Download presentation
Presentation is loading. Please wait.

1
Neonatal Resuscitation
The aim of obstetric emergency training is two-fold: Firstly it aims to provide the theoretical knowledge required for the effective treatment of maternal emergencies. In addition, it aims to teach the practical skills employed in these emergency situations and, specifically, maternal collapse.

2
Check equipment Always check equipment, ensure it is in working order
Become familiar with all equipment and ensure you know how it works Always be prepared for a flat infant Heater, light, clock Warm towels Air, O2, neopuff with masks in different size/Bag and mask Suction, with different sized suction catheters Laryngoscope

3
Basic equipment required
Radiant heater Apgar clock Air & oxygen and ability to blend same SaO2 & HR monitor Neopuff, tubing and 00 & 0/1 masks, bag & mask for back up if gas fails Suction tubing & catheters 8 (prems), 10 (all), 12 (meconium) Intubation equipment (laryngoscope handle, blades 0 & 1, stylet, ETT tubes 2.5, 3.0, 3.5 & 4.0’s, tapes)
, 10 (all), 12 (meconium) Intubation equipment (laryngoscope handle, blades 0 & 1, stylet, ETT tubes 2.5, 3.0, 3.5 & 4.0’s, tapes)")
4
Basic equipment required
PIV access equipment Umbilical access equipment (can use a size 5 feeding tube and a 3 way tap if nothing else available) Normal saline ampoules Adrenaline 1:10,000 ampoules 10 mL and 3 mL syringes and blunt needles This list covers the basics, for a full list refer to the neoresus website equipment guide.
 Normal saline ampoules. Adrenaline 1:10,000 ampoules. 10 mL and 3 mL syringes and blunt needles. This list covers the basics, for a full list refer to the neoresus website equipment guide.")
5
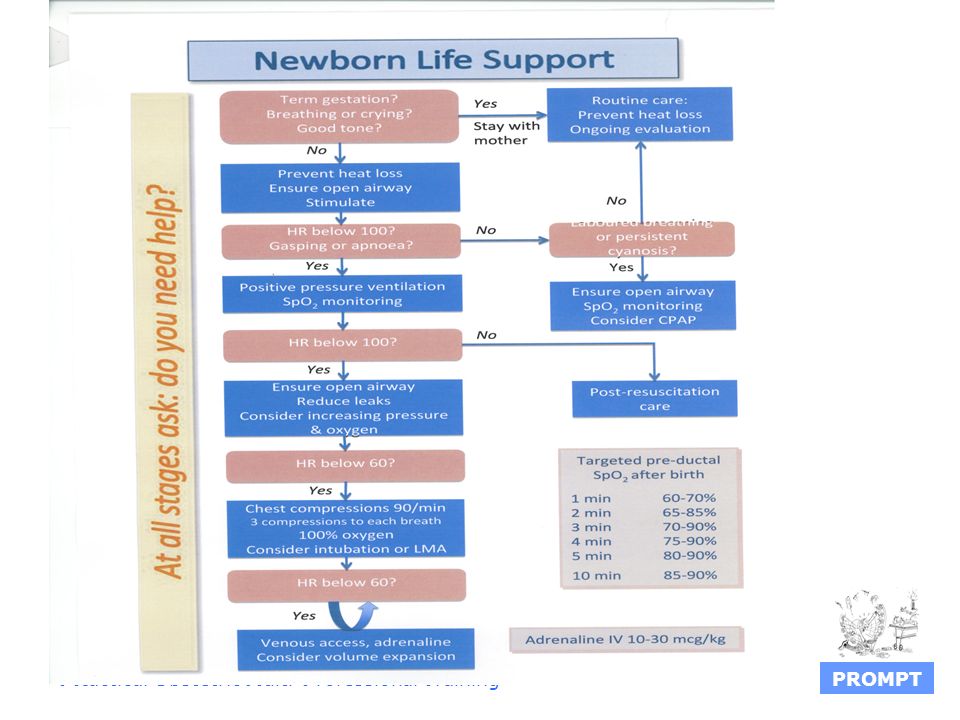
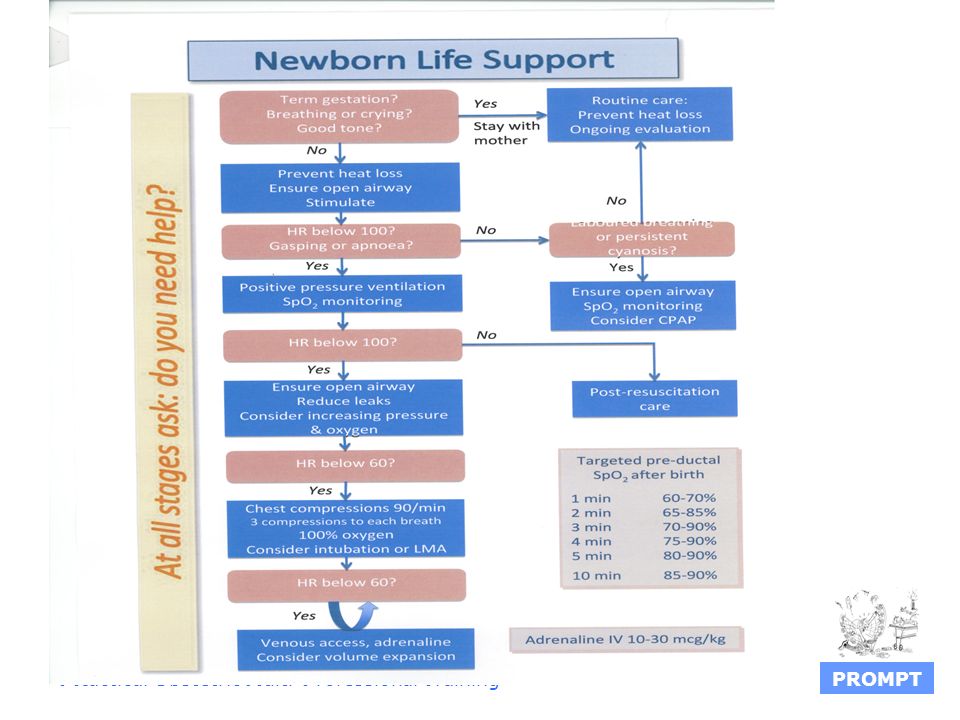
First evaluation Determines if intervention is required, is based upon the newly born infant’s: Response to stimulation Breathing Muscle tone Term? Amniotic fluid clear

6
First evaluation Is the baby making any respiratory effort?
What is their tone like? What is there colour like? Purple can be OK, white not OK. Newborns can take up to ten minutes to look “pink” Look at the colour of the lips to judge central cyanosis Blue hands/feet is not a concern PO2 in utero = Don’t waste initial precious time with a sats monitor

8
Assessment If baby is breathing, heart rate is > 100/min and beginning to look pink then give routine care and observations appropriate for gestation Ensure they are kept warm, close to mum if possible and continue to observe in the immediate time post birth If not…

9
Resuscitation needed…
Make it habit to start apgar clock when a baby is born, regardless of whether or not resus is required. If resuscitation is needed: Place the infant supine on the warm resuscitaire Head towards you, in a neutral position Remove wet wraps Provide warmth Think ABC 1 – 10 % of hospital born infants Dry, warm towels, hat

10
A B C A = Airway B = Breathing C = Circulation
The initial priority in neonatal resuscitation is to ventilate the lungs with air/oxygen

11
A = Airway Establish and maintain an airway
Position to maintain patency (so called ‘sniffing’ position) Suction only if required, the mouth first and then the nares. (Suction should not be extended past the oro /naso pharynx)
 Suction only if required, the mouth first and then the nares. (Suction should not be extended past the oro /naso pharynx)")
12
Suctioning If suctioning is done unneccessarily or too vigorously it:
Can cause gag reflex/vomiting, vagal depression and bradycardia Measure the suction tubing from the infant’s mouth to ear. The distance is similar to that from mouth to pharynx. In cases of meconium stained liquor there is special consideration regarding immediate care post birth 5 cm in term baby 100mmHg

13
Meconium Stained Liquor
If baby is not breathing and has poor muscle tone: Do not provide tactile stimulation Take baby to the resuscitaire If a medical officer is present they should suction the cords under direct vision using a large suction catheter (eg Fg 10-12), or an ETT with a mec aspirator Then proceed with standard resuscitation
, or an ETT with a mec aspirator. Then proceed with standard resuscitation.")
14
Meconium stained liquor
If a medical officer is not present The midwife should suction the mouth then nose and then proceed with standard resuscitation Ventilating the baby who is not breathing is still a priority Do not delay resuscitation to wait for a medical officer to be present

15
Breathing B = Breathing
Stimulate to breathe – firm, but gentle tactile stimulation (eg. Drying off the baby all over with a warm cloth) Assess respirations Provide IPPV (intermittent positive pressure ventilation) if the infant is not breathing &/or the heart rate is < 100 bmp
 Assess respirations. Provide IPPV (intermittent positive pressure ventilation) if the infant is not breathing &/or the heart rate is < 100 bmp.")
16
Ventilation Commence ventilation with medical air at flow 10litre/min
If oxygen is saturations are considered low for the time frame of transition, add O2 as required (eg could start at 40% and go up or down from there according to SaO2) Example of normal transition: at birth SaO2 of 60% normal, add 5% for each minute of life, getting to 85% by 5 mins of life If baby becomes bradycardic, requiring chest compressions commence 100% oxygen and wean if able once baby stabilised/not requiring chest compressions.
 Example of normal transition: at birth SaO2 of 60% normal, add 5% for each minute of life, getting to 85% by 5 mins of life. If baby becomes bradycardic, requiring chest compressions commence 100% oxygen and wean if able once baby stabilised/not requiring chest compressions.")
17
Ventilation Ventilate at a rate of 40 - 60 inflations per minute
Count: “breath- two- three, breath- two- three”, inflating the lungs as you say “breath” and allowing the infant to exhale on the “two - three” Babies have a very short inspiratory time (0.3 – 0.5 second) so don’t keep the inspiratory hole occluded for longer than a ‘fraction of a second’
 so don’t keep the inspiratory hole occluded for longer than a ‘fraction of a second’")
19
Hand/finger positioning on mask
Good technique with mask positioning is very important: apply the mask to the groove in the chin first, then roll up over the nose. Previous picture: with this type of mask it is preferable to have the thumb & first finger on top of the flat part of the mask, providing equal downward pressure (not as shown) – “2 point top hold” (see next slide)
 – 2 point top hold (see next slide)")
20
Different mask ‘hold’ techniques

21
Effective ventilation
The heart rate improves and increases to above 100 bpm The chest and upper abdomen rise with each inflation If these signs are not seen: reassess mask placement, reassess head position to open airway, consider increasing inflation pressures initially, consider suction if mouth is full of secretions. Tidal volume detemined by how long you push down on the Neopuff valve

22
“When performed properly, positive pressure ventilation alone is effective for resuscitating almost all apnoeic or bradycardic newborn infants” (ILCOR, 2006)
")
23
If response not satisfactory: Summon Help
Call for additional help Activate hospital protocol Notify switchboard (For Ballarat Hospital) Know your hospital protocol and codes to call For BHS state: neonatal code blue, location
 Know your hospital protocol and codes to call. For BHS state: neonatal code blue, location.")
24
Unsatisfactory response, consider:
Reposition mask, head position Higher inflation pressures (> 30 cmH2O and even as high as 50 cmH2O) may be needed for the first few inflations, especially in a pre-term infant who has never made any respiratory effort Once ventilation adequate REDUCE PRESSURES! Bag and mask pop off valve set at 40cm H2O
 may be needed for the first few inflations, especially in a pre-term infant who has never made any respiratory effort. Once ventilation adequate REDUCE PRESSURES! Bag and mask pop off valve set at 40cm H2O.")
25
Neopuff

26
Recommended Neopuff settings
Gas flow at 10 L/min Maximum pressure valve set at 50 cm H2O PIP at 30 cm H2O PEEP 5 cm H20 Ventilate breaths/min, 1/3 of the time in inspiration and 2/3 in expiration

27
Laerdal bag and mask Does not require gas supply
Cannot use passively, even with O2 connected

28
Circulation C = Circulation Assess heart rate and color
Chest compressions are indicated whenever the heart rate remains below 60 bmp despite 30 seconds of EFFECTIVE positive pressure ventilation 3 compression to 1 breathe Rate 2 a second 120/min 1,2,3 and breathe

29
Cardiac compressions Place hands symmetrically around the neonates chest. Place one thumb on top of the other on the lower half of the sternum (just below the nipple line) Fingers encircle the chest and rest on the boney structure of the scapular Compress 1/3 chest wall Reassess every 30 seconds
 Fingers encircle the chest and rest on the boney structure of the scapular. Compress 1/3 chest wall. Reassess every 30 seconds.")
30
2 thumbs technique (preferred)
2 thumbs on lower part of sternum, fingers over the spine compress to 1/3 of chest diameter

31
2 finger technique Place two fingers onto the lower third of the sternum, using the pads of the second and middle finger to compress the chest

32
Compressions The person providing the chest compressions should verbalize (out loud): “One - two - three - and - breathe, one - two - three - and - breathe” and so on. If the resuscitation has got to this point there will be the need to consider intubation, intravenous access and administration of adrenaline and/or normal saline bolus/es
: One - two - three - and - breathe, one - two - three - and - breathe and so on. If the resuscitation has got to this point there will be the need to consider intubation, intravenous access and administration of adrenaline and/or normal saline bolus/es.")
34
the infant’s lungs with air/oxygen.
The most important and effective action in neonatal resuscitation is to ventilate the infant’s lungs with air/oxygen.

35
Air or O2? Air (21%) should be used initially
Consider additional oxygen if the infant’s condition does not improve within the first minutes of resuscitation or if the baby bradycardic Aim to reduce supplementary O2 as infant improves

36
Deflate stomach During ventilation gas enters both the trachea and esophagus. Gas forced into the stomach interfers with ventilation. Consider the insertion of an orogastric tube to deflate the stomach – providing it does not interfer with resuscitation, having an orogastric insitu can effect the seal of the mask on the face.

38
< 30 weeks

39
< 32 weeks There has been a change to the ARC guidelines in 2012 with regard to the resuscitation of newborns < 32 weeks COMMENCE RESUSCITATION USING 30% OXYGEN, NOT AIR Increase to 100% if indicated, and wean down to air if able. Change PIP to 25 cmH2O (all other pressures remain the same)
")
40
Resuscitation Drugs Adrenaline 1:10,000
Can be administered through PIVC, UVC ( mL/kg) or ETT(0.3 – 1mL/kg) Solution is given as a straight push, undiluted and can be repeated multiple times Normal saline 10-20mLs/kg through PIVC or UVC If no other access possible intraosseous can be used and any infusions suitable to be given IV can go via that route
 or ETT(0.3 – 1mL/kg) Solution is given as a straight push, undiluted and can be repeated multiple times. Normal saline 10-20mLs/kg through PIVC or UVC. If no other access possible intraosseous can be used and any infusions suitable to be given IV can go via that route.")
41
Intubation May be considered at several stages during a resuscitation
Rarely required Size? (quick rule, divide gestation of baby by 10, eg 35wks = 3.5mm ETT) Insertion length (if orally, 6cm + wt of baby, eg 3kg baby = tape at 9cm at the lips)
 Insertion length (if orally, 6cm + wt of baby, eg 3kg baby = tape at 9cm at the lips)")
42
Scenario 1 28 yr old Primipara, 38 wks gestation, well through pregnancy, spontaneous labour Delay in second stage Clear liquor Shoulder dystocia, difficult birth, prolonged time on the perineum Baby born, apnoeic, poor muscle tone

43
Scenario 2 30 year old, multipara, 3 previous NVB’s, poor antenatal attendance Presented to birth suite, transitional, aggressive, difficult to manage Precipitate normal birth Baby appears IUGR, bruised face, stunned, apnoeic

44
Scenario 3 Multipara, history of premature births, presents at 29 weeks gestation, ? In labour Considerations? (steroids, MgSO4 infusion, transfer to tertiary hospital) Preparation for birth Proceeds to NVB Apnoeic, poor tone
 Preparation for birth. Proceeds to NVB. Apnoeic, poor tone.")
45
Scenario 4 25 year old multipara, Elective repeat LUSCS at 39 weeks gestation Difficultly with spinal anaesthetic Proceeds to general anaesthetic Delay from administration of anaesthetic to birth of baby Baby not breathing, poor tone

46
Scenario 5 27 year old primipara, induction of labour at 41.2 wks
ARM, syntocinon infusion Meconium stained liquor Fetal distress in second stage Forceps delivery Apnoeic, very floppy

47
Post Resuscitation Care
If significant resuscitation required consider admission to SCN for ongoing observation If baby appears well and does not require admission to SCN aim for WARM, SWEET and PINK Skin to skin with mum, feed, monitor temperature observing breathing, consider blood sugar monitoring

48
48

49
That’s all folks Previous picture is a resuscitaire in PNG (all just keeping warm while their mums are having a sleep post labour) makes me smile, thought it might make you too. Good luck with your exams Cheers, Nicole me if you have any worries/questions:
 makes me smile, thought it might make you too. Good luck with your exams. Cheers, Nicole. me if you have any worries/questions:")
Similar presentations














 wish to thank Dr S Richmond for this talk and fully acknowledge the use of material copyright the northern Neonatal Network,>")






) p. 201- 206 By : Mohammad Abuadas RN, MSN.>")