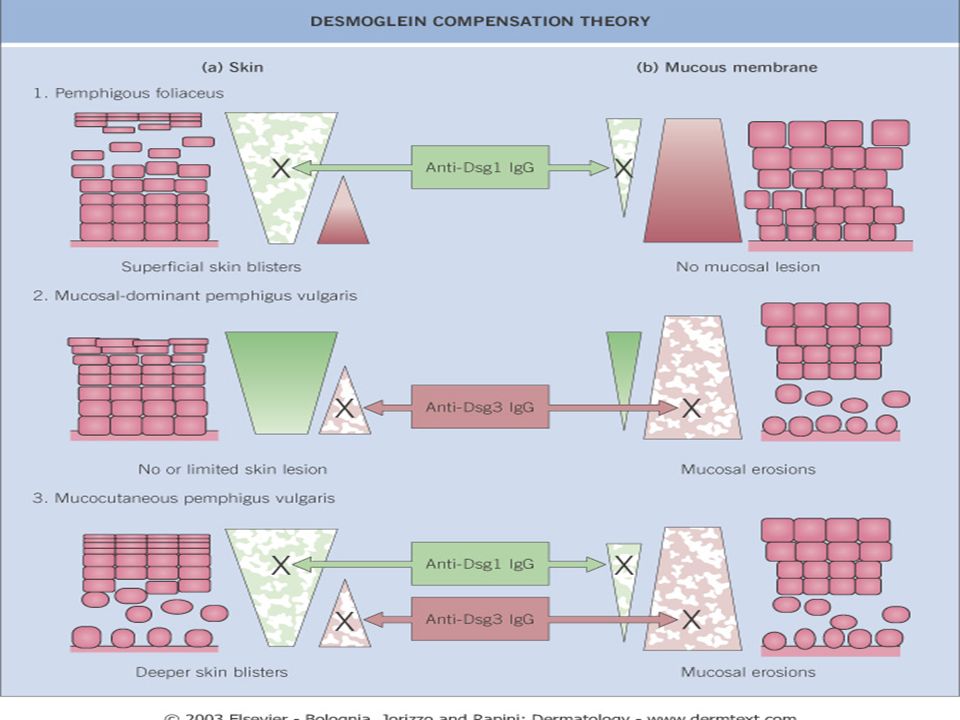
Pemphigus Vulgaris Antibodies in PV are most commonly directed against Dsg3 Presence of antibodies to both Dsg1 and Dsg3 correlates with mucocutaneous disease If autoantibodies are only directed against Dsg3, mucosal lesions predominate

13
Pemphigus Vulgaris Treatment Prednisone Azathioprine Mycophenolate mofetil Cyclophosphamide Methotrexate IVIG Plasmapheresis

14
Bullous Pemfigoid Characterized by large, tense, subepidermal bullae with a predilection for the groin, axillae, trunk, thighs and flexor surfaces of the forearms Key features distinguishing BP from other immunobullous diseases: subepidermal seperation at the dermoepidermal junction, an inflamatory cell infiltrate that tends to be rich in eosinophils, antibodies directed against two hemidesmosomal antigens, BP230 and BP18

15
Bullous Pemfigoid After the bullae rupture, large denuded areas are seen, but bullae and denuded areas do not tend to increase in size as they do in PV Instead, the denuded areas show a tendency to to heal spontaneously In addition to bullae, there often are erythematous patches and urticarial plaques, with a tendency to central clearing These patches and plaques may be present without bullae early in the course of the disease

16
Bullous Pemfigoid May begin at a localized site May remain localized throughout the course of the disease or eventuate in generalized pemfigoid Variants of BP: Dyshidrosiform pemfigoid Vulvar pemfigoid Vesicular pemfigoid Pemfigoid nodularis Pemfigoid vegetans Erythrodermic pemfigoid Nonbullous variant

17
Bullous Pemfigoid Incidence of oral involvement is about 20%, but involvement of the pharynx, larynx, nasal mucosa, vulva, urethra, and the eye is rare Occurs most frequently in the elderly The age of onset averages 65 to 75 years

18
Bullous pemphigoid. A Urticarial, infiltrated, and annular erythematous plaques on the trunk and abdomen. B Generalized eruption with blisters and erosions eroded and crusted lesions in the same patient later in the course of the disease.

19
A Excoriated eczematous lesions on the forearm. B Confluent plaques with tense blisters in the inguinal area and inner aspect of the legs in the same patient.

21
Childhood bullous pemphigoid. A Generalized bullous and crusted lesions. B Vulvar bullous pemphigoid.

22
Bullous Pemfigoid BP has occasionally been reported to be associated with other diseases DM RA Pemfigus foliaceus Dermatomyositis Ulcerative colitis Myastenia gravis Thymoma Drugs that induce BP: Penicillamine Furosemide Captopril Penicillin Sulfasalazine Nalidixic acid enalapril

23
Bullous Pemfigoid Histopathology: Subepidermal bullae Absence of acantholysis Superficial dermal infiltrate containing many eosinophils DIF: continious lineer basement membrane zone IgG (80%) and/or C3 (100%) deposition IgA and IgM are occasionally present All histopathologic features present in BP may also be seen in epidermolysis bullosa acquisita (EBA); therefore, immunofluorescence testing on salt-split skin is required to differentiate EBA from BP. C3 deposition nearly always present in BP, where it may be absent in EBA. Type IV collagen mapping in BP localizes to the base of the blister. In EBA it stains the roof.

24
Subepidermal blister formation and an inflammatory infiltrate composed of neutrophils and eosinophils in the dermis and bulla cavity, by light microscopy. Inset, at higher power, shows the infiltrate rich in eosinophils (hematoxylin–eosin stain).
..")
25
A DIF of perilesional skin demonstrating linear continuous deposits of IgG along the epidermal basement membrane zone (arrow). The same pattern of labeling is observed in cicatricial pemphigoid and EBA. B IIF utilizing salt-split normal human skin as a substrate. Patient's IgG autoantibodies are bound to the epidermal side (roof) of the split (arrow). The level of the artificial separation is indicated by asterisk. Cell nuclei are stained blue. The same pattern of labeling is observed in a subset of patients with cicatricial pemphigoid.
 of the split (arrow). The level of the artificial separation is indicated by asterisk. Cell nuclei are stained blue. The same pattern of labeling is observed in a subset of patients with cicatricial pemphigoid..")
26
Bullous Pemfigoid Treatment: Topical corticosteroid +/- prednisolone Prednisolone + azathioprine Prednisolone + plasma exchange Tetracycline + niacinamide Dapsone Mycophenolate mofetil Methotrexate Cyclophosphamide Chlorambucil IVIG Cyclosporin

27
Bullous Pemfigoid Course and Prognosis: Usually self-limitted over a 5- to 6- year period This period is generally a year or less in children Relapse occur in 10 % to 15% of patients once therapy is discontinued. Risk factors for death during the first year after diagnosis: The presence of circulating anti-BP180 antibodies Greater age Higher daily steroid dosage at discharge Low serum albumin ESR >30 mm/h

28
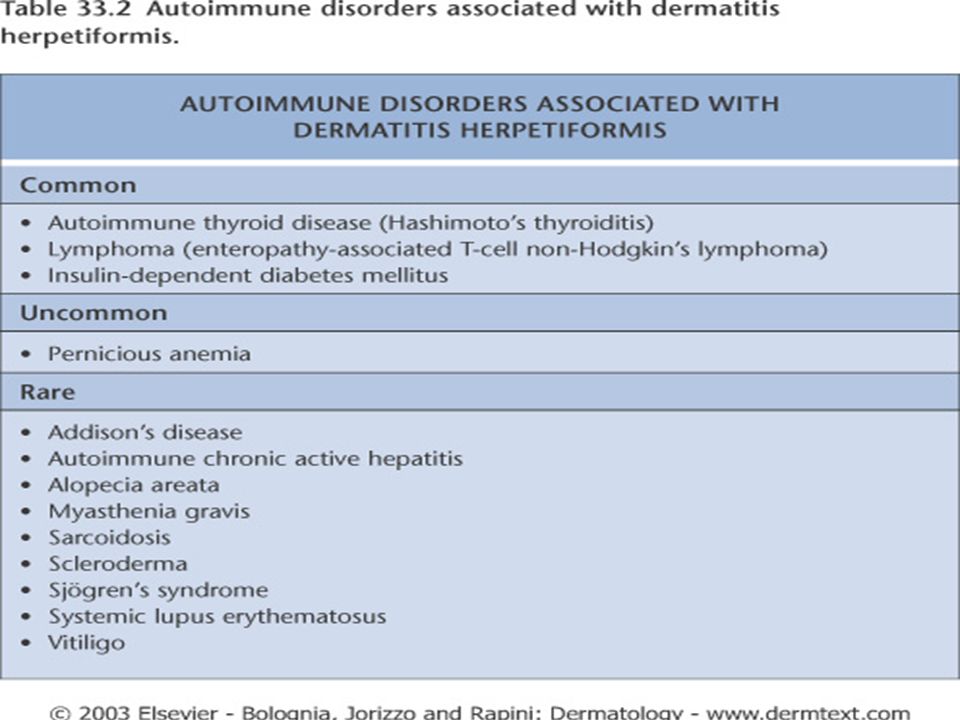
Dermatitis Herpetiformis Chronic, relapsing, severely pruritic disease characterized by grouped, symmetrical lesions on extensor surfaces, the scalp, nuchal area, and buttocks. Generally present as excoriations Eruption usually occurs on an erythematous base and may be papular, papulovesicular, vesiculobullous, bullous or urticarial Linear petechial lesions may be noted in the palmar area Mucous membranes are involved in rare cases

29
Dermatitis Herpetiformis 77% to 90% of patients with Dh are HLA-B8 positive, a similar frequency to that observed in gluten sensitive enteropathy (GSE) Gluten, a protein found in cereals except for rice and corn, provokes flares of the disease Villous atrophy of the jejunum and inflammation of the small bowel occurs IgA is bound to the skin, and this apparently activates complement, primarily via the alternate pathway Circulating IgA antibodies against the smooth muscle cell endomysium (anti-endomysial antibodies) are present in 70% of DH patients, in nearly all active celiac disease patients, and almost never in other conditions.
 Gluten, a protein found in cereals except for rice and corn, provokes flares of the disease Villous atrophy of the jejunum and inflammation of the small bowel occurs IgA is bound to the skin, and this apparently activates complement, primarily via the alternate pathway Circulating IgA antibodies against the smooth muscle cell endomysium (anti-endomysial antibodies) are present in 70% of DH patients, in nearly all active celiac disease patients, and almost never in other conditions.")
33
Dermatitis Herpetiformis Entheropathy: 70% to 100% of patients with dh have abnormalities in the jejunal mucosa, but most are asymptomatic If given a high-gluten diet, virtually all patients with DH develop findings indistinguishable from celiac disease DH affects 25% of celiac patients Dapson requirement in DH is usually decreased after 3-6 months of a gluten-free diet

34
Dermatitis Herpetiformis Differential Diagnosis: Linear IgA bullous dermatosis (clinically impossible) BP Bullous erythema multiforme Scabies Contact dermatitis Atopic dermatitis Nummular eczema Neurotic excoriations Insect bites Chronic bullous disease of childhood
 BP Bullous erythema multiforme Scabies Contact dermatitis Atopic dermatitis Nummular eczema Neurotic excoriations Insect bites Chronic bullous disease of childhood")
35
Dermatitis Herpetiformis M=F Average age of onset is between 20 and 40 years Occur in some frequency in children Black and Asian persons are rarely affected

36
Dermatitis Herpetiformis Histopathology: At the tips of the dermal papillae edema, focal fibrin, and neutrophilic microabcesses Subepidermal seperation Nearly 40% of patients have nonspecific findings on H&E: DIF studies are essential Histologic differentiation of linear IgA bullous dermatosis from DH is extremely difficult unless DIF is performed DIF from perilesional skin: granular pattern deposits of IgA +/- C3 at the dermoepidermal junction IgM and IgG deposits are occasionally observed in association with IgA

37
Neutrophilic microabscess

38
DIF showing granular IgA deposition along the dermal–epidermal junction

39
Dermatitis Herpetiformis Treatment: Dapsone Gluten-free diet

Similar presentations







>")














