Download presentation
Presentation is loading. Please wait.

1
Alessandro Settimi Ciro Esposito “Federico II” University, Naples Italy Division of Pediatric Surgery Chief: Prof Alessandro Settimi Minimally Invasive Surgery In Pediatric Urology

2
MIS is an alternative approach to OPEN SURGERY

3
Instruments

4
Laparoscopic Primary Pullthrough for Hirschsprung’s disease Aspetto Estetico LAPAROTOMIA LAPAROSCOPIA

5
Urinary tract pathologies - VUR - UPJO - MKDK - Non functioning Kidney - Duplex Kidney - Stones - Urachal cysts - Ureter pathology

6
Duplex Kidney

7
Partial - Nephrectomy Non-functioning upper or lower pole secondary to complicated duplex anomalies of the kidney The usual pathology of the upper pole is obstruction associated with a ureterocele or incontinence secondary to an ectopic ureter The usual pathology in the lower pole is reflux Indication

8
Partial nephrectomy is technically more demanding than total nephrectomy Currently, this procedure is performed using a retroperitoneal or transperitoneal approach. Partial Nephrectomy Lee RS et al: Pediatric retroperitoneal lap… J Urol 174: 702, 2005

9
LAPAROSCOPIC PARTIAL NEPHRECTOMY (LPN)
")
10
Patient’s Position Position for a right Nephrectomy LATERAL POSITION A ballast is placed under the patient

11
Patient’s Position #2

12
Team

13
Trocars 1: 10mm 2: 5mm 3: 5mm 4: 5mm 4 5mm 4

14
Step # 1 Stent positioning Incision of the lateral peritoneal fold

15
STEP # 2 Colon

16
STEP # 3 Ureteral section

17
STEP # 4 Kidney

18
STEP # 5 vessels u.p.

19
STEP # 6 Hemi-nephrect u.p.

20
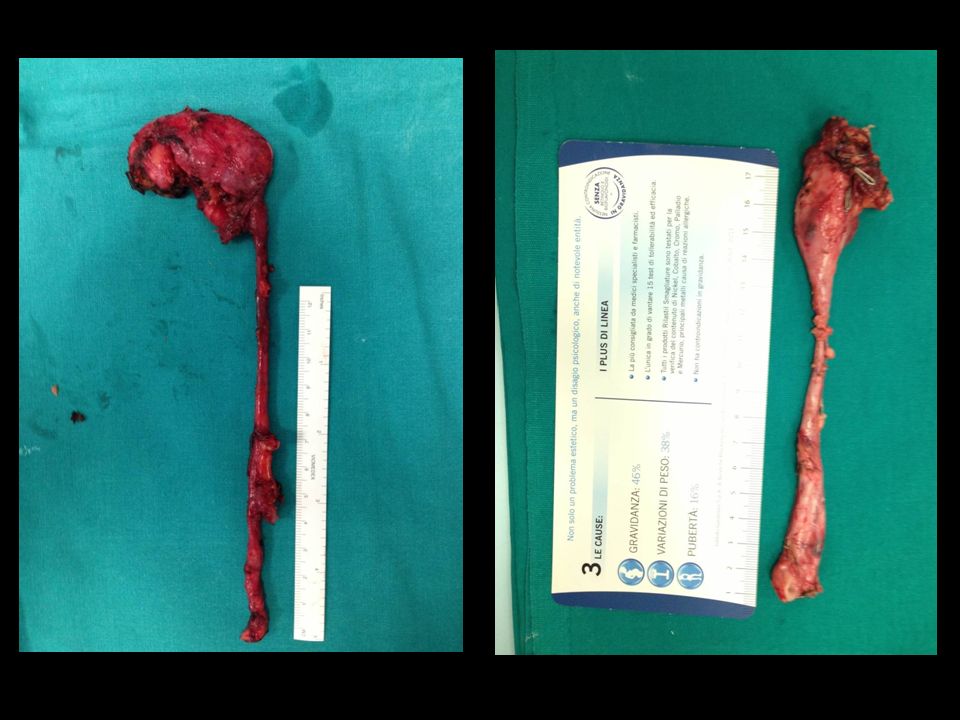
STEP # 7 Specimen removal

21
LPN personal Results Operative time: 90 min (70 to 120) Lenght of stay: 3-4 days Conversions: 0
 Lenght of stay: 3-4 days Conversions: 0")
22
Laparoscopic transposition of lower pole crossing vessels in extrinsic uretero-pelvic junction (UPJO) obstruction in children
 obstruction in children")
23
Background # 2 A recent study demonstrated that 58% of older children with symptomatic PUJO had lower pole crossing vessels [ The traditional management for lower pole vessels causing PUJO has been dismembered pyeloplasty The Hellstrom procedure, in which crossing polar vessels are relocated, has been an option in adult urological practice

24
Clinical findings Indication: abdominal pain presenting as Dietl’s crisis, UTI and rarely haematuria Median age of presentation > 6 years Absence of pre-natally detected hydronephrosis

25
Pre-operative work-up Renal ultrasonography Doppler ultrasound Scintigraphy MRI

26
Technique # 1 At laparoscopy the presence of a lower pole vessel is confirmed in the absence of a narrow PUJ The PUJ and the pelvis are adequately mobilised achieving easy displacement of vessels

27
Technique # 2 The ‘ shoe-shine ’ manoeuvre of the mobilised anterior pelvis behind the lower pole vessels confirms adequate availability of the pelvis to perform a loose wrap around the vessels

28
Technique # 3 Two or three interrupted sutures may be necessary to achieve an adequate tunnel within the anterior pelvic wall

29
Trocars 1: 10mm 2: 5mm 3: 5mm 4 4

30
STEP # 1 Dissection

31
STEP # 2 pelvis

32
STEP # 3 wrap

33
Classic UPJO

34
Patient’s Position #2

35
Trocars 1: 10mm 2: 5mm 3: 5mm 4 4

36
Lap Pyeloplasty

37
Urachal Anomalies In Pediatric Patients

38
Background Urachus is a 3-layered canal that connects the allantois to the fetal bladder. Descent of the bladder in month 5 of development stretches the urachus, causing its lumen to obliterate and become the median umbilical ligament. Occasionally this process may be incomplete and an epithelialized urachal canal may persist into adulthood.

39
Background # 2 This leaves the potential for various urachal anomalies, including cysts, sinus tracts, diverticula and malignancies 1) vesicourachal diverticulum 2) urachal cyst 3) Umbilical-urachus sinus
 vesicourachal diverticulum 2) urachal cyst 3) Umbilical-urachus sinus")
40
Indication Children with urachal anomalies, in about 60-70 % of patients have symptoms (umbilical drainage, hematuria, UTI, abdominal pain), In the other 30-40 % of patients the urachal anomalies are diagnosed incidentally during abdominal surgery performed for another indication
, In the other % of patients the urachal anomalies are diagnosed incidentally during abdominal surgery performed for another indication")
41
Technique # 1

42
Technique # 2

43
Technique # 3

44
Technique # 4

45
Technique # 5

46
LEVUR Laparoscopic Lich-Gregoir procedure In patients with VUR

47
VUR Techniques STING COHEN 70-85 % Success Rate 95 -98 % Day Surgery Hospitalisation 6-10 days No Pain +++++ Yes Ureteral Cath after No

48
LEVUR Laparoscopic Lich-Gregoir procedure

49
Trocars Position Optic 5mm 30° 3-mm trocars

50
LEVUR # 1 Ureter Isolation

51
LEVUR # 2 Ureteral Dissection

52
LEVUR # 3 Fix and prepare the bladder

53
LEVUR # 4 Ureter reimplantation

54
LEVUR # 5 Final Check

55
No ScarsPfanenstiell Incision3 small scars Day SurgeryHospitalisation 5-10 dHospitalisation 24-36h No Pain post-op discompfort 8-15 Days No pain 1st Inj : 75-85% 2nd inj : 90-95% 96- 98% Cistoscopy ?? 95-96% Ureters in the same axis RESULTS # 2

56
Difficult procedure to perform Delicate and fine dissection It’s fundamental to know the details of the technique Day surgery, excellent post-operative period No pain, no drugs, no catheters Comparable results with open Cohen Conclusions SURGEON ++ PATIENT ++++++

57
OPEN COHEN 5 Post Op day LEVUR 1 Post Op day

58
LAPAROSCOPIC Nephrectomy in Pediatric Patients

59
Nephrectomy Indication Non-functioning kidney secondary to VUR Non-functioning kidney secondary to UPJO with an ureterostomy Pelvic Kidney Previous renal surgery Infections

60
Trocars 1: 10mm 2: 5mm 3: 5mm

61
Step # 2 Isolate Kidney and ureter Vessels clipped and sectioned Ureter clipped and sectioned Remove the Kidney

62
Step # 1 ureter

63
Step # 2 vessels

67
Advanatages of MIS in Pediatric Urology Improve precision thanks to magnified view Less Pain Less Drugs Shorter Hospital Stay Better Cosmesis Same good long term Results

68
CONCLUSIONS In the 21° century it is unacceptable to perform any surgical procedure on a child by the open route if it can be safely and easily be carried out through minimally invasive surgery Gordon Mc Kinlay

Similar presentations









 Fellowship in Andrology (U of Ottawa) Fellowship in EndoUrology and Laparoscopy.>")

 Incidence: 1:188 Approximately 50% of antenatal scans are normal postnatally Posterior urethral.>")





 are variable, occur in 1 of 500 newborns; predisposing to development of hypertension,>")



