Download presentation
Presentation is loading. Please wait.

1
Statins in risk reduction Vasil Velchev MD, PhD St.Anna University Hospital, Sofia

2
Number of deaths (000s) Leading causes of death in the world World Health Report 2002 http://www.who.int/whr/2002/annex/en/index.html 02000400060008000 Occupational risk factors for injury Unsafe health care injections Vitamin A deficiency Zinc deficiency Urban air pollution Iron deficiency Indoor smoke from solid fuels Unsafe water, sanitation, and hygiene Alcohol Physical inactivity High BMI Fruit and vegetable intake Unsafe sex Malnutrition Cholesterol Smoking High blood pressure
 Leading causes of death in the world World Health Report Occupational risk factors for injury Unsafe health care injections Vitamin A deficiency Zinc deficiency Urban air pollution Iron deficiency Indoor smoke from solid fuels Unsafe water, sanitation, and hygiene Alcohol Physical inactivity High BMI Fruit and vegetable intake Unsafe sex Malnutrition Cholesterol Smoking High blood pressure")
3
Clinical manifestation of atherosclerosis Cardiovascular diseases CHD, MI, SCD, CHF & arrhythmias Cerebrovascular diseases Transient ischemic attack, stroke Peripheral vascular disease Claudication intermittent, gangrene, cold feet, болки в краката, erectile dysfunction

4
Cardiovascular disease continuum Endothelial dysfunction Remodeling Target organs damage Tissue damage MI, stroke Pathological remodeling Ventricular Dilatation, Glomerulo- sclerosis Congestive heart failure, nephropathy End stage organ failure Death Dyslipidemia Hypertension Diabetes Endothelial dysfunction Vascular diseases Dzau VJ, 2001; Dzau V, et al. 1991; Anderson S, 2003

5
What are target levels for treatment and prevention? Total cholesterol target levels is the part of patient common absolutely risk appraisal. The real objective is a LDL-C target levels. Both European and American guidelines define low levels of LDL-C (<1,8 mmol / l) as the primary goal of therapy in patients with established coronary artery disease or equivalent risk
 as the primary goal of therapy in patients with established coronary artery disease or equivalent risk.")
6
Decrease of LDL-C with1 mmol/L (39 mg/dL) is related with… Baigent C, et al, Cholesterol Treatment Trialists’ (CTT) Collaborators. Lancet 2005;366:1267–1278. A prospective meta-analysis of data from 90,056 individuals in 14 randomised trials of statins 1 Correlation between decreasing of events and optimal LDL-C reduction for 1 year Decreasing of frequency events (% SE)
.")
7
Relation between LDL-C, HDL-C & risk of Cardiovascular diseases 1 mmol/l 1 mmol/l decrease of LDL-C 20% reduced risk with 20% 0,1 mmol/l 0,1 mmol/l increase of 10% HDL-C reduced risk with 10% (CARE) Graham 1, et al. European guidelines on cardiovascular disease prevention in clinical practice: executive summary. Fourth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice. Eur Heart J 2007

8
HDLs (High-density lipoproteins) is a new object of interest. In vitro conditions, HDL-C helps purification of foamy cells developing in injured arteries. The low level of HDL-C is an independent risk factor strongly and inversely associated with risk of CHD. National Cholesterol Education Program Expert Panel. Detection, evaluation and treatment of high blood cholesterol in adults. (Adult Treatment Panel III). Circulation 2002 Relation between LDL-C, HDL-C & risk of Cardiovascular diseases
. Circulation 2002 Relation between LDL-C, HDL-C & risk of Cardiovascular diseases.")
9
The main risk factors (with the exception of LDL- C), which alter the goals of LDL-C Hypertension (RR ≥ 140/≥ 90 mm Hg or use of antihypertensive drugs) Low HDL-C (<1 mmol/l) Family history of premature CVD - first in men in '55 or '65 women under Age (man≥ 45 years old, women ≥ 55 years old)
, which alter the goals of LDL-C Hypertension (RR ≥ 140/≥ 90 mm Hg or use of antihypertensive drugs) Low HDL-C (<1 mmol/l) Family history of premature CVD - first in men in 55 or 65 women under Age (man≥ 45 years old, women ≥ 55 years old)")
10
Risk categories (from highest to lowest) Target of LDL-C Target of TC** Target of HDL-С** Target of TG (on an empty stomach) 1. Very high risk Documented CVD by invasive or non-invasive testing (such as coronary angiography, stress echocardiography, carotid plaque on ultrasound), previous myocardial infarction(MI), ACS, coronary revascularization and other arterial revascularization procedures, ischemic stroke, PAD. Patients with type 2 diabetes, patients with type 1 diabetes with target organ damage (such as microalbuminuria). Patients with moderate to severe CKD (GFR-6mL/min/1.73m2). A calculated 10 year risk SCORE ≥10%. < 1,8 mmol/L < 4,0 mmol/L >1.0 mmol/L за жени >1,2 mmol/L за мъже < 1.7 mmol/L 2. High risk Markedly elevated single risk factors such as familial dyslipidemias and severe hypertension. A calculated SCORE ≥5% and,10% for 10 year risk of fatal CVD. < 2,5 mmol/L < 4,5 mmol/L>1.0 mmol/L за жени >1,2 mmol/L за мъже < 1.7 mmol/L 3. Moderate risk Subjects are considered to be at moderate risk when their SCORE is ≥1% and,5% at 10 years. Many middle-aged subjects belong to this risk category. This risk is further modulated by a family history of premature CAD, abdominal obesity, physical activity pattern and social class. < 3.0 mmol/L < 4,5 mmol/L>1.0 mmol/L за жени >1,2 mmol/L за мъже < 1.7 mmol/L 4. Low risk The low risk category applies to individuals with SCORE,1%. < 3.0 mmol/L < 5.0 mmol/L>1.0 mmol/L за жени >1,2 mmol/L за мъже < 1.7 mmol/L Target of lipoprotein levels, based on the global risk of changes in recent European guidelines of 2011* *ESC/EAS Guidelines for the management of dyslipidemias, 2011 ** European guidelines on cardiovascular disease prevention in clinical practice, 2007
, previous myocardial infarction(MI), ACS, coronary revascularization and other arterial revascularization procedures, ischemic stroke, PAD. Patients with type 2 diabetes, patients with type 1 diabetes with target organ damage (such as microalbuminuria). Patients with moderate to severe CKD (GFR-6mL/min/1.73m2). A calculated 10 year risk SCORE ≥10%. < 1,8 mmol/L < 4,0 mmol/L >1.0 mmol/L за жени >1,2 mmol/L за мъже < 1.7 mmol/L 2. High risk Markedly elevated single risk factors such as familial dyslipidemias and severe hypertension. A calculated SCORE ≥5% and,10% for 10 year risk of fatal CVD. < 2,5 mmol/L < 4,5 mmol/L>1.0 mmol/L за жени >1,2 mmol/L за мъже < 1.7 mmol/L 3. Moderate risk Subjects are considered to be at moderate risk when their SCORE is ≥1% and,5% at 10 years. Many middle-aged subjects belong to this risk category. This risk is further modulated by a family history of premature CAD, abdominal obesity, physical activity pattern and social class. < 3.0 mmol/L < 4,5 mmol/L>1.0 mmol/L за жени >1,2 mmol/L за мъже < 1.7 mmol/L 4. Low risk The low risk category applies to individuals with SCORE,1%. < 3.0 mmol/L < 5.0 mmol/L>1.0 mmol/L за жени >1,2 mmol/L за мъже < 1.7 mmol/L Target of lipoprotein levels, based on the global risk of changes in recent European guidelines of 2011* *ESC/EAS Guidelines for the management of dyslipidemias, 2011 ** European guidelines on cardiovascular disease prevention in clinical practice,")
11
Pleiotropic effects : Improving or restoring endothelial function Strengthen the stability of atherosclerotic plaques Reduction of oxidative stress Reducing vascular inflammation Anti-thrombotic effects In 61 trials with a total of 55.000 cases of cardiovascular death, treatment with statins has led to strikingly reduced incidence of stroke, despite the lack of connection with plasma cholesterol levels. Pleiotropic effects of statins Takemoto M, Liao JK. Arterioscler Thromb Vasc Biol2001;21:1712-1719.

12
How statins “work” in time? DaysYears LDL-C lowering Inflammation reduction Plaque stabilization Restoration of endothelial function Reduction of ischemic episodes CV events reduction*

13
Additional benefits of statins Prevention of stroke Reduce inflammation in the coronary arteries Affect vascular proliferation Known immunomodulation Reduce the risk of osteoporosis Reduced risk of colon cancer (in combination with NSAIDs) Reduced risk of Alzheimer's disease Reduce the symptoms of MS
 Reduced risk of Alzheimer s disease Reduce the symptoms of MS")
14
Why Statins for the prevention of stroke? Patients after stroke are high risk for coronary artery disease Treatment with statins can reduce: Risk of stroke after MI 1-3 Risk of stroke or death after endarterectomy 4 FDA has approved some statins in patients after a stroke or "evidence of cerebrovascular disease” 1. Sacks FM, et al. N Engl J Med. 1996;335:1001-1009. 2. The LIPID Study Group. N Engl J Med. 1998;339:1349-1357. 3. Heart Protection Study Collaborative Group. Lancet. 2002;360:7-22. 4. Kennedy J, et al. Stroke. 2005;36:2072-2076.

15
Evaluation of the outcome of the survey data for primary prevention with statins Meta-analysis of studies on primary prevention, n=65 000 Mills EJ, Rachlis B, Wu P, Devereaux PJ, Arora P, Perri D. Primary prevention of cardiovascular mortality and events with statin treatments: a network meta-analysis involving more than 65,000 patients. J Am Coll Cardiol. 2008;52(22):1769–1781.
:1769–")
16
Recommendation NCEP ATP III Goldstein et al. Published online in Stroke Dec. 2, 2010 Treatment with statins in addition to changes in lifestyle to change LDL-C is as recommended in the NCEP primary prevention of ischemic stroke in patients with coronary artery disease or some high- risk, such as diabetes. Class I; Level of evidence A

17
Statins & prevention of stroke : A meta-analysis Prevention of stroke in patients at risk for stroke 4 studies, 6808 patients Frequency of stroke Placebo 3.1% Statin2.7%RR 15% Prevention of stroke in patients who have experience of stroke 8 studies, 11 710 patients Frequency of stroke Placebo 5.6% Statin4.1%RR 27% This meta-analysis covering more than 120,000 people demonstrated powerful statin-dependent decrease in the incidence of ischemic stroke and related mortality, which can not be related only to the extent of the decrease in LDL-C Crouse et al, Arch Int Med 1997

18
Heart Protection Study - results

19
Secondary prevention The latest recommendations of the AHA (American Heart Association) and ACC (American College of Cardiology) for secondary prevention support aggressive treatment that reduces the risk in patients with established coronary or other atherosclerotic vascular disease
 and ACC (American College of Cardiology) for secondary prevention support aggressive treatment that reduces the risk in patients with established coronary or other atherosclerotic vascular disease")
20
Aggressive statins therapy: A meta analysis Meta-analysis of 26 randomized trials (21 statin trials versus placebo and 5 trials of intensive statin against the standard dose), 170 000 patients which is published 2010. In summary: 1 mmol/l reduction in LDL-C with statin drug therapy lead to 20% reduction of vascular events (coronary death, nonfatal MI, coronary revascularization, and death) High doses of statins lead to additional lowering of LDL-C by an average of 0,51 mmol/l = 15% additional reduction in major vascular events, 13% in coronary mortality and nonfatal MI, 19% of the needs of coronary revascularization and 16% of ischemic stroke Effect (intensive dose) on cardiovascular events is significant in the first year - 12% reduction and increases with increasing time of administration of statin therapy - ~ 28% reduction for subsequent years (5.1 years) *Treatment Trialists’ (CTT) Collaborators. Efficacy and safety of more intensive lowering of LDL-C: a meta-analysis of data from 170000 participants in 26 randomized trials of statins. Lancet 2010
 High doses of statins lead to additional lowering of LDL-C by an average of 0,51 mmol/l = 15% additional reduction in major vascular events, 13% in coronary mortality and nonfatal MI, 19% of the needs of coronary revascularization and 16% of ischemic stroke Effect (intensive dose) on cardiovascular events is significant in the first year - 12% reduction and increases with increasing time of administration of statin therapy - ~ 28% reduction for subsequent years (5.1 years) *Treatment Trialists’ (CTT) Collaborators. Efficacy and safety of more intensive lowering of LDL-C: a meta-analysis of data from participants in 26 randomized trials of statins. Lancet")
21
Meta-analysis of studies examining intensive compared with moderate statin therapy J Am Coll Cardiol 2006;48:438–45 Summary Intensive therapy with high dose statin provides significant benefits over standard dose for protection mostly nonfatal events.

22
STELLAR Dose dependent reduction of LDL-C *p<0.002 vs ATV 10 mg; SIM 10, 20, 40 mg; PRA 10, 20, 40 mg †p<0.002 vs ATV 20, 40 mg; SIM 20, 40, 80 mg; PRA 20, 40 mg ‡p<0.002 vs ATV 40 mg; SIM 40, 80 mg; PRA 40 mg Jones PH et al. Am J Cardiol 2003; 92: 152–160 Changes in LDL-C according to baseline (%) 0–10–20–30–40–50–60 10 mg * –5–15–25–35–45–55 20 mg † 40 mg ‡ 10 mg 20 mg 80 mg 10 mg 20 mg 40 mg 80 mg 10 mg 20 mg 40 mg Rosuvastatin 10 mg (–46%) Rosuvastatin Atorvastatin Simvastatin Pravastatin 40 mg after 6 weeks
 0–10–20–30–40–50–60 10 mg * –5–15–25–35–45–55 20 mg † 40 mg ‡ 10 mg 20 mg 80 mg 10 mg 20 mg 40 mg 80 mg 10 mg 20 mg 40 mg Rosuvastatin 10 mg (–46%) Rosuvastatin Atorvastatin Simvastatin Pravastatin 40 mg after 6 weeks.")
23
*p<0.002 Rosuvastatin 10 mg vs pravastatin 10, 20 mg; #p<0.002 Rosuvastatin 20 mg vs simvastatin 40 mg, pravastatin 20, 40 mg; †p<0.002 Rosuvastatin 40 mg vs simvastatin 40 mg, pravastatin 40 mg –12 –18 –15 –18 1020408010204010204080 –8 –13 102040 Dose (mg) rosuvastatin atorvastatin pravastatin simvastatin Change in TG from baseline (%) –30 –25 –20 –15 –10 0 –5 –20 –23 –27 –28 –24 # –26 † –20 * STELLAR Changes in Triglyceride levels Jones PH, et al. Am J Cardiol 2003;92:152–60.

24
Summary The increase in HDL levels with statins is associated with clinical benefit Part of the change in HDL-C with statins is associated with decreased levels of triglycerides STELLAR Dose dependent increase of HDL-C Changes in HDL-C according to baseline (%) Dose (mg)
 Dose (mg)")
25
1.Lancet. 1994;344:1383; 2. N Engl J Med. 1995;333:1301; 3. N Engl J Med. 1996;335:1001; 4. JAMA. 1998;279:1615; 5. N Engl J Med. 1998;339:1349 Results of fundamental studies with statins (1)
.")
26
1.Lancet 2002;360:7-22; 2. Lancet 2002;360:1623-30; 3. JAMA 2002;288:2998-3007; 4. Lancet 2003;361:1149-58. Results of fundamental studies with statins (2)
.")
27
4S (Scandinavian Simvastatin Survival Study) : Clinical results Adapted from Scandinavian Simvastatin Survival Study Group Lancet 1994;344:1383-1389; Kjekshus J et al Am J Cardiol 1995;76(9):64C-68C; 0 –10 –20 –30 –40 –50 Fundamental 4S study showed that the use of simvastatin for secondary prevention leads to a reduction in mortality and incidence of coronary events. % Risk reduction Overall mortality p=0.0003 Major coronary events Coronary mortality Cardiovascular mortality p<0.00001 p<0.0001 p<0.00001 – 35% – 42% – 34% – 30% – 37% Revascularizations

28
Simvastatin is the first with indication prevention of cardiovascular diseases. Simvastatin reduced the risk of total mortality by 30%, coronary events by 34% in patients with coronary artery disease. After the end of the study (5.4 years) patients were followed for another 5-year period and proved an additional reduction of total mortality by 15% (The Scandinavian Simvastatin Survival Study Group. Randomized trial of cholesterol lowering in 4444 patients with coronary heart disease: the Scandinavian Simvastatin Survival Study (4S). Lancet 1994;344:1383-1389) 4S (Scandinavian Simvastatin Survival Study) : In summary
 patients were followed for another 5-year period and proved an additional reduction of total mortality by 15% (The Scandinavian Simvastatin Survival Study Group. Randomized trial of cholesterol lowering in 4444 patients with coronary heart disease: the Scandinavian Simvastatin Survival Study (4S). Lancet 1994;344: ) 4S (Scandinavian Simvastatin Survival Study) : In summary.")
29
SIMVASTATIN: CAUSE-SPECIFIC MORTALITY (10269)(10267)SIMVASTATINPLACEBO Rate ratio & 95% CI STATIN better PLACEBO better Cause of death Vascular 587707 Coronary 194230 Other vascular (7.6%)(9.1%) 17% SE 4 reduction 781937 (2P<0.0001) ANY VASCULAR (5.3%)(5.6%) 5% SE 6 reduction 547570 (NS) NON-VASCULAR (12.9%)(14.7%) 13% SE 4 reduction 13281507 (2P<0.001) ALL CAUSES 0.40.60.81.01.21.4 HPS collaborative group. Lancet 2002;360:7-22.

30
SIMVASTATIN: CORONARY EVENTS & REVASCULARISATION (10269)(10267)SIMVASTATINPLACEBO Rate ratio & 95% CI STATIN better PLACEBO better Major coronary event 357574 Non-fatal MI 587707 Coronary death (8.7%)(11.8%) 27% SE 4 reduction 8981212 (2P<0.00001) CORONARY EVENTS Revascularisation 513725 Coronary 450532 Non-coronary (9.1%)(11.7%) 24% SE 4 reduction 9391205 (2P<0.00001) REVASCULARISATIONS 0.40.60.81.01.21.4 HPS collaborative group. Lancet 2002;360:7-22.

31
SIMVASTATIN: MAJOR VASCULAR EVENTS (10269)(10267)SIMVASTATINPLACEBO Rate ratio & 95% CI STATIN better PLACEBO better Vascularevent 8981212Major coronary 444585Any stroke 9391205Revascularisation (19.8%)(25.2%) 24% SE 3 reduction 20332585 (2P<0.00001) ANY OF ABOVE 0.40.60.81.01.21.4 HPS collaborative group. Lancet 2002;360:7-22.

32
SIMVASTATIN: Main conclusions After allowance for non-compliance, 40mg daily simvastatin safely reduces the risk of heart attack, of stroke, and of revascularisation by about one-third 5 years of statin treatment typically prevents these “major vascular events” in about: 100 of every 1000 people with previous MI 80 " " " other CHD 70 " " " cerebrovascular disease 70 " " " other arterial disease 70 " " " diabetes (age 40+)....irrespective of cholesterol level (or age, or sex, or other treatments)
....irrespective of cholesterol level (or age, or sex, or other treatments)")
33
Evidences for Primary prevention ASCOT (Anglo-Scandinavian Cardiac Outcomes Trial) - clinical benefit of atorvastatin 10 mg / day versus placebo in total 10 305 hypertensive patients with average total cholesterol 5.5 mmol / L, mean levels of LDL-C 3.4 mmol / L and high risk profile. Originally planned for a 5-year follow-up study ASCOT was prematurely terminated due to the obvious benefits. Treatment with atorvastatin decreased the relative risk of cardiovascular events by 36% (P = 0.0005) and stroke - with 27% (P = 0.024). No effect on mortality or differences in the incidence of side effects in different groups. CARDS (The Collaborative Atorvastatin Diabetes Study) - prevention of CVD and CVD (acute coronary events and stroke), featuring high-risk patients with type 2 diabetes and at least one risk factor, but not with elevated levels of cholesterol Due to the proven clinical benefits for patients treated with atorvastatin 10 mg daily compared with placebo the study was discontinued in advance. Reduced the relative risk of: stroke - 41%, acute coronary events - 36%, coronary revascularization - 31%
 and stroke - with 27% (P = 0.024). No effect on mortality or differences in the incidence of side effects in different groups. CARDS (The Collaborative Atorvastatin Diabetes Study) - prevention of CVD and CVD (acute coronary events and stroke), featuring high-risk patients with type 2 diabetes and at least one risk factor, but not with elevated levels of cholesterol Due to the proven clinical benefits for patients treated with atorvastatin 10 mg daily compared with placebo the study was discontinued in advance. Reduced the relative risk of: stroke - 41%, acute coronary events - 36%, coronary revascularization - 31%.")
34
Evidences from ASCOT-LLA Primary end point: Non Fatal MI & Fatal CHD atorvastatin10 mgNo of incidents100 PlaceboNo of incidents 154 36% Reduction HR = 0.64 (0.50-0.83) P =.0005.Sever PS, et al. Lancet. 2003;361:1149-1158. atorvastatin10 mg No of incidents 89 Placebo No of incidents 121 0 1 2 3 0.00.51.01.52.02.53.03.5 Years Cumulative hazard (%) HR = 0.73 (0.56-0.96) P =.0236 27% Reduction Secondary end point : Fatal and non fatal stroke Cumulative hazard (%) Years
 HR = 0.73 ( ) P = % Reduction Secondary end point : Fatal and non fatal stroke Cumulative hazard (%) Years.")
35
Secondary end point : Overall CV events & procedures Secondary end point : Overall Coronary events 0 2 4 6 8 10 12 0.00.51.01.52.02.53.03.5 Years Cumulative hazard (%) 21% Reduction HR = 0.79 (0.69-0.90) P =.0005 atorvastatin10 mg No of incidents 389 Placebo No of incidents 486 atorvastatin10 mg No of incidents 178 Placebo No of incidents 247 0 1 2 3 4 5 6 0.00.51.01.52.02.53.03.5 Years Cumulative hazard (%) 29% Reduction HR = 0.71 (0.59-0.86) P =.0005 Sever PS, et al. Lancet. 2003;361:1149-1158. Evidences from ASCOT-LLA

36
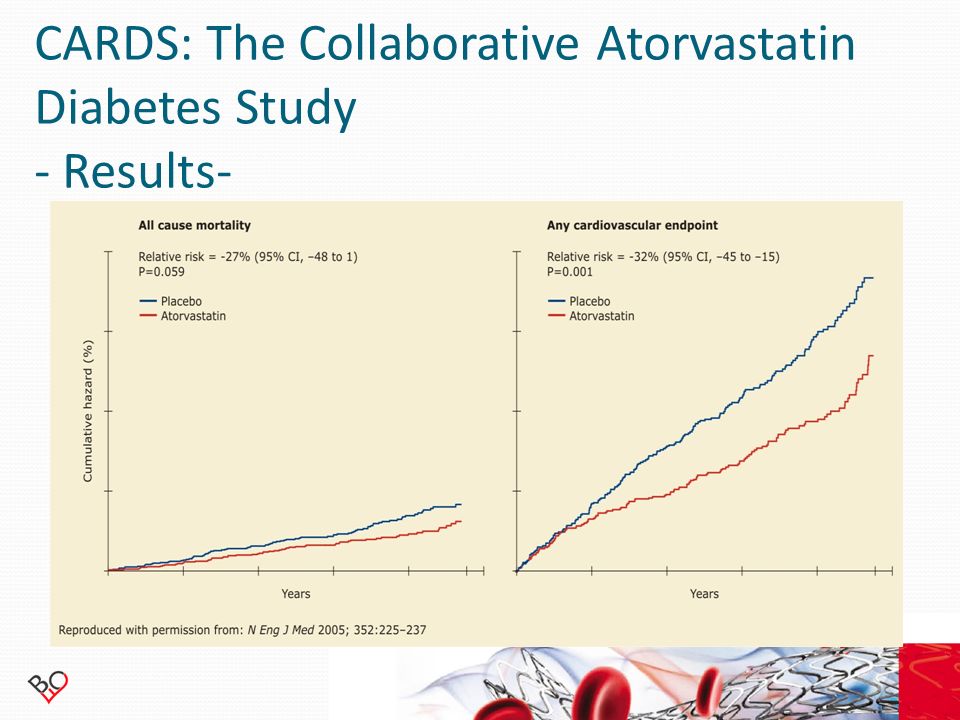
CARDS: The Collaborative Atorvastatin Diabetes Study - Results-

38
CARDS: The Collaborative Atorvastatin Diabetes Study - Summary - Compared with placebo, patients receiving 10 mg atorvastatin daily showed a 37% reduction in major cardiovascular events from 9.0% to 5.8 % (p = 0.001) There was a favourable trend in the atorvastatin group with regard to all cause mortality, acute coronary events, coronary revascularization, and stroke Adverse event rate similar in atorvastatin and placebo groups. No cases of rhabdomyolysis.

39
MIRACL (Myocardial Ischemia Reduction and Aggressive Cholesterol Lowering) – atorvastatin 80 mg versus placebo & PROVE-IT (atorvastatin 80 mg versus pravastatin 40 mg) studied the assumption that early treatment with high doses (80 mg daily) atorvastatin after ACS would have clinically significant benefits. TNT (Treating to New Targets) - maximum doses of atorvastatin (80 mg daily) decreased the mean LDL-C of about 2.6 to 2.0 mmol / L, and the incidence of serious cardiovascular events was reduced by 22% compared with the lower dose (10 mg daily) Evidences for Secondary prevention Summary: In patients with ACS, intensive lipid lowering therapy has a better protective effect (death and major CV events) compared with standard therapy.
 - maximum doses of atorvastatin (80 mg daily) decreased the mean LDL-C of about 2.6 to 2.0 mmol / L, and the incidence of serious cardiovascular events was reduced by 22% compared with the lower dose (10 mg daily) Evidences for Secondary prevention Summary: In patients with ACS, intensive lipid lowering therapy has a better protective effect (death and major CV events) compared with standard therapy..")
40
MIRACL Worsening Angina With New Objective Evidence of Ischemia and Emergency Re-hospitalization Relative risk = 0.74 P=0.018 Atorvastatin Placebo Time Since Randomization (Weeks) Cumulative Incidence (%) 15 10 5 0 0481216 26%
 Cumulative Incidence (%) %")
41
MIRACL Fatal and non fatal Stroke 0 0.5 1 1.5 2 0481216 Relative risk= 0.50 p=0.045 95% CI 0.26-0.99 Atorvastatin 80 mg Placebo Data on file, Pfizer Inc. 50% Time Since Randomization (Weeks) Cumulative Incidence (%)
 Cumulative Incidence (%).")
42
MIRACL Inflammatory Marker Results MIRACL Inflammatory Marker Results -74%-83% } - 34 %

43
PROVE IT: Pravastatin or Atorvastatin Evaluation and Infection Therapy - Results - Cannon et al. N Engl J Med 2004;350:1495–1504. Months after randomization Endpoint rate (%) 0 0 612182430 5 10 15 20 25 30 Primary endpoint: death or major cardiovascular event Standard-dose pravastatin High-dose atorvastatin P = 0.005 Relative risk 0,50 (95% CI 5–26%) 16%
 Primary endpoint: death or major cardiovascular event Standard-dose pravastatin High-dose atorvastatin P = Relative risk 0,50 (95% CI 5–26%) 16%.")
44
Cannon et al.N Engl J Med 2004;350:1495–1504. Secondary endpoints and components of primary endpoint 1.001.500.50 Death from any cause Death from CHD Death from other causes MI Death or MI Death from CHD or MI Revascularization MI, revascularization or death from CHD Unstable angina requiring hospitalization Stroke Hazard ratio (95% CI) High-dose atorvastatin better Standard-dose pravastatin better PROVE IT: Pravastatin or Atorvastatin Evaluation and Infection Therapy - Results -
 High-dose atorvastatin better Standard-dose pravastatin better PROVE IT: Pravastatin or Atorvastatin Evaluation and Infection Therapy - Results -.")
45
PROVE IT: Pravastatin or Atorvastatin Evaluation and Infection Therapy - Summary - Compared with standard-dose pravastatin, high-dose atorvastatin group had significantly reduced: — median LDL cholesterol (62 vs. 95 mg/dL, 1.60 vs. 2.46 mmol/L, P<0.001) — primary endpoint of all-cause mortality, MI, unstable angina, revascularization and stroke (22.4 vs. 26.3%, P=0.005) — MI, revascularization or death from CHD (19.7 vs. 22.3%, P=0.029) — revascularization (16.3 vs. 18.8%, P=0.04) and unstable angina (3.8 vs. 5.1%, P=0.02) Trend towards reduced death (2.2 vs. 3.2%, P=0.07) and death or MI (8.3 vs. 10%, P=0.06) with high dose, but not significant Early benefit of high-dose atorvastatin was consistent over time Standard- and high-dose regimens equally tolerated as defined by similar discontinuation rates (33 vs. 30%, P=0.11)
 — primary endpoint of all-cause mortality, MI, unstable angina, revascularization and stroke (22.4 vs. 26.3%, P=0.005) — MI, revascularization or death from CHD (19.7 vs. 22.3%, P=0.029) — revascularization (16.3 vs. 18.8%, P=0.04) and unstable angina (3.8 vs. 5.1%, P=0.02) Trend towards reduced death (2.2 vs. 3.2%, P=0.07) and death or MI (8.3 vs. 10%, P=0.06) with high dose, but not significant Early benefit of high-dose atorvastatin was consistent over time Standard- and high-dose regimens equally tolerated as defined by similar discontinuation rates (33 vs. 30%, P=0.11).")
46
TNT: Treating to New Targets Primary end point Relative risk = 0.78 P=0.026 Atorvastatin 80 mg Atorvastatin 10 mg Time Since Randomization (Weeks) Cumulative Incidence (%) 15 10 5 0 0481216 25% Major cardiovascular events (diabetes group) Diabetes Care. 2006;29(6):1220-1226. © 2006 American Diabetes Association, Inc.
: © 2006 American Diabetes Association, Inc..")
47
The TNT study confirmed and extended the growing body of evidence indicating that lowering LDL cholesterol to values well below currently recommended levels with more intensive statin therapy is associated with additional cardiovascular benefit. The current sub-analysis of the TNT study indicates that these benefits are consistent in patients with diabetes and CHD. For secondary outcomes (any cardiovascular event, major coronary event (CHD death, nonfatal non procedure-related myocardial infarction, or resuscitated cardiac arrest), any coronary event, cerebrovascular event etc.), intensive therapy with atorvastatin 80 mg significantly reduced the rate of all cardiovascular events and cerebrovascular events compared with atorvastatin 10 mg. In 2005, the ADA updated its clinical practice recommendations for patients with diabetes and cardiovascular disease, noting that these individuals are at very high risk for subsequent clinical events. On the basis of randomized trials of moderate versus intensive lipid lowering in very-high-risk (albeit nondiabetic) populations, the ADA advised that use of high-dose statin to achieve an LDL cholesterol level of < 1,8 mmol/l was a therapeutic option in diabetic patients with cardiovascular disease TNT: Treating to New Targets Conclusions
, any coronary event, cerebrovascular event etc.), intensive therapy with atorvastatin 80 mg significantly reduced the rate of all cardiovascular events and cerebrovascular events compared with atorvastatin 10 mg. In 2005, the ADA updated its clinical practice recommendations for patients with diabetes and cardiovascular disease, noting that these individuals are at very high risk for subsequent clinical events. On the basis of randomized trials of moderate versus intensive lipid lowering in very-high-risk (albeit nondiabetic) populations, the ADA advised that use of high-dose statin to achieve an LDL cholesterol level of < 1,8 mmol/l was a therapeutic option in diabetic patients with cardiovascular disease TNT: Treating to New Targets Conclusions.")
48
48 SPARCL: Stroke Prevention by Aggressive Reduction in Cholesterol Levels (≥ 50% vs. < 50% reduction in LDL-cholesterol). N Engl J Med. 2006;355:459-559.
. N Engl J Med. 2006;355:")
49
49 SPARCL: Stroke Prevention by Aggressive Reduction in Cholesterol Levels (≥ 50% vs. < 50% reduction in LDL-cholesterol). N Engl J Med. 2006;355:459-559.
. N Engl J Med. 2006;355:")
50
SPARCL: Stroke Prevention by Aggressive Reduction in Cholesterol Levels -Summary- The only study to date, which is directly evaluated the effectiveness of atorvastatin 80 mg for the reduction of risk of occurrence of fatal or nonfatal stroke in patients experienced stroke or transient ischemic attack within the past 6 months without evidence of CHD Post-hoc analysis: Atorvastatin reduced the relative risk for occurrence of ischemic stroke by 22% (p = 0.01) and the risk of occurrence of undifferentiated stroke by 45% (p = 0,01) N Engl J Med. 2006;355:459-559.

51
ASTEROID: Relationship between mean LDL-C levels and median change in percent atheroma volume for several intravascular ultrasound trials Nissen SE, et al. JAMA 2006;295:1556. Mean LDL-C (mg/dL) –1.2 –0.6 0 0.6 1.2 1.8 50 708090100110120 Mean change in percent atheroma volume, % 60 CAMELOT placebo A-Plus placebo REVERSAL atorvastatin REVERSAL pravastatin ASTEROID rosuvastatin r 2 =0.97 p<0.001
 –1.2 – Mean change in percent atheroma volume, % 60 CAMELOT placebo A-Plus placebo REVERSAL atorvastatin REVERSAL pravastatin ASTEROID rosuvastatin r 2 =0.97 p<")
52
ASTEROID -Summary- ASTEROID 40-mg rosuvastatin daily LDL-C reaching an average of 2,32 mmol/L HDL-C increase of 15% No progression seen with IVUS Possibly some regression A great study moving us toward lower LDL-C In the future, in the high-risk population, LDL-C targets may be as low as 1,93 mmol/L

53
According to evidence-based medicine… The most important indicator for reducing cardiovascular risk is LDL-C For the best control of high-risk patients (all patients with coronary artery disease,pateints after invasive procedures, diabetes or cerebrovascular disease) should achieve optimal levels of LDL-C According to U.S. recommendations (ATP III) and European recommendations (ESC 2011), the optimal level of LDL-C was 1,8 mmol / l “LDL-C and HDL-C - Is their unique effect on atherosclerosis?” Ass.Prof. Ivo Petrov – Head of Cardiology clinic, Tokuda hospital Sofia.
 and European recommendations (ESC 2011), the optimal level of LDL-C was 1,8 mmol / l LDL-C and HDL-C - Is their unique effect on atherosclerosis Ass.Prof. Ivo Petrov – Head of Cardiology clinic, Tokuda hospital Sofia..")
54
Algorithm for treatment recommended by the ESC 2011 1. Assessment of total cardiovascular risk of patients 2. Involving patients in decisions about the management of cardiovascular risk 3. Identification of target LDL-C, depending on the level of risk 4. Calculate the percentage reduction in LDL-C, necessary to achieve target. 5. Choice of statin, which on average can provide this reduction. 6. Due to the response of statin treatment is different, increasing the dose until the target is mandatory! 7. If statins can not achieve the goal, consider drug combinations. Patient's clinical condition, concomitant drug treatment and tolerance will determine behavior in determining the final choice of medication and dosage.

55
Statins in risk reduction Actalipid (simvastatin) Luvinsta (fluvastatin) Lipopres (lovastatin) Torvalipin (atorvastatin) Tintaros (rosuvastatin)
 Luvinsta (fluvastatin) Lipopres (lovastatin) Torvalipin (atorvastatin) Tintaros (rosuvastatin)")
Similar presentations
 Clinical events (morbidity.>")
>")


: Design Cannon CP.>")


>")










 vs. placebo FU 5 years total cholesterol 25%; LDL.>")
>")