Download presentation
Presentation is loading. Please wait.

1
بسم الله الرحمن الرحيم

2
Candida albicans Brought to you by :- Hind Hamed Abed
Medical mycology is a growing field of interest because an increased number of clinical diseases are associated with pathogenic fungi. From athlete’s foot to candidal sepsis, fungi cause a wide range of diseases in humans. More specifically, Candida albicans is a key player in causing genital yeast infections, thrush, and sepsis (Calderone, 2002). Interestingly, C. albicans is an unharmful, commensal organism in the healthy individual. However, when the environmental balance in the body has been tipped, C. albicans becomes virulent. Brought to you by :- Hind Hamed Abed Collage of Medicine ,University of Baghdad
. Interestingly, C. albicans is an unharmful, commensal organism in the healthy individual. However, when the environmental balance in the body has been tipped, C. albicans becomes virulent. Brought to you by :- Hind Hamed Abed. Collage of Medicine ,University of Baghdad.")
3
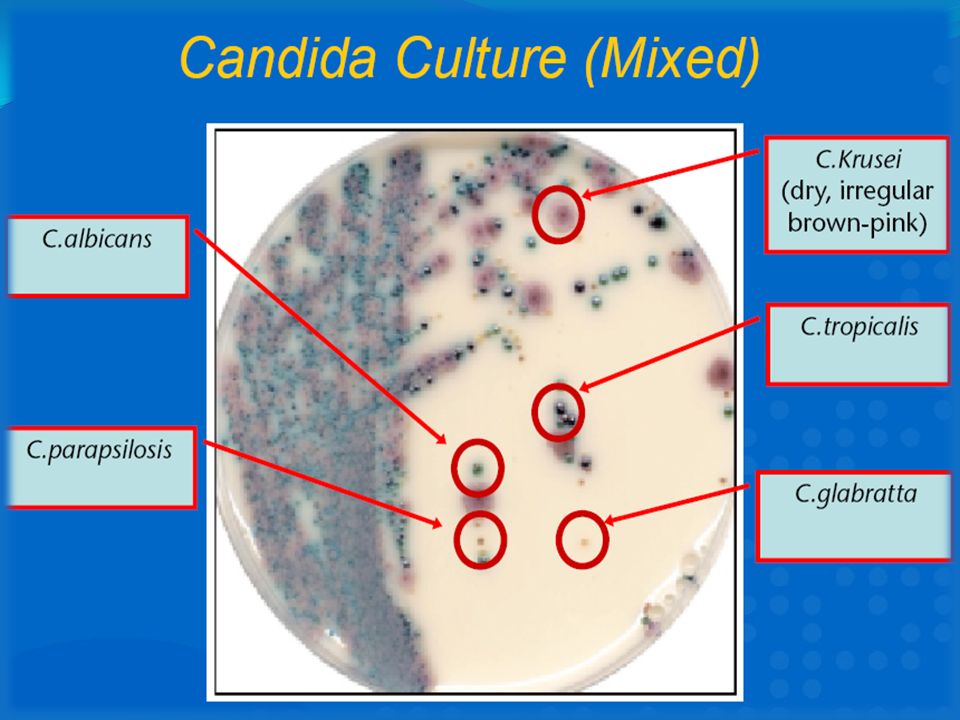
Candida Culture

4
Contents Mycology Basics Introduction Disease capabilities
Pathogenesis Laboratory diagnosis Drug therapy Research This discussion starts with a brief overview of mycology to provide the audience with a background that will aid in understanding the biology of Candida albicans. Thereafter, it will focus on the major diseases caused by C. albicans. How these diseases are possible will be clarified in the discussion of its pathogenesis. Detecting C. albicans and confirming that it is a responsible for a disease that has manifested in a patient is rather recondite. However, the advent of new biotechnological methods has made detection and diagnosis much more feasible. Candidal infections are treated with antifungals, and the different kinds will be discussed. Unfortunately, the rise in incidence of candidal infections and overprescription of antifungals have contributed to an increasing resistance against C. albicans. Therefore, on-going research and attention to medical mycology are necessary to control this organism.

5
Introduction:- - cancer and HIV-AIDs patients.
It is the most common fungal pathogen worldwide -It considered the 4th leading causes of nosocomial infections, &cause 40% mortality -It also made significant mortality and morbidity in low birth-weight infants & affect 75% women, 45% experience recurrence. It account more than > 10 million visits/year - classified as a STD by CDC - cancer and HIV-AIDs patients. - most commonly manifested in patients with leukemia or HIV-AIDs infections. Oral candidiasis is often a clue to acute primary infection. - increasing resistance to drug therapies due to antibiotics and antifungals. Alarmingly, the statistics show how serious infections by C. albicans can be. The CDC has ranked it as the 4th leading pathogen in causing nosocomial bloodstream infections (Naglik et. Al., 2003). Surgical and neonatal intensive care units are dense sources of spread of Candida infections (Roilides et. Al., 2004). Moreover, 75% of women will suffer from a yeast infection at least once in her life (Owen et. Al., 2004). In the U.S., vaginitis accounts for 10 million visits to the physician each year. C. albicans is also considered a sexually transmissable pathogen for one’s ability to contract it though sexual intercourse (Prescott et. Al., 2002). Many environmental factors from taking steroids to being a patient in a hospital can predispose a person to diseases that are caused by C. albicans. These factors will be highlighted later in this discussion.
. Surgical and neonatal intensive care units are dense sources of spread of Candida infections (Roilides et. Al., 2004). Moreover, 75% of women will suffer from a yeast infection at least once in her life (Owen et. Al., 2004). In the U.S., vaginitis accounts for 10 million visits to the physician each year. C. albicans is also considered a sexually transmissable pathogen for one’s ability to contract it though sexual intercourse (Prescott et. Al., 2002). Many environmental factors from taking steroids to being a patient in a hospital can predispose a person to diseases that are caused by C. albicans. These factors will be highlighted later in this discussion.")
6
Mycology Basics Kingdom: Fungi
More than 10 million species, but only ~400 human disease. Sexual Groups Ascomycota Basidiomycota Zygomycota Chytridia Fungi Imperfection Very few species are in a commensally relationship with humans - includes Candida albicans and Malasezia furfur Diseases caused by fungi are usually accidental Endogenous and Exogenous Sources Increasing problem due to antibacterial & immunosuppressive agents Molecular mechanisms of pathogenesis not well-defined Candida albicans belongs in the kingdom Fungi. Over 10 million species exist in this kingdom, of which only approximately 400 species are known to cause disease. Fungi are separated into four major groups that are based on their reproductive structures (Baron, 1996). These groups are Ascomycota, Basidiomycota, Zygomycota, Chytridiomycota, and the Fungi Imperfecti. The classification depends on whether the fungus has the ability to reproduce sexually, asexually, or by a combination of both (Baron, 1996). See Figure 1 on slide 5. The 400 species that are known to cause human diseases belong mainly in the Ascomycota, Basidiomycota, Zygomycota, and Fungi Imperfecti phyla (Kwong-Chung et. Al., 1992). Most of these species are pathogenic, but very few exist as commensal organisms along with their pathogenic potential. Such organisms are Malassezia furfur and Candida albicans (Baron, 1996). The diseases that are caused by fungi are usually accidental, but fungal infection may arise endogenously or exogenously. Endogenously from the internal environment of a human and exogenously from an external environment that has gained internal access by the penetration of the host (Baron, 1996). It is worthwhile to mention that fungal diseases are a problem in today’s world as the number of disease associated with fungal infections rises, in large part, due to a increased episode of antibacterial and immunosuppressive agent therapies (Baron, 1996). In addition, while the molecular mechanisms of pathogenesis in bacteria are extensively known, the mechanisms in fungi are limited and require much more research (Baron, 1996).
. These groups are Ascomycota, Basidiomycota, Zygomycota, Chytridiomycota, and the Fungi Imperfecti. The classification depends on whether the fungus has the ability to reproduce sexually, asexually, or by a combination of both (Baron, 1996). See Figure 1 on slide 5. The 400 species that are known to cause human diseases belong mainly in the Ascomycota, Basidiomycota, Zygomycota, and Fungi Imperfecti phyla (Kwong-Chung et. Al., 1992). Most of these species are pathogenic, but very few exist as commensal organisms along with their pathogenic potential. Such organisms are Malassezia furfur and Candida albicans (Baron, 1996). The diseases that are caused by fungi are usually accidental, but fungal infection may arise endogenously or exogenously. Endogenously from the internal environment of a human and exogenously from an external environment that has gained internal access by the penetration of the host (Baron, 1996). It is worthwhile to mention that fungal diseases are a problem in today’s world as the number of disease associated with fungal infections rises, in large part, due to a increased episode of antibacterial and immunosuppressive agent therapies (Baron, 1996). In addition, while the molecular mechanisms of pathogenesis in bacteria are extensively known, the mechanisms in fungi are limited and require much more research (Baron, 1996).")
7
The 5 main groups Classification of Fungi. Fungi are classified
Fungi are classified into five main groups based on their sexual/asexual reproductive abilities and structures. What should be noted here is that C. albicans exists as an asexual (imperfect) yeast. The phylum Fungi Imperfecti is unique in that species under this group do not have a sexual stage (Baron, 1996). Budding yeasts is the most common form of asexual reproduction, and is key to the growth of c. albicans. C. albicans is also recognized by its ability to form chlamydospores by the conversion of its hyphal elements (Baron, 1996). Classification of Fungi. Fungi are classified based on their ability to reproduce sexually, asexually, by a combination of both. The different reproductive structures places them in the appropriate category. (Baron, 1996)
 yeast. The phylum Fungi Imperfecti is unique in that species under this group do not have a sexual stage (Baron, 1996). Budding yeasts is the most common form of asexual reproduction, and is key to the growth of c. albicans. C. albicans is also recognized by its ability to form chlamydospores by the conversion of its hyphal elements (Baron, 1996). Classification of Fungi. Fungi are classified. based on their ability to reproduce sexually, asexually, by a. combination of both. The different reproductive structures. places them in the appropriate category. (Baron, 1996)")
8
Fungal Characteristics
Plant-like lacking chlorophyll Cell wall chitinous matrix Free-living saprobes and heterotrophy needs Carbon source and Nitrogen source Yeasts or Molds or both Success of an infection Accidental Overcoming host barriers Presiding in host with immunological defects Fungi are eukaryotic cells that look like plant cells, but lack cholorophyll. They possess a cell wall that is made up of chitinous myofibrils that are embedded into a matrix with polysaccharides, proeins, lipids, inorganic salts, and pigments that provide structural rigidity. The major polysaccharides are glucans, mannans, chitosan, and galactans (Baron, 1996). Glucans are a large group of D-glucose polymers that are linked by glycosidic bonds. Mannans are mannose polyers with -D-mannan backbones. Chitosan are polymers of glucosamine and galactans are polymers of galactose. The proportions of these cell wall polymers differ from fungus to fungus. The cell wall of C. albicans, for instance, contains 30-60% glucan, 25-50% mannan, 1-2% chitin, 2-14% lipid, and 5-15% protein (Baron, 1996). Studies have indiciated that the mannans and galactomannans are key players in the immunological response to many yeasts and moulds. Morever, identifying serum concentrations of mannan from clinical samples has been a useful diagnostic technique for determining patients with disseminated candiddiasis (Baron, 1996). The plasma membrane of a fungus is similar to mammalian plasma membranes. Its main difference lies in the presence of nonpolar sterol ergosterol rather than cholesterol (Baron, 1996). Ergosterol is significant in its role of drugs that target fungal diseases and a role in making one who is on steroid treatment more susceptible to yeast infections. These relationships will become clearer throughout the discussion. Fungi are free-living saprobes that nourishes from non-living or decaying organic matter. They cannot synthesize their own food and are therefore heterophic, depending on complex organic substances for nutrition (Kwong-Chung et. Al., 2992). Carbon is needed for the synthesis of carbohydrates, lipids, nucleic acids, and proteins. Nitrogen is also a much needed molecule for the synthesis of amino acids and nucleic acids. Fungi may exist as yeast, mould, or an interchanging phase of both. Yeasts are unicellular, solitary rounded cells while moulds are filamentous. See Figure 1 and Figure 2 on slide 6. Fungi that are yeasts reproduce by budding while moulds reproduce by hyphae formation. See Figure 1 on slide 7 and Figure 2 on slide 8. The budding cells of yeasts are known as blastoconidia. This formation involves three stages: bud emergence, bud growth, and conidium separation (Baron, 1996). See Figure 1 on slide 7. Mould spores, on the other hand, grow hyphae into masses called mycelium by elongation. Although C. albicans oftentimes referred to as a yeast, it has a dual morphology (dimorphic) that allows it to be a yeast but alternate to a mould form, as well (Kwong-Chung et. Al.,1992). As mentioned before, fungi do not usually cause disease, and when they do, disease is a result of an accidental penetration of host barriers or the condition of an immunological defect in the host. When a fungus gains entry into the host from an exogenous source or is capable of growing from an endogenous source, it often develops virulence mechanisms that help it adapt and grow in its new environment. Some fungi are quite comfortable at 37 C and can assume many morphological forms like yeasts, hyphae, and pseudohyphae to facilitate their rapid multiplication and dissemination in the host (Baron, 1996). Penicillium chrysogenum
. Glucans are a large group of D-glucose polymers that are linked by glycosidic bonds. Mannans are mannose polyers with -D-mannan backbones. Chitosan are polymers of glucosamine and galactans are polymers of galactose. The proportions of these cell wall polymers differ from fungus to fungus. The cell wall of C. albicans, for instance, contains 30-60% glucan, 25-50% mannan, 1-2% chitin, 2-14% lipid, and 5-15% protein (Baron, 1996). Studies have indiciated that the mannans and galactomannans are key players in the immunological response to many yeasts and moulds. Morever, identifying serum concentrations of mannan from clinical samples has been a useful diagnostic technique for determining patients with disseminated candiddiasis (Baron, 1996). The plasma membrane of a fungus is similar to mammalian plasma membranes. Its main difference lies in the presence of nonpolar sterol ergosterol rather than cholesterol (Baron, 1996). Ergosterol is significant in its role of drugs that target fungal diseases and a role in making one who is on steroid treatment more susceptible to yeast infections. These relationships will become clearer throughout the discussion. Fungi are free-living saprobes that nourishes from non-living or decaying organic matter. They cannot synthesize their own food and are therefore heterophic, depending on complex organic substances for nutrition (Kwong-Chung et. Al., 2992). Carbon is needed for the synthesis of carbohydrates, lipids, nucleic acids, and proteins. Nitrogen is also a much needed molecule for the synthesis of amino acids and nucleic acids. Fungi may exist as yeast, mould, or an interchanging phase of both. Yeasts are unicellular, solitary rounded cells while moulds are filamentous. See Figure 1 and Figure 2 on slide 6. Fungi that are yeasts reproduce by budding while moulds reproduce by hyphae formation. See Figure 1 on slide 7 and Figure 2 on slide 8. The budding cells of yeasts are known as blastoconidia. This formation involves three stages: bud emergence, bud growth, and conidium separation (Baron, 1996). See Figure 1 on slide 7. Mould spores, on the other hand, grow hyphae into masses called mycelium by elongation. Although C. albicans oftentimes referred to as a yeast, it has a dual morphology (dimorphic) that allows it to be a yeast but alternate to a mould form, as well (Kwong-Chung et. Al.,1992). As mentioned before, fungi do not usually cause disease, and when they do, disease is a result of an accidental penetration of host barriers or the condition of an immunological defect in the host. When a fungus gains entry into the host from an exogenous source or is capable of growing from an endogenous source, it often develops virulence mechanisms that help it adapt and grow in its new environment. Some fungi are quite comfortable at 37 C and can assume many morphological forms like yeasts, hyphae, and pseudohyphae to facilitate their rapid multiplication and dissemination in the host (Baron, 1996). Penicillium chrysogenum")
9
Candida •Candida is a yeast like fungus which inhabits almost all humans. •Most common cause of opportunistic mycoses worldwide. •The genusCandida includes around 154 species. •6 are most frequently isolated in human infections. •Candida albicans is the most abundant & pathogenic. •C. tropicalis; C. glabrata; C. parapsilosis; C.kusei; & C. lusitaniae,causative human infective agents. •Geotrichum is yeast found worldwide in soil, water, air & sewage. A coloniser of human intestinal tract.

10
Candida •It lives in the moist dark mucous membranes which line the mouth, vagina and intestinal tract. •Ordinarily it exists only in small colonies. Prevented from growing too rapidly by the human host’s immune system, and by competition from other microorganisms in and on the body’s mucous membranes. •When this delicate balance is upset, candida can grow rapidly and aggressively, causing many unpleasant symptoms.

11
Yeast Characteristics Mould Characteristics
solitary, unicellular reproduction via budding rounded shape moist & mucoid colonies Mould Characteristics filamentous hyphae hyphal formation tips may be rounded (conidia/spores) This slide shows the typical yeast and typical mould. Yeasts and moulds are two main broad, morphological groups of fungi. Candida albicans is referred to as a yeast, but has characteristics of both morphologies (Baron, 1996). Figure 1. Typical Yeast Figure 2. Typical mould
 This slide shows the typical yeast and typical mould. Yeasts and moulds are two main broad, morphological groups of fungi. Candida albicans is referred to as a yeast, but has characteristics of both morphologies (Baron, 1996). Figure 1. Typical Yeast. Figure 2. Typical mould.")
12
Saccharomyces sp. Different strains of Saccharomyces are used in
brewing and baking (right) Candida albicans, also a unicellular yeast, causes Candidiasis (thrush) infections in humans. © Dennis Kunkel (
 Candida albicans, also a unicellular yeast, causes. Candidiasis (thrush) infections. in humans. © Dennis Kunkel (")
13
Sporangia and Spores of the Penicillium sp.
Fungal hyphae with fruiting structure (r). Similar fungi are the skin-inhabiting dermatophytes of the Epidermophyton and Microspores groups © Dennis Kunkel (
. Similar fungi are the. skin-inhabiting. dermatophytes of the. Epidermophyton and. Microspores groups. © Dennis Kunkel (")
14
Fungi-yeasts: Candida albicans

15
Yeast Bud Formation Hyphal Formation Stages of bud growth and
This slide shows the formation of a yeast bud. Bud cell emergence is regulated by turgor pressure in the parent cell and by the synthesis of cellular materials that have been activated by a polysaccharide synthetase zymogen. As the bud emerges, the cell of wall the parent things, microtubules elongate into spindle microtubules, and a pinching at the end of the cell begins. This emerging bud is the blastoconidium, and a ring of chitin forms between the blastoconidium and the parent cell to encourage a separation when the ring forms a septal wall. A bud scar might be produced. However, if the blastoconidia continue to develop without separating from the parent, structures called pseudohyphae form. This can be visualized as a filament of attached blastoconidia. C. albicans has the ability to form budding yeast cells, pseudohyphae, and true hyphae (Baron, 1996). Stages of bud growth and yeast cell cycle (Baron et. Al., 1996) Polarized hyphal formation (Baron et. Al., 1996)
. Stages of bud growth and. yeast cell cycle (Baron et. Al., 1996) Polarized hyphal formation (Baron et. Al., 1996)")
16
Pathogenesis Host Recognition Adhesions Enzymes
Hydrolysis: Phosphoplipases, Lipases, Proteinases 4.Morphogenesis Yeast form to Filamentous hyphae/pseudohyphae 5.Phenotypic Switching Without its virulence factors, Candida albicans would not survive in the human body. The major mechanisms of its pathogenesis come in the form of host recognition, the production of enzymes, the ability to assume different morphologies, and the capacity to switch phenotypically (Calderone & Gow, 2002). Host Recognition Host recognition involves key players called adhesins (Calderone & Gow, 2002), which also contribute to colonization. In studies where genes that encoded for adhesions were deleted, C. albicans demonstrated the inability to adhere onto the host and as a result, infection did not proceed (Calderon & Gow, 2002). Thus, adhesion is a major virulence determinant of C. albicans. What prompted these studies of adherence factors were investigations led by King et. al. in the 1980s. An assay was developed to measure the adherence of several species in Candida by using radiolabeled Candida species that were added to human buccal or vaginal exfoliated cells in a suspension. Filters removed non-adhering yeasts and adherence was measured by the amount of radiolabeled yeast cells left. The studies revealed that C. albicans adhered most significantly and to the greatest extent (Calderone & Gow, 2002). Adhesins are either polysaccharide or glycoprotein, but are more abundant as glycoproteins (Calderone & Gow, 2002). Types of adhesins include MP66 whose ligand is Asialoglcospingolipid, MP-hemed whose ligand is fibronectin, and Ala1p whose ligand is also fibronectin (Cormack et. al., 1999). Not only do adhesins allow C. albicans to bind to human epithelial cells, but also to human proteins and internal tissues (Calderone & Gow, 2002). The adherence onto plastic surfaces by C. albicans is yet another growing problem that exacerbates the spread of candidiasis in hospital settings. The contamination of indwelling catheters in patient pools often initiates systemic candidiasis (Jarvis, 1995). Plastics also have the great capacity to collect biofilms, which promotes the adherence of C. albicans. In studies that focused on the adherence of C. albicans to different medical catheters, it was found that polyvinyl catheters supported the most for biofilm formation and polyurethane supported it the least (Hawser & Douglas, 1994). Of all the species of Candida that were tested, C. albicans contributed to the most biofilm mass (Hawser & Douglas, 1994). This nature is an important one for experimental investigation because it could correlate with organisms that are embedded in biofilms have more resistance to antifungal drugs. Recent studies have shown that there is an increased resistance to amphotericin B for organisms that are in a biofilm (Baillie and Douglas, 1999). Enzyme Hydrolases Gaining entry into the host is an important strategy for C. albicans and many other pathogenic organisms. To aid in doing so, C. albicans produces hydrolytic digestive enzymes such as the secreted aspartyl proteinases (SAPs) and phospholipase B (PLB) (Calderone & Gow, 2002). Hydrolytic enzymes play a central role in the pathogenesis of C. albicans, just as they do in many other pathogenic fungi, bacteria, and protozoa (Naglik et. Al., 2003). In contrast to bacteria, C. albicans tends to produce hydrolytic enzymes that are broad-spectrum rather than highly-substrate specific (Hube and Naglik, 2002). Hydrolytic enzymes serve multiple purposes from the digestion of molecules for nutrient absorption to host tissue invasion by the destruction of cell membranes (Hube and Naglik, 2002). Three major categories of hydrolytic enzymes are known to be involved with C. albicans’ virulence (Hube and Naglik, 2002). These enzymes are proteinases, phospholipases, and lipases (Naglik et. al., 2003). Proteinases hydrolyze peptide bonds, phospholipases hydrolyzes phospholipids, and lipases hydrolyze lipids. More specifically, C. albicans secrete aspartyl proteinases, PLB2, PLB2, and PLD-type phospholipases, and Lip1 through Lip10 lipases (Ghannoum, 2000). It has been purported that the phospholipases enhance virulence by mediating the adhesion and lyssis of host cell membranes during an infection (Ghannoum, 2000). While evidence implicates these findings, more research is needed to determine the actual relationship and mechanism (Ghannoum, 2000). Further study on lipases is also necessary to understand their involvement in the organism’s pathogenesis. However, it has been implicated that the broad lipolytic activity may contribute to its persistence and virulence (Hube and Naglik, 2002). The secreted aspartyl proteinases are encoded by a family of ten SAP genes and are concluded to be key virulence determinants of Candida albicans (Felk et. al., 2000). Studies have shown their involvement in hyphal formation, adhesion, and phenotypic switching (Naglik et. al., 2002). The correlation between SAP and Candida virulence has been determined by isolating C. albicans from various candidal diseases and noting the SAP activity. For instance, increased SAP activity occurred in C. albicans strains that were isolated form HIV-positive patients with oral candidiasis compared with HIV-negative C. albicans strains carriers (De Bernardis et. al., 19992). The same effect was found in isolates from patients with oropharyngeal candidiasis and vaginal candidiasis. In animal models, the strains with more SAP production led to higher levels of tissue colonization in the liver, kidneys, and spleen (Abu-Elteen et. al., 2001). Ten different kinds of SAP have been identified that range in size from 35 to 50 kDA. SAP1 to SAP3 execute high activity at a low pH while SAP4 to SAP6 execute high activity at a high pH (Naglik et. al., 2003). The different optimal pH levels for each SAP may be an evolutionary advantage for proteinases to adapt to varying kinds of environment. For instance, the pH of the oral cavity is different than the pH of the gastrointestinal tract, and C. albicans would have to demonstrate the ability to survive in each one. SAP is also significant for facilitating the adherence of C. albicans onto host cells and tissues followed by the degradation of host proteins (Naglik et. al., 2003). It is also found to play some role in hyphal formation and in the regulation of phenotypic switching, which enhances C. albicans’ virulence (Naglik et. al., 2003). The molecular mechanisms are unclear, however, and more research is necessary. Morphogenesis The characteristic that C. albicans is dimorphic and can convert from yeast buds to filamentous hyphae/pseudohyphae under varying conditions indicates another virulent property. One study of an isolated C. albicans strain that was regulated for suppressed hyphal growth was found to be avirulent in an animal mouse model compared to its wild type (Calderone & Gow, 2002). Moreover, the normal environment of the vagina is a classic example to illustrate the non-pathogenic and pathogenic nature of C. albicans. In normal healthy individuals, C. albicans exists as yeast whose growth is mainly suppressed by beneficial bacteria that reside in the vagina. When C. albicans turns virulent, however, its morphology changes into filamentous hyphae (Brown, 2002). Phenotypic Switching The ability for C. albicans to undergo phenotypic switching is a postulated mechanism of virulence. Switching could changes in the expression of cell-surface antigens, tissue affinities of the organism, enzyme production, and drug sensitivity (Calderone & Gow, 2002). Switching also had profound effects on the susceptiblity to antifungal drugs, producing strains that are resistant (Vargas et. al., 2000).
. Host Recognition. Host recognition involves key players called adhesins (Calderone & Gow, 2002), which also contribute to colonization. In studies where genes that encoded for adhesions were deleted, C. albicans demonstrated the inability to adhere onto the host and as a result, infection did not proceed (Calderon & Gow, 2002). Thus, adhesion is a major virulence determinant of C. albicans. What prompted these studies of adherence factors were investigations led by King et. al. in the 1980s. An assay was developed to measure the adherence of several species in Candida by using radiolabeled Candida species that were added to human buccal or vaginal exfoliated cells in a suspension. Filters removed non-adhering yeasts and adherence was measured by the amount of radiolabeled yeast cells left. The studies revealed that C. albicans adhered most significantly and to the greatest extent (Calderone & Gow, 2002). Adhesins are either polysaccharide or glycoprotein, but are more abundant as glycoproteins (Calderone & Gow, 2002). Types of adhesins include MP66 whose ligand is Asialoglcospingolipid, MP-hemed whose ligand is fibronectin, and Ala1p whose ligand is also fibronectin (Cormack et. al., 1999). Not only do adhesins allow C. albicans to bind to human epithelial cells, but also to human proteins and internal tissues (Calderone & Gow, 2002). The adherence onto plastic surfaces by C. albicans is yet another growing problem that exacerbates the spread of candidiasis in hospital settings. The contamination of indwelling catheters in patient pools often initiates systemic candidiasis (Jarvis, 1995). Plastics also have the great capacity to collect biofilms, which promotes the adherence of C. albicans. In studies that focused on the adherence of C. albicans to different medical catheters, it was found that polyvinyl catheters supported the most for biofilm formation and polyurethane supported it the least (Hawser & Douglas, 1994). Of all the species of Candida that were tested, C. albicans contributed to the most biofilm mass (Hawser & Douglas, 1994). This nature is an important one for experimental investigation because it could correlate with organisms that are embedded in biofilms have more resistance to antifungal drugs. Recent studies have shown that there is an increased resistance to amphotericin B for organisms that are in a biofilm (Baillie and Douglas, 1999). Enzyme Hydrolases. Gaining entry into the host is an important strategy for C. albicans and many other pathogenic organisms. To aid in doing so, C. albicans produces hydrolytic digestive enzymes such as the secreted aspartyl proteinases (SAPs) and phospholipase B (PLB) (Calderone & Gow, 2002). Hydrolytic enzymes play a central role in the pathogenesis of C. albicans, just as they do in many other pathogenic fungi, bacteria, and protozoa (Naglik et. Al., 2003). In contrast to bacteria, C. albicans tends to produce hydrolytic enzymes that are broad-spectrum rather than highly-substrate specific (Hube and Naglik, 2002). Hydrolytic enzymes serve multiple purposes from the digestion of molecules for nutrient absorption to host tissue invasion by the destruction of cell membranes (Hube and Naglik, 2002). Three major categories of hydrolytic enzymes are known to be involved with C. albicans’ virulence (Hube and Naglik, 2002). These enzymes are proteinases, phospholipases, and lipases (Naglik et. al., 2003). Proteinases hydrolyze peptide bonds, phospholipases hydrolyzes phospholipids, and lipases hydrolyze lipids. More specifically, C. albicans secrete aspartyl proteinases, PLB2, PLB2, and PLD-type phospholipases, and Lip1 through Lip10 lipases (Ghannoum, 2000). It has been purported that the phospholipases enhance virulence by mediating the adhesion and lyssis of host cell membranes during an infection (Ghannoum, 2000). While evidence implicates these findings, more research is needed to determine the actual relationship and mechanism (Ghannoum, 2000). Further study on lipases is also necessary to understand their involvement in the organism’s pathogenesis. However, it has been implicated that the broad lipolytic activity may contribute to its persistence and virulence (Hube and Naglik, 2002). The secreted aspartyl proteinases are encoded by a family of ten SAP genes and are concluded to be key virulence determinants of Candida albicans (Felk et. al., 2000). Studies have shown their involvement in hyphal formation, adhesion, and phenotypic switching (Naglik et. al., 2002). The correlation between SAP and Candida virulence has been determined by isolating C. albicans from various candidal diseases and noting the SAP activity. For instance, increased SAP activity occurred in C. albicans strains that were isolated form HIV-positive patients with oral candidiasis compared with HIV-negative C. albicans strains carriers (De Bernardis et. al., 19992). The same effect was found in isolates from patients with oropharyngeal candidiasis and vaginal candidiasis. In animal models, the strains with more SAP production led to higher levels of tissue colonization in the liver, kidneys, and spleen (Abu-Elteen et. al., 2001). Ten different kinds of SAP have been identified that range in size from 35 to 50 kDA. SAP1 to SAP3 execute high activity at a low pH while SAP4 to SAP6 execute high activity at a high pH (Naglik et. al., 2003). The different optimal pH levels for each SAP may be an evolutionary advantage for proteinases to adapt to varying kinds of environment. For instance, the pH of the oral cavity is different than the pH of the gastrointestinal tract, and C. albicans would have to demonstrate the ability to survive in each one. SAP is also significant for facilitating the adherence of C. albicans onto host cells and tissues followed by the degradation of host proteins (Naglik et. al., 2003). It is also found to play some role in hyphal formation and in the regulation of phenotypic switching, which enhances C. albicans’ virulence (Naglik et. al., 2003). The molecular mechanisms are unclear, however, and more research is necessary. Morphogenesis. The characteristic that C. albicans is dimorphic and can convert from yeast buds to filamentous hyphae/pseudohyphae under varying conditions indicates another virulent property. One study of an isolated C. albicans strain that was regulated for suppressed hyphal growth was found to be avirulent in an animal mouse model compared to its wild type (Calderone & Gow, 2002). Moreover, the normal environment of the vagina is a classic example to illustrate the non-pathogenic and pathogenic nature of C. albicans. In normal healthy individuals, C. albicans exists as yeast whose growth is mainly suppressed by beneficial bacteria that reside in the vagina. When C. albicans turns virulent, however, its morphology changes into filamentous hyphae (Brown, 2002). Phenotypic Switching. The ability for C. albicans to undergo phenotypic switching is a postulated mechanism of virulence. Switching could changes in the expression of cell-surface antigens, tissue affinities of the organism, enzyme production, and drug sensitivity (Calderone & Gow, 2002). Switching also had profound effects on the susceptiblity to antifungal drugs, producing strains that are resistant (Vargas et. al., 2000).")
17
Virulence assay of different C
Virulence assay of different C. albicans strains using the skin equivalent (AST 2000) Figure 1. skin equivalent before infection Figure 2. Infection with pathogenic clinical isolate of C. albicans. After 48 h the yeast penetrates the skin equivalent and destroys the tissue This slide illustrates the responses to different C. albicans strains using a skin sample. In Figure 1, there is no infection, and the skin sample is healthy. In Figure 2, the skin has been infected with a pathogenic strain of C. albicans. The skin equivalent is penetrated and tissue is destroyed. In Figure 3, non-pathogenic strains of C. albicans have infected the skin equivalent, but not change is observed. (Fraunhofer, 2002) Hence, the virulence factors that were mentioned in the previous slide must be significant in the success of infection of C. albicans. Figure 3. Infection with non-pathogenic C. albicans. This strain is not able to penetrate into the tissue and thus behaves as a virulent as shown in the mouse model of systemic infection. (Fraunhofer, 2002)
 Figure 1. skin equivalent before infection. Figure 2. Infection with pathogenic clinical isolate of C. albicans. After 48 h the yeast penetrates the skin equivalent and destroys. the tissue. This slide illustrates the responses to different C. albicans strains using a skin sample. In Figure 1, there is no infection, and the skin sample is healthy. In Figure 2, the skin has been infected with a pathogenic strain of C. albicans. The skin equivalent is penetrated and tissue is destroyed. In Figure 3, non-pathogenic strains of C. albicans have infected the skin equivalent, but not change is observed. (Fraunhofer, 2002) Hence, the virulence factors that were mentioned in the previous slide must be significant in the success of infection of C. albicans. Figure 3. Infection with non-pathogenic C. albicans. This strain is not able to penetrate into the tissue and thus behaves as a virulent as shown in the mouse model of systemic infection. (Fraunhofer, 2002)")
18
MORPHOGENESIS Figure 1. Morphogenesis. Morphogenesis in
C. albicans is a pivotal virulence factor that allows rapid multiplication and subsequent dissemination in host tissue. ( This slide shows the different routes of morphology that C. albicans may take according to the environment it is in. Figure 2. Morphogenic forms of Candida albicans

19
How Does It Cause Disease ?
•Candida albicans can disturb the immune system at different levels. •It is a polyantigenic organism, containing at least 30 different antigens. •It cross-reacts with baker’s yeast and brewer’s yeast. •It can induce production of autoantibodies and endocrinopathy. •It produces IgA proteases. •It contains glycoproteins which stimulate the mast cells to release histamine and prostaglandin.

20
How Does It Cause Disease ?
•It assimilates all sugars except lactose. •It depresses the activity of lactase. •Dietary carbohydrates are fungal growth promoters and associated with increased adherence of Candida species to mucosal epithelial cells. •Release of toxic fungal metabolites.

21
Candida albicans -Antibodies

22
Candida –Risk Factors of Infection
Examples Factor Pregnancy, age (elderly & infants) Diet high in sweets, fruit juices, alcohol Physiological Infection, burn wounds. Trauma Neutropenia, cellular immunodeficiency (leukaemia, lymphoma, AIDS, aplastic anaemia Haematological Diabetes mellitus, Addison’s disease, hypoparathyroidism Endocrinological Chemotherapeutics, corticosteroids, oral contraceptives, antibiotics catheters, surgery Iatrogenic Intravenous drugs, malnutrition, malabsorption, Chronic Stress Others
 Diet high in sweets, fruit juices, alcohol. Physiological. Infection, burn wounds. Trauma. Neutropenia, cellular immunodeficiency (leukaemia, lymphoma, AIDS, aplastic anaemia. Haematological. Diabetes mellitus, Addison’s disease, hypoparathyroidism. Endocrinological. Chemotherapeutics, corticosteroids, oral contraceptives, antibiotics catheters, surgery. Iatrogenic. Intravenous drugs, malnutrition, malabsorption, Chronic Stress. Others.")
23
Diseases by C. albicans Thrush :it is a white yeast infection of mouth &tongue most common in infant. Esophagitis Cutaneous Candidiasis Genital Yeast Infections Deep Candidiasis The common diseases that C. albicans can cause are oropharyngeal candidiasis, which includes thrush and esophagitis, cutaneous candidiasis, genital yeast infections, and deep candidiasis. As an overview, thrush and esophagitis are infections concering the mouth and throat. Patients infected with HIV or who have cancer have these types being the most frequent manifestations of mucotaneous lesions (Ruhnke, 2002). Cutaneous candidiasis is infection of the skin, scalp, and nails by C. albicans. An example is diaper rash that often occurs in newborn infants. Genital yeast infections, especially those women, are extremely frequent, but can affect men, too. Several lifestyle factors can predispose a man or woman to a genital yeast infection. Deep candidiasis is also known as invasive candidiasis and afflicts mainly people who are severely immunocompromised. Colonies of C. albicans invade the bloodstream and can spread to many areas of the body destroying tissue and leading to organ failure. It is one type of sepsis that carries a significant mortality and morbidity rate particularly in intensive care units where nosocomial infections are rampant (Marr, 2004). Recall that C. albicans is the fourth leading cause of nosocomial infections in the United States (Marr, 2004).
. Cutaneous candidiasis is infection of the skin, scalp, and nails by C. albicans. An example is diaper rash that often occurs in newborn infants. Genital yeast infections, especially those women, are extremely frequent, but can affect men, too. Several lifestyle factors can predispose a man or woman to a genital yeast infection. Deep candidiasis is also known as invasive candidiasis and afflicts mainly people who are severely immunocompromised. Colonies of C. albicans invade the bloodstream and can spread to many areas of the body destroying tissue and leading to organ failure. It is one type of sepsis that carries a significant mortality and morbidity rate particularly in intensive care units where nosocomial infections are rampant (Marr, 2004). Recall that C. albicans is the fourth leading cause of nosocomial infections in the United States (Marr, 2004).")
24
Thrush is commonly seen in infants
Thrush is commonly seen in infants. It is not considered abnormal in infants unless it lasts longer than a couple of weeks. Candida can also cause yeast infections in the vagina. People who have diabetes and had high blood sugar levels are more likely to get thrush in the mouth (oral thrush), because the extra sugar in your saliva acts like food for Candida. Taking high doses of antibiotics or taking antibiotics for a long time also increases the risk of oral thrush. Antibiotics kill some of the healthy bacteria that help keep Candida from growing too much. People with poorly fitting dentures are also more likely to get thrush.
, because the extra sugar in your saliva acts like food for Candida. Taking high doses of antibiotics or taking antibiotics for a long time also increases the risk of oral thrush. Antibiotics kill some of the healthy bacteria that help keep Candida from growing too much. People with poorly fitting dentures are also more likely to get thrush.")
25
Oral thrush Note multiple white plaques on lips, gingivae, tongue, and palate

26
Oral candidiasis (thrush)
…common in immunocompromised hosts, such as those with HIV infection.

27
Candidiasis Candida in culture Pseudohyphae and budding cells
in specimens

28
Oropharyngeal Thrush * Pseudo membranous * Atrophic * Angular chelitis
Risk Factors HIV Figure 1. Angular chelitis ( In 400 B.C., Hippocrates described oral thrush as oral ulcers. It was not until 1839 when Langenbeck detected fungi in the oral cavity. Then in 1846, Berg connected that the fungi caused oral thrush. To demonstrate, he infected healthy infants with samples he had taken from the oral lesions and saw the manifestation of thrush (Ruhnke, 2002). Although that would be considered an unethical approach to studying science in today’s society, it was a common practice to understand pathogenecity that lasted until the middle of the 20th century (Ruhnke, 2002). Thrush is the common name for an oral infection that is caused by Candida albicans. The areas of the mouth that are affected are the moist surfaces around the lips, inside the cheeks, and on the tongue and palate. Thrush in patients with cancer and AIDS is frequently observed. Other patients who are at-risk for developing thrush are elderly people, people who have diabetes, or those who have irritation from wearing dentures. There are three types of oral thrush that are clinically classified: pseudomembranous, atrophic, and angular chelitis (Samaranayake et. al., 1990). White, thick plaques that spot the sites of the buccal, mucosa, tongue, palata, and uvula characterize pseudomembraneous candidiasis. When these plaques are removed, they leave an erythematous bleeding surface. Symptoms include burning, pain, and changes in taste. In atrophic candidiasis, there is diffuse erythema that affects mainly the palate and the tongue and result in soreness. Oftentimes, this is denture-induced. Finally, in angular chelitis, the corners of the mouth show signs of cracking and inflammation and associated with the feeling of pain, burning, and soreness (Samarnayake et. al., 1990). When Candida infections spread to the esophagus, a condition known as esophagitis occurs. Symptoms related to this disease may be dysphagia, odynophagia, chest pain, and possible fever (Mildvan, 1995). Candidal esophagitis is the most frequent candidal disease in patients with HIV-AIDS and with oral candidiasis, contributes to an incident rate as high as 50-90% (Ruhnke, 2002). In many clinical cases, esophagitis is a marker that the HIV-infected patient is becoming significantly immunocompromised and is developing AIDs (HSTAT, 2005). Treatment for most oropharyngeal candidiasis typically involves topical antifungal agents (nystatin and clotrimazole) for thrush (Intelihealth). For more severe cases including esophagitis, treatment would require the administration of ketoconazoles or fluconazoles, which can be taken orally (Intelihealth). Flucanzole has proven to be the most effective medication in patients with HIV/AIDS (Intelihealth). Figure 2. Oral Thrush, atrophic ( Figure 3. Oral Thrush, pseudomembranous (
. Although that would be considered an unethical approach to studying science in today’s society, it was a common practice to understand pathogenecity that lasted until the middle of the 20th century (Ruhnke, 2002). Thrush is the common name for an oral infection that is caused by Candida albicans. The areas of the mouth that are affected are the moist surfaces around the lips, inside the cheeks, and on the tongue and palate. Thrush in patients with cancer and AIDS is frequently observed. Other patients who are at-risk for developing thrush are elderly people, people who have diabetes, or those who have irritation from wearing dentures. There are three types of oral thrush that are clinically classified: pseudomembranous, atrophic, and angular chelitis (Samaranayake et. al., 1990). White, thick plaques that spot the sites of the buccal, mucosa, tongue, palata, and uvula characterize pseudomembraneous candidiasis. When these plaques are removed, they leave an erythematous bleeding surface. Symptoms include burning, pain, and changes in taste. In atrophic candidiasis, there is diffuse erythema that affects mainly the palate and the tongue and result in soreness. Oftentimes, this is denture-induced. Finally, in angular chelitis, the corners of the mouth show signs of cracking and inflammation and associated with the feeling of pain, burning, and soreness (Samarnayake et. al., 1990). When Candida infections spread to the esophagus, a condition known as esophagitis occurs. Symptoms related to this disease may be dysphagia, odynophagia, chest pain, and possible fever (Mildvan, 1995). Candidal esophagitis is the most frequent candidal disease in patients with HIV-AIDS and with oral candidiasis, contributes to an incident rate as high as 50-90% (Ruhnke, 2002). In many clinical cases, esophagitis is a marker that the HIV-infected patient is becoming significantly immunocompromised and is developing AIDs (HSTAT, 2005). Treatment for most oropharyngeal candidiasis typically involves topical antifungal agents (nystatin and clotrimazole) for thrush (Intelihealth). For more severe cases including esophagitis, treatment would require the administration of ketoconazoles or fluconazoles, which can be taken orally (Intelihealth). Flucanzole has proven to be the most effective medication in patients with HIV/AIDS (Intelihealth). Figure 2. Oral Thrush, atrophic. ( Figure 3. Oral Thrush, pseudomembranous. (")
29
Symptoms Thrush appears as whitish, velvety lesions in the mouth and on the tongue. Underneath the whitish material, there is red tissue that may bleed easily. The lesions can slowly increase in number and size.

30
Candida Esophagitis

31
Candidiasis, cutaneous - around the mouth
This child has a large rash caused by Candidiasis, affecting the skin around the mouth. There are also other lesions that aren't connected to the large lesion, called "satellite lesions".

32
Vulvovaginal Candidiasis

33
Secondary infection Secondary infection occurs during or after treatment of a primary infection because the normal bacterial flora is destroyed, allowing yeast to flourish.

34
Candidiasis •It is generally known that about 50% of the medical evaluations of out-patient polysymptomatic patients fail to elucidate a specific causative disease. •The symptom patterns often suggest the possibility of a systemic disease process involving multiple body systems. •The patient may complain of chronic fatigue, poor concentration, impaired memory, respiratory tract symptoms, GI distress, pains in muscles and joints, skin problems, recurrent infections, urogenital problems etc. •Usually diagnosis is ‘stress’, ‘psychosomatic symptoms’ or an assurance ‘there is nothing physically wrong’.

35
Candidiasis -Symptoms
•Nasal congestion •Nasal itching •Dry mouth or throat •Rash or blisters in mouth •Sore throat •Laryngitis, loss of voice •Cough or bronchitis •Pain or tightness in chest •Bad breath •Indigestion or heartburn •Abdominal pain •Constipation / diarrhoea •Mucus in stools •Rectal itching •Bloated, belching, gas •Food sensitivity/intolerance •Chronic rashes or itching •Numbness, burning

36
Candidiasis -Symptoms
•Foot, hair or body odour •Muscle aches •Muscle weakness/paralysis •Pain and/or swelling joints •Vaginal burning, discharge •Rash or blisters in mouth •Sore throat •Laryngitis, loss of voice •Cough or bronchitis •Pain or tightness in chest •Bad breath •Indigestion or heartburn •Abdominal pain •Constipation / diarrhoea •Mucus in stools •Rectal itching •Bloated, belching, gas

37
Candidiasis -Symptoms
•Food sensitivity/intolerance •Chronic rashes or itching •Numbness, burning •Foot, hair or body odour •Muscle aches •Muscle weakness/paralysis •Pain and/or swelling joints •Vaginal burning, discharge •Loss of sexual desire •Urinary frequency or urgency •Burning on urination •Cold hands or feet and / or chilliness

38
Deep Candidiasis According to a survey conducted by the CDC, 8 in every 100,000 persons have candidemia each year (CDC). In deep candidiasis, C. albicans infects the bloodstream and spreads throughout the circulatory system and causes severe infection. Newborns, especially those who have low birth weights, severely immunocompromised patients, or those who have severe medical problems are vulnerable to this type of an infections. The fungi may gain access to the bloodstream through catheters, tracheotomies, ventilation, and deep surgical wounds (Intelihealth). It is for this reason that many hospitals need to reevaluate their protocol in treating patients to prevent high rates of nosocomial infections. It is also possible to get infected by C. albicans through intravenous drug abuse, severe burns, and traumatic wounds (Intelihealth). The symptoms include fevers and chills that are not usually alleviated after antibiotic treatment and symptoms associated with different affected organ sites. Death due to organ failure is inevitable if the sepsis is not treated. The treatment for deep candidiasis usually calls for the intravenous administration of amphotericin B. Invasive candiadis is involved in four over-lapping forms that typically begins as an episode of candidemia and leads to various clinical subtypes. These subtypes are catheter-related, acute disseminated, chronic disseminated, and deep organ candidiasis. Catheter-related candidemia is noted as the most common form of candidiasis, which puts C. albicans as the 4th most commonly isolated nosocomial pathogen. Infections of this type are mainly local. A direct contamination of the catheter makes it potentially potent to the patient as the organism can gain entry into the bloodstream and spread to other places in the body. Figure 1. Four forms of invasive candidiasis (
. In deep candidiasis, C. albicans infects the bloodstream and spreads throughout the circulatory system and causes severe infection. Newborns, especially those who have low birth weights, severely immunocompromised patients, or those who have severe medical problems are vulnerable to this type of an infections. The fungi may gain access to the bloodstream through catheters, tracheotomies, ventilation, and deep surgical wounds (Intelihealth). It is for this reason that many hospitals need to reevaluate their protocol in treating patients to prevent high rates of nosocomial infections. It is also possible to get infected by C. albicans through intravenous drug abuse, severe burns, and traumatic wounds (Intelihealth). The symptoms include fevers and chills that are not usually alleviated after antibiotic treatment and symptoms associated with different affected organ sites. Death due to organ failure is inevitable if the sepsis is not treated. The treatment for deep candidiasis usually calls for the intravenous administration of amphotericin B. Invasive candiadis is involved in four over-lapping forms that typically begins as an episode of candidemia and leads to various clinical subtypes. These subtypes are catheter-related, acute disseminated, chronic disseminated, and deep organ candidiasis. Catheter-related candidemia is noted as the most common form of candidiasis, which puts C. albicans as the 4th most commonly isolated nosocomial pathogen. Infections of this type are mainly local. A direct contamination of the catheter makes it potentially potent to the patient as the organism can gain entry into the bloodstream and spread to other places in the body. Figure 1. Four forms of invasive candidiasis (")
39
Onchomycosis Nail infections are much more difficult to
cure and can last a lifetime without proper treatment

40
Candidemia hematogenous seeding Spread to the eye Can cause blindness

41
Laboratory diagnosis Diagnosis based on direct exam of
scrapings, culture on selective media Examine for fungal hyphae and characteristic asexual spores – macroconidia Culture – colonies also Characteristic

42
Diagnosis History, signs and symptoms Visualization of pseudohyphae (mycelia) and/or budding yeast (conidia) on KOH or saline wet prep Stained with special fungal stain like lacto phenol blue . Stained histology slides :-gomoris methylamine sliver stains (GMS). Culture :sabourauds glucose agar medium; brain heart infusion. Serology by CFT &Latex agglutination test & ELISA. Skin test PCR& Fluorescent Abs Technique .
. Culture :sabourauds glucose agar medium; brain heart infusion. Serology by CFT &Latex agglutination test & ELISA. Skin test. PCR& Fluorescent Abs Technique .")
44
Candida Cross-Reactivity byImmunofluorescence

45
Vulvovaginal Candidiasis
- Vulvar component often dominant Diagnosis = symptoms with pseudohyphae On KOH prep - Women are often misdiagnosed as having VVC when they really have - Genital herpes - Contact dermatitis - Lichen planus - Atrophic vaginitis - Recurrent BV - Uncomplicated VVC defined by all 4: - Sporadic - Mild-moderate severity - Likely to be Candida albicans - Non-immunocompromised host

46
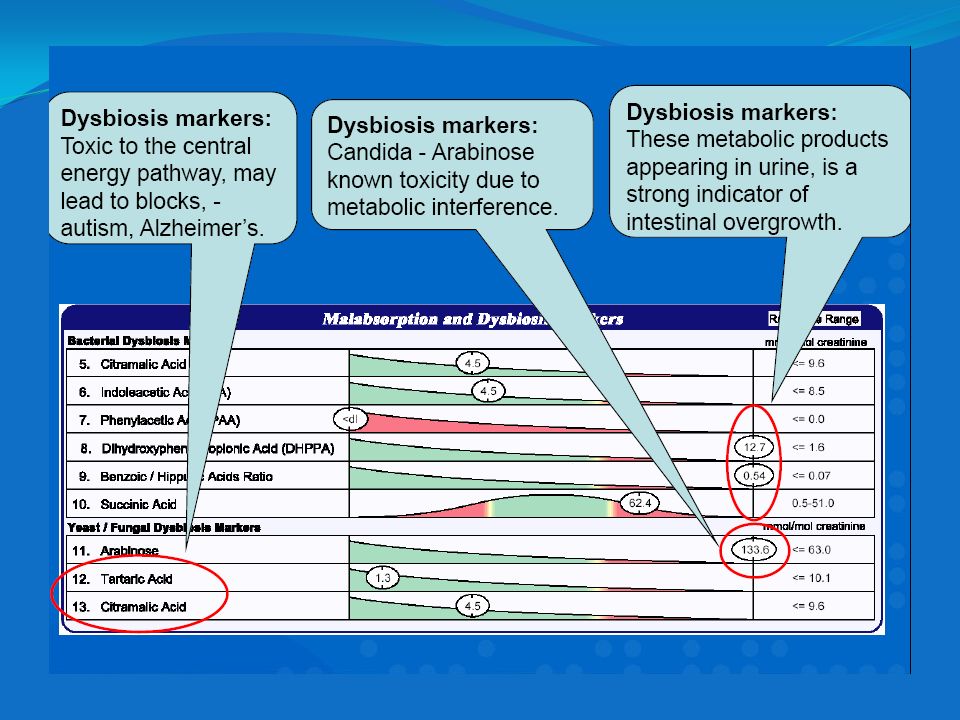
Dysbiosis Markers –Urine
•Compounds produced by bacteria, yeast, fungi, & protozoa that may colonise or grow in the small or large intestines. •Dysbiosis involves overgrowth of one or more species leading to increased production of these compounds, that are absorbed & excreted in urine. •When pathogens are distributed throughout the small & large intestine, stool testing is possible. However, it does not reveal the situation in the small intestine.

47
Dysbiosis Markers –Yeast / Fungal
•Their metabolic products appearing in urine, is a strong indicator of intestinal overgrowth. •Treatment with antifungals lowers these compounds. •Arabinitol –known toxicity due to metabolic interference. •ß-Ketoglutarate –toxic metabolic interference. •All are related central energy pathway, may lead to blocks, -autism, Alzheimer’s.

49
Dietary Treatment of Candida albicans
•Eliminate all sugar: –fruit juice –white flour –refined grains •Eat a higher protein, lower carbohydrate, high fiber diet •Avoid fermented foods including alcohol

50
Botanical Medicines with Anti-Fungal Activity
•Allium (garlic) •Astragalus •Barberry, Oregon Grape •Citrus Seed Extract •GrapeFruit Seed Extract •Hydrastis(Golden Seal) •Olive Leaf •Tebebuia(Pau d’Arco) •Plant Tannins Volatile Oils (enteric-coated) •Anise •Oregano •Rosemary •Sage •Thyme
 •Astragalus. •Barberry, Oregon Grape. •Citrus Seed Extract. •GrapeFruit Seed Extract. •Hydrastis(Golden Seal) •Olive Leaf. •Tebebuia(Pau d’Arco) •Plant Tannins. Volatile Oils (enteric-coated) •Anise. •Oregano. •Rosemary. •Sage. •Thyme.")
51
Current Drug Therapies
antifungal drugs: Amphotericin B (Fungizone) Clotrimazole (Mycelex) Fluconazole (Diflucan) Itraconazole (Sporanox) Ketoconazole (Nizoral) Nystatin (Mycostatin) The rise of incidences of candidal infections is not the only problem. Antifungal treatments against Candida are strained in the success due to the emergence of refractory fungal species and the development of drug resistance (Sanglard and Balk, 2002). Because the ergosterol biosynthesis pathway is quite specific to fungi, most antifungal drugs target it. These agents include polyenes and the azoles. Polyenes were discovered in the early 1950s and include one of its most successful derivatives in treating C. albicans, amphotericin B (AmB). AmB binds to ergosterol of the plasma membrane and causes the leakage of the cell’s electrolytes by puncturing it. AmB forms salts in acidic and basic environments and is insoluble in water. Its intense potency, however, is associated with severe side effects such as systemic and renal problems. To reduce these problems, AmB has been suspended with lipid complexes to lower its toxicity in mammalian cells (Sanglard and Balk, 2002). A decrease of ergosterol in the cell, however, gives resistance to this agent, which is another drawback. Resistant yeast strains may develop with lowered levels of ergosterol, which would render AmB useless as an antifungal drug. AmB is also known to cause oxidative damage to the cell, but resistant strains may develop with decreased catalase activity, which would diminish AmB’s ability as a powerful antifungal weapon. AmB is usually administered to patients with invasive candidiasis, although its treatment is also necessary for patients with oropharyngeal candidiasis who have had no success under azole therapy (Sanglard and Balk, 2002). The other major category of antifungal agents is the azoles. The group of azoles was discovered in the 1960s and contains the largest group of antifungal agents. Their mode of action is to inhibit the 14-lanosterol demethylase. It binds to the heme iron of the cytochrome P450 in yeast, which inhibits the enzymatic reaction that is involved in demethylating lanosterol into ergosterol (Sanglard and Balk, 2002). Ergosterol, which is needed for the production of Vitamin D in yeast cells, is not synthesized. Thus Vitamin D is not produced either, and the vitality of the yeast cell is supposedly lost. The azole antifungal agents have a broad-spectrum of activity. Perhaps because it is widely used, resistance to these agents is most frequently reported (Sanglard and Balk, 2002). Clinical studies have shown that resistance is related to the cells’ enhanced effluxes that are mediated by multidrug transporters that were upregulated (Sanglard and Balk, 2002). This upregulation explains for the failure resistant yeasts to accumulate the azoles.
 Clotrimazole (Mycelex) Fluconazole (Diflucan) Itraconazole (Sporanox) Ketoconazole (Nizoral) Nystatin (Mycostatin) The rise of incidences of candidal infections is not the only problem. Antifungal treatments against Candida are strained in the success due to the emergence of refractory fungal species and the development of drug resistance (Sanglard and Balk, 2002). Because the ergosterol biosynthesis pathway is quite specific to fungi, most antifungal drugs target it. These agents include polyenes and the azoles. Polyenes were discovered in the early 1950s and include one of its most successful derivatives in treating C. albicans, amphotericin B (AmB). AmB binds to ergosterol of the plasma membrane and causes the leakage of the cell’s electrolytes by puncturing it. AmB forms salts in acidic and basic environments and is insoluble in water. Its intense potency, however, is associated with severe side effects such as systemic and renal problems. To reduce these problems, AmB has been suspended with lipid complexes to lower its toxicity in mammalian cells (Sanglard and Balk, 2002). A decrease of ergosterol in the cell, however, gives resistance to this agent, which is another drawback. Resistant yeast strains may develop with lowered levels of ergosterol, which would render AmB useless as an antifungal drug. AmB is also known to cause oxidative damage to the cell, but resistant strains may develop with decreased catalase activity, which would diminish AmB’s ability as a powerful antifungal weapon. AmB is usually administered to patients with invasive candidiasis, although its treatment is also necessary for patients with oropharyngeal candidiasis who have had no success under azole therapy (Sanglard and Balk, 2002). The other major category of antifungal agents is the azoles. The group of azoles was discovered in the 1960s and contains the largest group of antifungal agents. Their mode of action is to inhibit the 14-lanosterol demethylase. It binds to the heme iron of the cytochrome P450 in yeast, which inhibits the enzymatic reaction that is involved in demethylating lanosterol into ergosterol (Sanglard and Balk, 2002). Ergosterol, which is needed for the production of Vitamin D in yeast cells, is not synthesized. Thus Vitamin D is not produced either, and the vitality of the yeast cell is supposedly lost. The azole antifungal agents have a broad-spectrum of activity. Perhaps because it is widely used, resistance to these agents is most frequently reported (Sanglard and Balk, 2002). Clinical studies have shown that resistance is related to the cells’ enhanced effluxes that are mediated by multidrug transporters that were upregulated (Sanglard and Balk, 2002). This upregulation explains for the failure resistant yeasts to accumulate the azoles.")
52
References Baillie, GS and LJ Douglas Role of dimorphism in the development of Candida albicans biofilme. J. Med. Microbiol. 48: Brown, JP Morphogenetic Signaling Pathways in Candida albicans. Washington: ASM Press: Candida and Candidiasis. pp Calderone, R.A. (ed.). Candida and Candidiasis. Washington: ASM Press; 2002. Calderone R and N.A.R. Gow Host recognition by Candida species. Washington: ASM Press: Candida and Candidiasis. pp Cormack, B.P., N. Ghori, and s. Falkow An adhesin of the yeast pathogen Candidia glabrata mediating adherence to human epithelial cells. Science 285: Ghannoum, MA Potential role of phospholipaes in virulence and fungal pathogenesis. Clin Micro Review. 13(1): Gow, NAR Cell Biology and the Cell Cycle of Candida. ASM Press: Candida and Candidiasis. pp Hawser, SP and LJ Douglas Biofilm formation by Candida species on the surface of catheter materials in vitro. Infect. Immuno. 62: Jabra-Rizk, MA. Et. al Fungal Biofilms and Drug Resistance. Emerging Infectious Diseases. 10(1): Jarvis, WR Epidemiology of nosocomial fungal infections, with emphasis on Candida species. Clin Infec Dis. 20(6):
. Candida and Candidiasis. Washington: ASM Press; Calderone R and N.A.R. Gow Host recognition by Candida species. Washington: ASM Press: Candida and Candidiasis. pp Cormack, B.P., N. Ghori, and s. Falkow An adhesin of the yeast pathogen Candidia glabrata mediating adherence to human epithelial cells. Science 285: Ghannoum, MA Potential role of phospholipaes in virulence and fungal pathogenesis. Clin Micro Review. 13(1): Gow, NAR Cell Biology and the Cell Cycle of Candida. ASM Press: Candida and Candidiasis. pp Hawser, SP and LJ Douglas Biofilm formation by Candida species on the surface of catheter materials in vitro. Infect. Immuno. 62: Jabra-Rizk, MA. Et. al Fungal Biofilms and Drug Resistance. Emerging Infectious Diseases. 10(1): Jarvis, WR Epidemiology of nosocomial fungal infections, with emphasis on Candida species. Clin Infec Dis. 20(6):")
53
15. U.S. National Library of Medicine 8600 Rockville Pike, Bethesda, MD U.S. Department of Health and Human Services National Institutes of Health Page last updated: 15 November 2010 16. Kauffman CA. Candidiasis. In: Goldman L, Ausiello D, eds. Cecil Medicine. 23rd ed. Philadelphia, Pa: Saunders Elsevier; 2007:chap 359. 17. WARREN LEVINSON;BOARD REVIEW OF MED. MICRO.&IMMUN;2008. 18. JAWETZ;MELNICK.MED.MICRO;2004. 19. CRUICK SHANK; BACTERIOLOGY ILLUSTRATED;1976. 20. URL of this page: Thrush is a yeast infection of the mucus membrane lining of the mouth and tongue

Similar presentations


>")










 –Five kingdoms –Modified by Woese’s.>")

>")
 Lecture 18 Bacterial Pathogenesis (Based on other textbooks such as Madigan’s)>")

>")
