Download presentation
Presentation is loading. Please wait.

1
بنام خداوند جان وخرد

2
Anaerobic Bacteria Clostridia cont… C. perfringens, C
Anaerobic Bacteria Clostridia cont… C. perfringens, C. difficile Bacteroides, Porphyromonas Dr Alvandi 94-95

3
نمونه سوالات علوم پايه

4
کداميک از کلستريديوم هاي زير مي تواند عامل اسهال ناشي از مصرف طولاني مدت آمپي سيلين باشد؟
الف- كلستريديوم ديفيسيل ب- كلستريديوم پرفرينجنس ج- كلستريديوم بوتولينوم د- كلستريديوم تتاني شهريور 88

5
در اسهال هاي مرتبط با مصرف آنتي بيوتيک، شايعترين باکتري کدام است؟
الف- كلستريديوم ديفيسيل ب- سودوموناس ايروژينوزا ج- يرسينيا انتروکوليتيکا د- كلستريديوم پرفرينجنس شهريور86

6
كداميك از باكتري هاي زير عامل سببي گانگرن گازي (ميونكروز) مي باشد؟
الف- كلستريديوم پرفرينژنز ب- سودوموناس ايروژينوزا ج- استافيلوكوكوس اورئوس د- كورينه باكتريوم ديفتريه اسفند 84

7
كداميك از باكتري هاي زير عامل سببي کولیت با غشای کاذب می گردد؟
الف- شیگلا دیسانتری ب- سالمونلا تیفی ج- کمپیلوباکتر فتوس د- کلستریدیوم دیفیسیل شهریور 81

8
Pathogenic Clostridia
Species Human Disease Frequency C. difficile Antibiotic-associated diarrhea, pseudomembranous colitis Common C. perfringens Soft tissue infections (i.e.,Cellulitis, suppurative myositis, myonecrosis or gas gangrene), food poisoning, enteritis necroticans, septicemia C. botulinum Botulism Uncommon C. tetani Tetanus C. butyricum Rare C. novyi Gas gangrene
, food. poisoning, enteritis necroticans, septicemia. C. botulinum. Botulism. Uncommon. C. tetani. Tetanus. C. butyricum. Rare. C. novyi. Gas gangrene.")
9
Clostridium perfringens
Is one of few nonmotile clostridia Rapidly spreading growth on laboratory media (resembling motile organisms) hemolytic Lethal toxins subdivide isolates into five types (A-E)
 hemolytic. Lethal toxins subdivide isolates into five types (A-E)")
11
Clostridium perfringens
Type Alpha(α) Beta (β) Epsilon (ε) Iota (ι) A x B C D E
 Beta (β) Epsilon (ε) Iota (ι) A. x. B. C. D. E.")
12
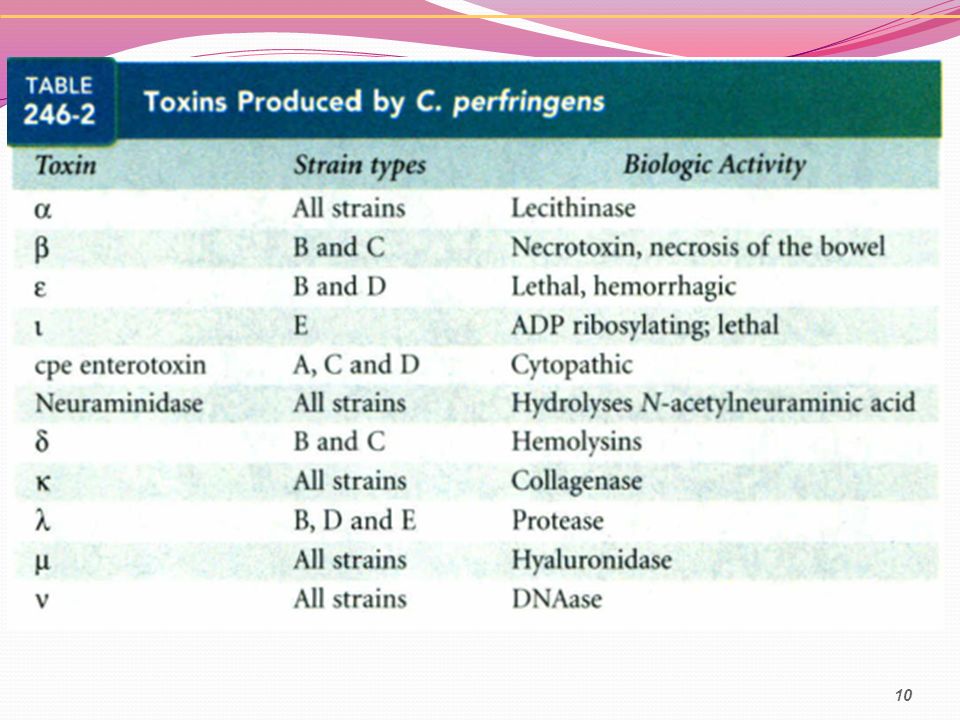
Lethal toxin; phospholipase C (lecithinase); hemolysin
Virulence Factors Biologic Activity α toxin Lethal toxin; phospholipase C (lecithinase); hemolysin β toxin Lethal toxin; necrotizing activity (Enteritis necroticans, pig-bel) ε toxin Lethal toxin; permease ζ toxin Lethal binary toxin; ADP ribosylating δ toxin Hemolysin Θ toxin Heat- and oxygen-labile hemolysin; cytolytic κ toxin Collagenase; gelatinase; necrotizing activity λ toxin Protease μ toxin Hyaluronidase ν toxin Deoxyribonuclease; hemolysin; necrotizing activity Enterotoxin Alters membrane permeability; by type A strains Neuraminidase Alters cell surface ganglioside receptors;
; hemolysin. β toxin. Lethal toxin; necrotizing activity. (Enteritis necroticans, pig-bel) ε toxin. Lethal toxin; permease. ζ toxin. Lethal binary toxin; ADP ribosylating. δ toxin. Hemolysin. Θ toxin. Heat- and oxygen-labile hemolysin; cytolytic. κ toxin. Collagenase; gelatinase; necrotizing activity. λ toxin. Protease. μ toxin. Hyaluronidase. ν toxin. Deoxyribonuclease; hemolysin; necrotizing activity. Enterotoxin. Alters membrane permeability; by type A strains. Neuraminidase. Alters cell surface ganglioside receptors;")
13
Epidemiology Type A commonly inhabits intestinal tract of humans and animals in soil and water contaminated with feces Types B-E do not survive in soil colonize intestinal tracts of animals and occasionally humans Type A is responsible for most human infections soft tissue infections, food poisoning, and primary septicemia Type C is responsible for enteritis necroticans (Pigbel)
")
14
Clinical Diseases 1- Soft Tissue Infections 2- Food Poisoning
Cellulitis Fasciitis or suppurative myositis Myonecrosis or gas gangrene 2- Food Poisoning 3- Necrotizing Enteritis 4- Septicemia

15
Clinical Diseases 1- Soft Tissue Infections
Most isolates of C. perfringens species from wound cultures are insignificant Organisms can also initiate cellulitis with gas formation in soft tissue Can progress to suppurative myositis Characterized by An accumulation of pus in muscle planes Absent of muscle necrosis and systemic symptoms

16
Clinical Diseases Myonecrosis or gas gangrene
Generally develops within a week after clostridia are introduced Intense pain, Shock Extensive muscle necrosis Renal failure, Death Cellular lysis by clostridial toxins Abundant rectangular, gram-positive rods Absence of inflammatory cells C. perfringens, and other species (C. septicum, C. histalyticum, and C. novyi)
")
17
Clinical Diseases Clostridial food poisoning
A short incubation period (8 to 24 hours) Abdominal cramps, watery diarrhea (no fever, nausea, or vomiting) A clinical course lasting less than 24 hours Ingestion of meat product 108 to 109 organisms of type A C. perfringens Reheating of food to 74° C can destroy heat-labile enterotoxin
 Abdominal cramps, watery diarrhea (no fever, nausea, or vomiting) A clinical course lasting less than 24 hours. Ingestion of meat product. 108 to 109 organisms of type A C. perfringens. Reheating of food to 74° C can destroy heat-labile enterotoxin.")
18
Clinical Diseases Necrotizing Enteritis
Rare, acute necrotizing process in jejunum Abdominal pain, bloody diarrhea, shock, and peritonitis Mortality is 50% β-Toxin-producing C. perfringens type C Septicemia Isolation from bloods patients with significant infections (myonecrosis, necrotizing enteritis)
")
19
Diagnostic Laboratory Tests
Clinical presentation Large gram-positive rods in specimen (wounds, pus, and tissue) spores are not regularly present. chopped meat-glucose medium and thioglycolate medium A clot torn by gas in 24 hours is suggestive of C perfringens. Lecithinase activity is evaluated by precipitate formed around colonies on egg yolk media Toxin production and neutralization by specific antitoxin. C perfringens
 spores are not regularly present. chopped meat-glucose medium and thioglycolate medium. A clot torn by gas in 24 hours is suggestive of C perfringens. Lecithinase activity is evaluated by precipitate formed around colonies on egg yolk media. Toxin production and neutralization by specific antitoxin. C perfringens.")
20
Blood agar plate with C. perfringens:
characteristic double zone of hemolysis alpha-toxin incomplete outer zone theta-toxin clear inner

21
Laboratory Diagnosis Food poisoning
recovery of more than 105 organisms per gram of food or more than 106 bacteria per gram of feces collected within 1 day of onset of disease

22
Treatment, Prevention, and Control
Surgical debridement and high-dose penicillin therapy Mortality ranging from 40% to almost 100% Antibiotic therapy for clostridial food poisoning is unnecessary, because this is a self-limiting disease Symptomatic treatment for food poisoning

23
Clostridium difficile

24
Physiology and Structure
Anaerobic, gram positive rod Produces toxins Pseudomembranous colitis High prevalence among hospital patients Antibiotic associated

25
Pathogenesis and Immunity
Virulence Factor Biologic Activity Enterotoxin (toxin A) Produces chemotaxis; induces cytokine production with hypersecretion of fluid; produces hemorrhagic necrosis Cytotoxin (toxin B) Induces depolymerization of actin with loss of cellular cytoskeleton Adhesin factor Mediates binding to human colonic cells Hyaluronidase Produces hydrolytic activity
 Produces chemotaxis; induces cytokine production with. hypersecretion of fluid; produces hemorrhagic necrosis. Cytotoxin. (toxin B) Induces depolymerization of actin with loss of. cellular cytoskeleton. Adhesin factor. Mediates binding to human colonic cells. Hyaluronidase. Produces hydrolytic activity.")
26
Clinical Disease Antibiotics disrupt normal flora
Ampicillin, cephalosporins, fluoroquinolones and Clindamycine Uncontrolled proliferation of C. difficile Onset days after start of antibiotic Asymptomatic Carriage Antibiotic-associated diarrhea without colitis Antibiotic-associated colitis without pseudomembrane Formation Pseudomembranous colitis Fulminant disease (toxic megacolon, ileus, perforation, sepsis)
")
27
Epidemiology Colonizes 5% of healthy individuals endogenous infection
exogenous source of infection: Fecal-oral

28
Clinical Disease

29
C. difficile Associated Disease (CDAD)
")
30
Laboratory Diagnosis Symptoms Diagnostic tests
Loose, watery stools, Fever Crampy lower abdominal pain, anorexia Diagnostic tests Stool studies: Toxin, fecal leukocytes Labs: leukocytosis with left shift, dehydration, acidosis Endoscopy: pseudomembranes Radiology: thickened colonic wall, megacolon

31
Laboratory Diagnosis Isolation of organism in stool culture documents colonization but not disease. Demonstration of enterotoxin or cytotoxin in a stool specimen Immunoassays. In vivo cytotoxicity assay using tissue culture cells and specific neutralizing antibodies for cytotoxin

32
Laboratory Diagnosis Diagnosis: Detection of toxins
Detection of organism culture of feces for C. difficile (48-72 h) immunoassay Detection of toxins tissue culture
 immunoassay. Detection of toxins. tissue culture.")
33
The appearance of Clostridium difficile on
cycloserine-cefoxitin-fructos agar (CCFA): yellow, "ground-glass“ colonies and a yellowing of the medium around the colonies
: yellow, ground-glass colonies and a yellowing of the medium around the colonies.")
34
Treatment, Prevention, and Control
Discontinuation of implicated antibiotic (e.g., ampicillin, clindamycin, fluoroquinolones) Specific therapy with metronidazole or vancomycin is necessary for the management of severe diarrhea or colitis. Relapses may occur in as many as 20% to 30% of patients after completion of therapy. It is difficult to prevent disease, because organism commonly exists in hospitals, particularly in areas adjacent to infected patients (e.g., beds, bathrooms). Spores of C. difficile are difficult to eliminate unless thorough housekeeping measures are used. Thus organism can contaminate an environment for many months and can be a major source of nosocomial outbreaks of C. difficile disease.
 Specific therapy with metronidazole or vancomycin is necessary for the management of severe diarrhea or colitis. Relapses may occur in as many as 20% to 30% of patients after completion of therapy. It is difficult to prevent disease, because organism commonly exists in hospitals, particularly in areas adjacent to infected patients (e.g., beds, bathrooms). Spores of C. difficile are difficult to eliminate unless thorough housekeeping measures are used. Thus organism can contaminate an environment for many months and can be a major source of nosocomial outbreaks of C. difficile disease.")
35
Treatment, Prevention, and Control
Most important: Cessation of inciting antibiotic Non-antibiotic management: Correction of fluid and electrolyte losses Avoid anti-peristaltic agents Indications for antibiotic treatment: 1) Evidence of colitis 2) Persistent diarrhea despite cessation of abx 3) Need to continue abx to treat underlying infection Metronidazole; Vancomycin
 Evidence of colitis. 2) Persistent diarrhea despite cessation of abx. 3) Need to continue abx to treat underlying infection. Metronidazole; Vancomycin.")
36
Other Clostridial Species
C. septicum is a particularly important pathogen because it is a cause of non-traumatic myonecrosis and often exists in patients with occult colon cancer, acute leukemia, or diabetes. after initial presentation. C. sordellii is implicated in fatal toxic shock syndrome associated with natural childbirth or medically induced abortions. C. tertium s commonly isolated in soil samples. It has primarily been associated with traumatic wound infections (e.g., war wounds, a fall producing a soil-contaminated wound)
")
37
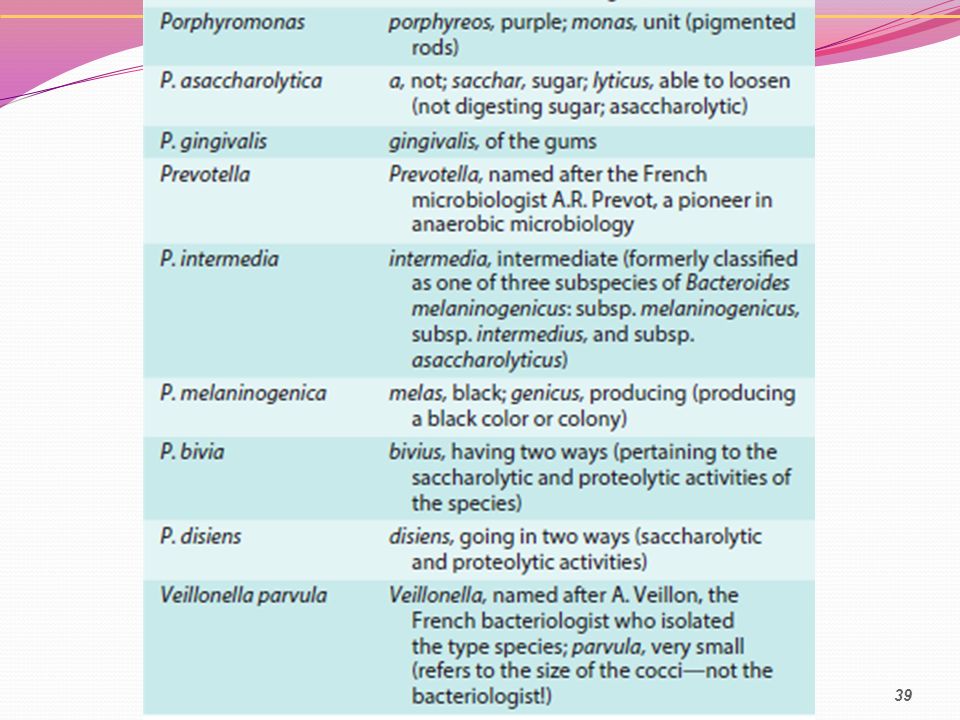
Anaerobic Gram-Negative Bacteria
colonize the human upper respiratory, gastrointestinal and genitourinary tracts Anaerobes are the predominant bacteria at each of these sites, outnumbering aerobic bacteria 10- to 1000-fold. Bacteroides, Fusobacterium, Parabacteroides, Porphyromonas, Prevotella Veillonella

41
Treatment all members of the B. fragilis group, many Prevotella and Porphyromonas species, and some Fusobacterium isolates produce β-lactamases. metronidazole carbapenems (e.g., imipenem, meropenem), β-lactam–β-lactamase inhibitors (e.g., piperacillin-tazobactam).
, β-lactam–β-lactamase inhibitors (e.g., piperacillin-tazobactam).")
42
Questions???

43
Thanks for your attention

Similar presentations





: Fast Facts. What is Clostridium difficile (C. diff)? C. diff is a bacteria that lives in the intestinal tract of about.>")









 –Bacteria or their products may migrate to adjacent tissues or bloodstream.>")



, Ph.D. Departg ment of Microbiology & Immunology, NCKU ext 5632 References: 1. Chapter.>")

