Download presentation
Presentation is loading. Please wait.

1
Chapter 17 – Intrapartum Fetal Surveillance
C. Lutkenhaus, MSN, RNC-OB, C-EFM Updated 8/2015

2
Purposes of Fetal Surveillance
Identify fetal well-being Identify the fetus who may be having hypoxic stress Two approaches to intrapartum fetal monitoring Intermittent auscultation with palpation of uterine activity Continuous electronic fetal monitoring

3
Fetal Oxygenation Normal flow of oxygenated maternal blood into the placenta Normal exchange within the placenta Patent umbilical cord vessels Normal fetal circulation Oxygen caring function

4
Fetal Oxygenation Factors related to adequate fetal oxygenation
Normal maternal blood flow and volume Maternal O2 sat Adequate placental exchanges (blood, 02) Normal fetal circulatory and oxygen carrying functions
 Normal fetal circulatory and oxygen carrying functions.")
5
Mechanisms That Influence the Fetal Heart Rate
Stimulation of the sympathetic nervous system: Increases the fetal heart rate Strengthens the heart contraction Stimulation of the parasympathetic nervous system: Slows the heart rate

6
Pathologic Influences on Fetal Oxygenation
Maternal cardiopulmonary alterations Uterine activity Placental disruptions Interruptions in umbilical flow Fetal alterations

7
Risk Factors for Fetal Compromise
Antepartum Maternal history (prior stillbirth or C/S, poor nutrition, chronic diseases, acute infections, hematologic problems, drug/alcohol abuse, psychosocial stressors) Problems during pregnancy (IUGR, prolonged or multi-fetal gestation, preeclampsia, gestational diabetes, placental abnormalities, anemia, infection, trauma) Intrapartum Maternal problems (hypo- or hypertension, hypertonic contractions, abnormal labor, prolonged ROM, infection, fever) Fetal or placental problems (anemia, abnormal heart rate or pattern, meconium, abnormal presentation or position, prolapsed cord, placental abruption)
 Problems during pregnancy (IUGR, prolonged or multi-fetal gestation, preeclampsia, gestational diabetes, placental abnormalities, anemia, infection, trauma) Intrapartum. Maternal problems (hypo- or hypertension, hypertonic contractions, abnormal labor, prolonged ROM, infection, fever) Fetal or placental problems (anemia, abnormal heart rate or pattern, meconium, abnormal presentation or position, prolapsed cord, placental abruption)")
8
Intermittent Fetal Monitoring
Auscultation and palpation Advantages – mobility, water-based pain management, “natural” Limitations – monitoring occurs only during part of labor, absence of continuous record, interruptions are distracting, more staff-intensive casacolibri.org

9
Electronic Fetal Monitoring
Advantages Provides permanent record, graphic record for review Continuous fetal responses to contractions Coach uses strip to anticipate contractions Gives nursing time for teaching Limitations Reduced mobility Position changes may require transducer adjustments Belts may be uncomfortable “Technical” birth rather than “natural” one clinicomp.com veronica-wanderlust.blogspot.com

10
Electronic Fetal Monitoring Types
External FM- Ultra-sound transducer and uterine activity tocodynomometer Internal FM – must have ruptured membranes for scalp electrode and intra-uterine pressure catheters (IUPC) cerner.com 2002, CDC reported that it was used 85.4% of the time, impacting 3.2 million live births. brighamandwomens.org
 cerner.com. 2002, CDC reported that it was used 85.4% of the time, impacting 3.2 million live births. brighamandwomens.org.")
11
Electronic Fetal Monitor
External Monitor Applied to the Patient 1. Uterine Activity toco-transducer. This instrument contains a pressure-sensing area which detects changes in the abdominal contour to measure uterine activity. It monitors frequency and duration of contractions. The monitor takes this signal and prints it out on the lower grid of the paper. 2. Fetal Heart Rate ultrasound transducer. The ultrasound (doppler) transducer when placed on the abdomen responds to high frequency sound waves from the action of the fetal heart and indicates the fetal heart rate changes. The monitor takes this signal and prints it out on the upper grid of the paper strip.
 transducer when placed on the abdomen responds to high frequency sound waves from the action of the fetal heart and indicates the fetal heart rate changes. The monitor takes this signal and prints it out on the upper grid of the paper strip.")
12
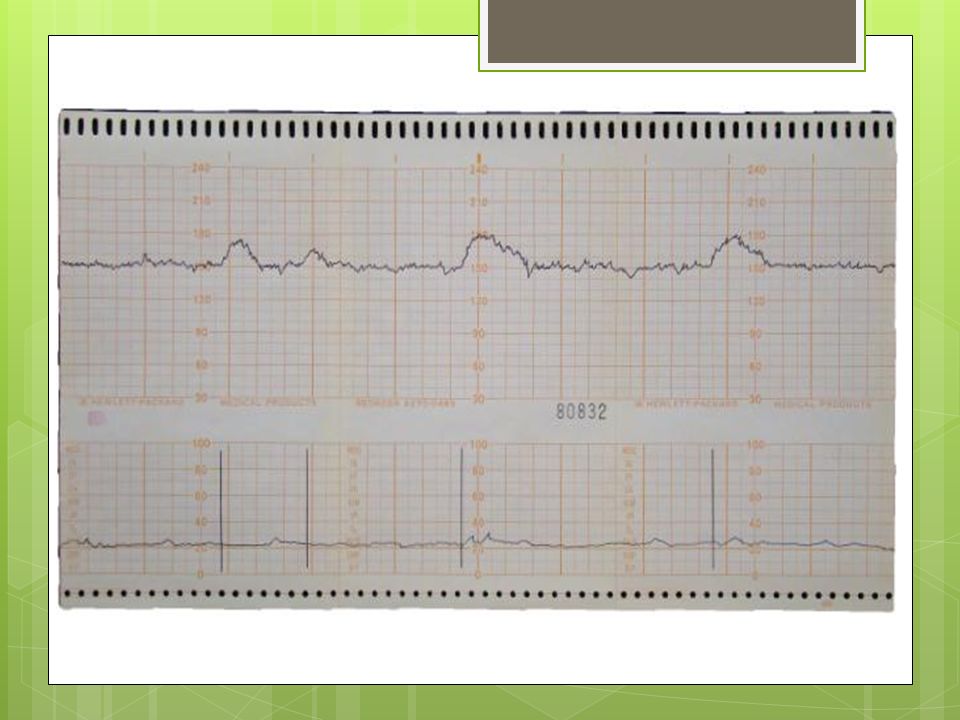
Fetal Heart Patterns Normal Pattern:
The baseline FHR is bpm in the full term fetus (preterm babies may have a higher FHR). The heart rate is noted on the upper portion of the monitoring graph strip. The lower portion of the monitoring graph strip is the recording of the uterine activity. Intensity of contractions is measured in mmHg by way of the internal uterine pressure catheter. The resting tone in between contractions is 10 mmHg. At the peak of a contraction the normal pressure is mm. Hg. You can assess frequency and duration of a contraction from this fetal monitor graph. Contractions last about seconds and frequency should be about every 2-3 minutes apart. The strip has dark lines and lighter lines. The dark lines are 1 minute apart and there are 10 seconds between the lighter lines.
. The heart rate is noted on the upper portion of the monitoring graph strip. The lower portion of the monitoring graph strip is the recording of the uterine activity. Intensity of contractions is measured in mmHg by way of the internal uterine pressure catheter. The resting tone in between contractions is 10 mmHg. At the peak of a contraction the normal pressure is mm. Hg. You can assess frequency and duration of a contraction from this fetal monitor graph. Contractions last about seconds and frequency should be about every 2-3 minutes apart. The strip has dark lines and lighter lines. The dark lines are 1 minute apart and there are 10 seconds between the lighter lines.")
14
Variability The normal irregularity of cardiac rhythm. The push-pull effect of cardiac accelerations and decelerations as influenced by ANS, CNS, etc. Variability on the FHR paper strip is demonstrated by fluctuations of the FHR baseline that cause the printed line to have a rough rather than smooth appearance. Decreased variability is an early warning sign of fetal distress. Absence of variability (smooth baseline ) is a sign of fetal distress, usually indicates fetal hypoxia, and acidosis and is normal for a fetus < 28 weeks.
 is a sign of fetal distress, usually indicates fetal hypoxia, and acidosis and is normal for a fetus < 28 weeks.")
15
Accelerations Accelerations Increase in HR of 15 beats for 15 seconds
The heart rate accelerates above the normal baseline. Accelerations are most often associated with fetal movement and uterine contractions. An acceleration of 15 bpm for 15 seconds is a healthy sign of fetal alertness and well-being (over 32 week fetus). Accelerations Increase in HR of 15 beats for 15 seconds 28-32 weeks 10x10 accels Reassuring sign no treatment required
. Accelerations. Increase in HR of 15 beats for 15 seconds weeks 10x10 accels. Reassuring sign no treatment required.")
16
Decelerations Decelerations are a drop in FHR below baseline. The timing and type of the deceleration in relation to the uterine contraction indicate certain factors. A. Early Decelerations: Early decelerations occur only during a contraction. They are mirror images of the contraction and begin early in the contraction with the onset of the contraction and recovery occurring at the same time the uterine contraction ends and returns to baseline. Early decelerations are caused by compression of the fetal head which causes reduced cerebral blood flow which stimulates the vagus nerve which produces a decrease in heart rate. No intervention is necessary. B. Variable Decelerations: Variable decelerations are those periodic decelerations that occur anytime during a uterine contraction. Variable decelerations are related to umbilical cord compression which results in a lack of oxygen in fetal blood. The pattern is probable variable because the degree of cord compression changes from one contraction to another. Variable decelerations indicate fetal distress when there is prolonged or deep decelerations of bpm. Interventions include position changes for the patient and amnioinfusion. C. Late Decelerations: Late decelerations are periodic decelerations that begin late in the contraction and recovery and return to baseline after the end of the contraction. These are related to uteroplacental insufficiency. When the flow of blood from the mother to the placenta is compromised, the fetal heart rate slows. Late decelerations are an ominous sign and usually are associated with fetal asphyxia and acidosis. Nursing interventions for fetal distress are necessary.

17
Fetal Tachycardia Fetal Tachycardia Greater than 160bpm x 10 min
Possible causes: terbutaline*, maternal anxiety or fever, prematurity, fetal infection, fetal stimulation, Early sign of fetal hypoxia Tx: Notify the doctor Not FDA Approved any longer.

18
Fetal Bradycardia Possible causes: Late sign of fetal hypoxia
Less than 110bpm > 10 min Possible causes: narcotics, epidural, pitocin, maternal hypotension, prolonged cord compression, postmaturity Late sign of fetal hypoxia Tx: Call the doctor WORD OF CAUTION: Make certain that a non-reassuring pattern is not attributable to medical intervention. Fetal bradycardia may result from maternal hypotension after an epidural or narcotic given IVP. In these cases, correcting the maternal condition may be all that is needed to correct the bradycardia.

19
Early Decelerations Early Decelerations
Decrease in HR near beginning of contraction and return to baseline by end “Mirror” the contraction Caused by head compression during contraction Not associated with fetal compromise No treatment required

20
Variable Decelerations
Caused by cord compression Can happen with ROM- artificial or spontaneous Are sharp shapes of “V” or “W” Usually treated by repositioning mother Appear differently from either early or late decelerations. They are characterized by a sudden, abrupt drop in the FHT and often an abrupt return to baseline.

21
Late Decelerations Caused by utero-placental insufficiency or compromise Fetus has reduced O2 reserves Occur after(thus late) the peak of contraction with return to baseline after end of contraction Usually treated with repositioning, IV fluid bolus. Stop pitocin, may give tocolytic, and O2. Requires careful monitoring and reporting
 the peak of contraction with return to baseline after end of contraction. Usually treated with repositioning, IV fluid bolus. Stop pitocin, may give tocolytic, and O2. Requires careful monitoring and reporting.")
22
Nursing Interventions for Fetal Distress
1. Reposition the woman, avoiding supine 2. Give oxygen via mask at lpm 3. Turn off the Pitocin, if there is any infusing 4. Give tocolytic if indicated 5. Increase the rate of the main line IV 6. Call the doctor

23
What do you think?

24
What do you think?

25
What do you think?

26
What do you think?

Similar presentations

: Part 1 - Introduction>")

















