Download presentation
Presentation is loading. Please wait.

1
1 CONTRAST - INDUCED ACUTE RENAL INJURY

2
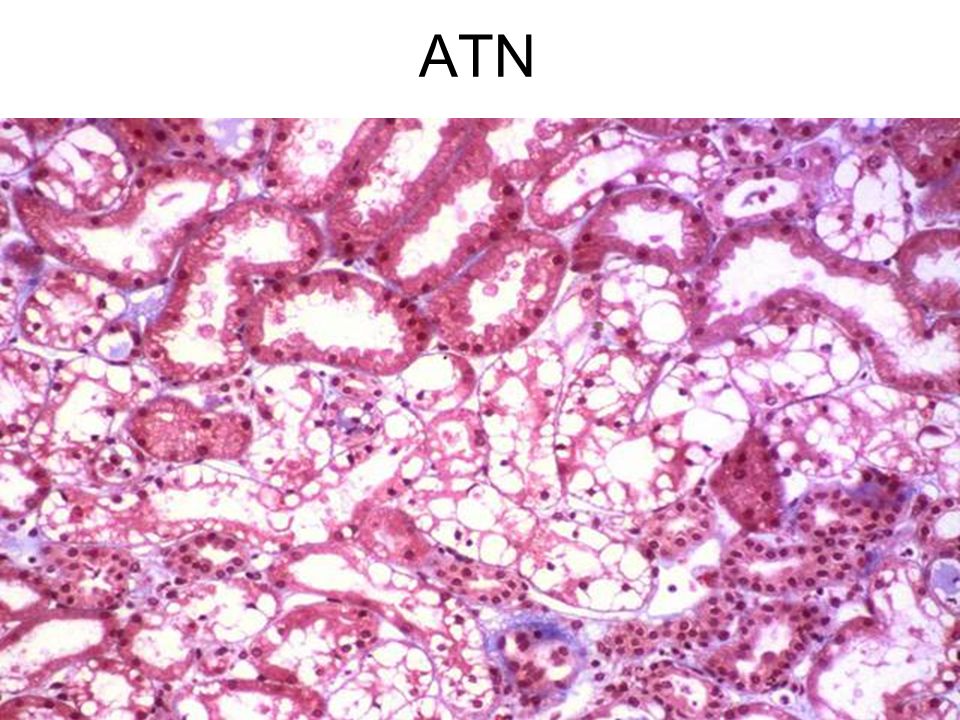
Acute Renal Failure Nephrotoxic ATN Endogenous Toxins –Heme pigments (myoglobin, hemoglobin) –Myeloma light chains Exogenous Toxins –Antibiotics (e.g., aminoglycosides, amphotericin B) –Radiocontrast agents –Heavy metals (e.g., cis-platinum, mercury) –Poisons (e.g., ethylene glycol)
 –Myeloma light chains Exogenous Toxins –Antibiotics (e.g., aminoglycosides, amphotericin B) –Radiocontrast agents –Heavy metals (e.g., cis-platinum, mercury) –Poisons (e.g., ethylene glycol)")
3
ATN

5
Contrast-Induced ARF Prevalence Less than 1% in patients with normal renal function Increases significantly with renal insufficiency

6
Contrast-Induced ARF Risk Factors Renal insufficiency Diabetes mellitus Multiple myeloma High osmolar (ionic) contrast media Contrast medium volume
 contrast media Contrast medium volume")
7
Contrast-induced ARF Clinical Characteristics Onset - 24 to 48 hrs after exposure Duration - 5 to 7 days Non-oliguric (majority) Dialysis - rarely needed Urinary sediment - variable Low fractional excretion of Na
 Dialysis - rarely needed Urinary sediment - variable Low fractional excretion of Na")
8
Pre-Procedure Prophylaxis 1. IV Fluid (N/S) 1-1.5 ml/kg/hour x12 hours prior to procedure and 6-12 hours after 2. Mucomyst (N-acetylcysteine) Free radical scavenger; prevents oxidative tissue damage 600mg po bd x 4 doses (2 before procedure, 2 after)
 ml/kg/hour x12 hours prior to procedure and 6-12 hours after 2. Mucomyst (N-acetylcysteine) Free radical scavenger; prevents oxidative tissue damage 600mg po bd x 4 doses (2 before procedure, 2 after).")
9
9 Pre-Procedure Prophylaxis 3. Bicarbonate (JAMA 2004) Alkalinizing urine should reduce renal medullary damage 5% dextrose with 3 amps HCO3; bolus 3.5 mL/kg 1 hour preprocedure, then 1mL/kg/hour for 6 hours postprocedure 4. Possibly helpful? Fenoldopam, Dopamine 5. Not helpful! Diuretics, Mannitol
 Alkalinizing urine should reduce renal medullary damage 5% dextrose with 3 amps HCO3; bolus 3.5 mL/kg 1 hour preprocedure, then 1mL/kg/hour for 6 hours postprocedure 4. Possibly helpful. Fenoldopam, Dopamine 5. Not helpful. Diuretics, Mannitol.")
10
Contrast-induced ARF Prophylactic Strategies Use I.V. contrast only when necessary Hydration Minimize contrast volume Low-osmolar (nonionic) contrast media N-acetylcysteine, fenoldopam
 contrast media N-acetylcysteine, fenoldopam.")
11
11 McCullough, P. A. J Am Coll Cardiol 2008;51:1419-1428 Risk of Contrast-Induced AKI According to Baseline Renal Function (eGFR or CrCl ml/min)
.")
12
12 McCullough, P. A. J Am Coll Cardiol 2008;51:1419-1428 Postulated Pathophysiology of Contrast-Induced AKI

13
13 McCullough, P. A. J Am Coll Cardiol 2008;51:1419-1428 Rates of Contrast-Induced AKI in a Meta-Analysis of 16 Trials of Iso-Osmolar Iodixanol

14
14 McCullough, P. A. J Am Coll Cardiol 2008;51:1419-1428 Advanced Algorithm for Management of Patients Receiving Iodinated Contrast Media

15
15 Protocol for interventional radiology. © 2009 Mayo Foundation for Medical Education and Research

16
16 Protocol for diagnostic computed tomography risk defined according to American College of Radiology (ACR) criteria.20 AKI = acute kidney injury; CKD = chronic kidney disease; CM = contrast medium; CrCl = creatinine clearance; eGFR = estimated glomerular filtration rate; MDRD = Modification of Diet in Renal Disease; NSAIDs = nonsteroidal anti-inflammatory drugs. Goldfarb S et al. Mayo Clin Proc. 2009;84:170-179

17
17 Protocol for interventional cardiology. Goldfarb S et al. Mayo Clin Proc. 2009;84:170-179

18
18 THE TRIALS

19
19 Brar, S. S. et al. Clin J Am Soc Nephrol 2009;4:1584-1592 Flowchart of meta-analysis

20
20 Brar, S. S. et al. Clin J Am Soc Nephrol 2009;4:1584-1592 Funnel plot with pseudo-95% confidence limits for assessment of publication bias

21
21 Brar, S. S. et al. Clin J Am Soc Nephrol 2009;4:1584-1592 Forest plot of randomized trials meeting inclusion criteria

22
22 Brar, S. S. et al. Clin J Am Soc Nephrol 2009;4:1584-1592 CI-AKI rates by trial

23
23 Brar, S. S. et al. Clin J Am Soc Nephrol 2009;4:1584-1592 CI-AKI in studies meeting quality criteria

24
24 Brar, S. S. et al. Clin J Am Soc Nephrol 2009;4:1584-1592 Changes in serum creatinine in published trials

25
25 Circulation 2009; 120: 1793– 1799 Iloprost, a prostacyclin analogue, has been shown to protect against radiocontrast media renal toxicity in rats Compared iloprost (infused 30 – 90 min before, ending 4 h after intervention) to placebo in a trial of 208 patients with serum creatinine ≥1.4 mg/dL undergoing coronary angiography and/or percutaneous coronary intervention (PCI).
 to placebo in a trial of 208 patients with serum creatinine ≥1.4 mg/dL undergoing coronary angiography and/or percutaneous coronary intervention (PCI).")
26
26 Circulation 2009; 120: 1793– 1799 These patients were at high risk for CI-AKI; 50% were diabetic, and contrast volumes were large (mean approximately 250 cc) Of patients randomized to iloprost, 8% developed CI-AKI versus 22% of control patients (odds ratio [OR] 0.29, confidence interval [all reported at 95%] 0.12 – 0.69)
![26 Circulation 2009; 120: 1793– 1799 These patients were at high risk for CI-AKI; 50% were diabetic, and contrast volumes were large (mean approximately 250 cc) Of patients randomized to iloprost, 8% developed CI-AKI versus 22% of control patients (odds ratio [OR] 0.29, confidence interval [all reported at 95%] 0.12 – 0.69)](http://images.slideplayer.com/38/10828263/slides/slide_26.jpg "26 Circulation 2009; 120: 1793– 1799 These patients were at high risk for CI-AKI; 50% were diabetic, and contrast volumes were large (mean approximately 250 cc) Of patients randomized to iloprost, 8% developed CI-AKI versus 22% of control patients (odds ratio [OR] 0.29, confidence interval [all reported at 95%] 0.12 – 0.69)")
27
27 J Am Coll Cardiol 2009; 53: 1040–1046 Testing the efficacy of atrial natriuretic peptide (ANP; initiated 4 – 6 h before, continued for 48 h after coronary angiography or intervention) in a randomized placebo-controlled trial of CI-AKI prevention in 254 patients Independent predictors of CI-AKI were contrast volume ≥155 cc (OR 6.89, 2.4 – 19.3) and ANP infusion (OR 0.24, 0.07 – 0.77).
 in a randomized placebo-controlled trial of CI-AKI prevention in 254 patients Independent predictors of CI-AKI were contrast volume ≥155 cc (OR 6.89, 2.4 – 19.3) and ANP infusion (OR 0.24, 0.07 – 0.77).")
28
28 J Am Coll Cardiol 2009; 53: 1040–1046 Protective effect of ANP is interesting Scrupulous attention to contrast volume and pre-procedural intravascular volume expansion remain the cornerstones of CI- AKI prevention

29
29 Am Heart J 2009; 158: 822–828 Comparative efficacy of iso-osmolar versus low-osmolar contrast media (LOCM) for CI-AKI prevention compared the 'iso-osmolar' iodixanol to the 'low-osmolar' iopamidol in 526 patients (of whom 418 were 'evaluable') with diabetes and CKD
 for CI-AKI prevention compared the iso-osmolar iodixanol to the low-osmolar iopamidol in 526 patients (of whom 418 were evaluable ) with diabetes and CKD")
30
30 Am Heart J 2009; 158: 822–828 Median baseline estimated creatinine clearance was 45.5 mL/min for the iodixanol and 47.9 mL/min for the iopamidol groups (P = ns) Peri-procedural intravascular volume expansion was employed, but without sodium bicarbonate or other putative 'nephroprotective' agents Contrast volume was similar in both groups and not unduly large (mean approximately 120 cc).
 Peri-procedural intravascular volume expansion was employed, but without sodium bicarbonate or other putative nephroprotective agents Contrast volume was similar in both groups and not unduly large (mean approximately 120 cc).")
31
31 Am Heart J 2009; 158: 822–828 Incidence of CI-AKI was 11.2% in the iodixanol and 9.8% in the iopamidol groups (P = ns) As the study population would be legitimately considered to be at increased risk for CI-AKI, the findings are noteworthy, with the caveat that creatinine clearance was < 30 mL/min for relatively few patients (10%).
 As the study population would be legitimately considered to be at increased risk for CI-AKI, the findings are noteworthy, with the caveat that creatinine clearance was < 30 mL/min for relatively few patients (10%).")
32
32 JACC Cardiovasc Interv 2009; 2: 415–421 Compared 72 patients (51% with diabetes) receiving iodixanol to 74 patients (41% with diabetes) receiving the low-osmolar agent ioxaglate Mean baseline creatinine clearance in both groups was about 45 mL/min
 receiving iodixanol to 74 patients (41% with diabetes) receiving the low-osmolar agent ioxaglate Mean baseline creatinine clearance in both groups was about 45 mL/min")
33
33 JACC Cardiovasc Interv 2009; 2: 415–421 The contrast volume was large (55% of iodixanol and 51% of ioxaglate patients received at least 200 cc) A peak increase in serum creatinine of ≥0.5 mg/dL occurred in 15.9% of iodixanol and 18.2% of ioxaglate patients (P = ns) An increase of at least 25% in 15.9% of iodixanol and 24.2% of ioxaglate patients (P = ns)
 A peak increase in serum creatinine of ≥0.5 mg/dL occurred in 15.9% of iodixanol and 18.2% of ioxaglate patients (P = ns) An increase of at least 25% in 15.9% of iodixanol and 24.2% of ioxaglate patients (P = ns)")
34
34 JACC Cardiovasc Interv 2009; 2: 645–654 A recent meta-analysis of 16 trials comparing CI-AKI incidence with iodixanol and other LOCM found no difference overall for iodixanol versus LOCM (relative risk [RR] 0.79, 0.56 – 1.12)
![34 JACC Cardiovasc Interv 2009; 2: 645–654 A recent meta-analysis of 16 trials comparing CI-AKI incidence with iodixanol and other LOCM found no difference overall for iodixanol versus LOCM (relative risk [RR] 0.79, 0.56 – 1.12)](http://images.slideplayer.com/38/10828263/slides/slide_34.jpg "34 JACC Cardiovasc Interv 2009; 2: 645–654 A recent meta-analysis of 16 trials comparing CI-AKI incidence with iodixanol and other LOCM found no difference overall for iodixanol versus LOCM (relative risk [RR] 0.79, 0.56 – 1.12)")
35
35 JACC Cardiovasc Interv 2009; 2: 645–654 However, when individual agents were compared, the conclusion was somewhat different: Iodixanol versus ioxaglate, RR 0.58, 0.37 – 0.92; versus iohexol, RR 0.19, 0.07 – 0.56; versus iopamidol, RR 1.20, 0.66 – 2.18; versus iopromide, RR 0.93, 0.47 – 1.83; versus ioversol, RR 0.92, 0.60 – 1.39

36
36 JACC Cardiovasc Interv 2009; 2: 645–654 Unfortunately, no compelling data could resolve this agent-specific versus class- specific conundrum for CI-AKI But this is not a unique clinical problem At present, a fair conclusion is that the benefit of iodixanol for reducing CI-AKI risk is, at best, modest

37
37 Role of sodium bicarbonate for preventing CI-AKI The issue remains unsettled A open-label trial randomized 502 patients with estimated creatinine clearance < 60 mL/min to isotonic saline 1 mL/kg/h 12 h before and after coronary angiography/PCI or sodium bicarbonate (154 mEq/L in dextrose and water) 3 mL/kg 1 h before contrast administration and 1 mL/kg/h 6 h after the procedure
 3 mL/kg 1 h before contrast administration and 1 mL/kg/h 6 h after the procedure")
38
38 J Am Coll Cardiol 2008; 52: 599–604 All patients received oral N-acetylcysteine and iodixanol Mean contrast volume was 170 mL in the saline and 160 mL in the bicarbonate groups Only 24% of patients were diabetic Mean basal creatinine clearance was 42 mL/min in the saline and 43 mL/min in the bicarbonate group (< 30 mL/min for only 15% of all patients)
")
39
39 J Am Coll Cardiol 2008; 52: 599–604 CI-AKI (≥0.5 mg/dL increase in serum creatinine within 5 days after contrast) occurred in 11.5% of the saline and 10.0% of the bicarbonate groups (P = 0.60) The secondary endpoint, ≥25% relative increase in serum creatinine, occurred for 20.6% of the saline and 15.2% of the bicarbonate groups (P = 0.13)
 occurred in 11.5% of the saline and 10.0% of the bicarbonate groups (P = 0.60) The secondary endpoint, ≥25% relative increase in serum creatinine, occurred for 20.6% of the saline and 15.2% of the bicarbonate groups (P = 0.13)")
40
40 J Am Coll Cardiol 2008; 52: 599–604 This trial is 'negative', but one paradoxical outcome may be increased sodium bicarbonate use; a 7-h infusion of sodium bicarbonate would be more palatable than a 24-h infusion of saline.

41
41 Am J Cardiol 2009; 104: 921– 925 A single-bolus intravenous administration of 20 mEq of sodium bicarbonate 5 min before contrast exposure further reduces CI-AKI risk when added to 'conventional' isotonic saline administration, given 12 h before and after contrast However, infusion time was not shortened in the bicarbonate arm

42
42 Am J Cardiol 2009; 104: 921– 925 In this small trial (72 patients in each arm), incidence of reported CI-AKI (>25% rise in serum creatinine or >0.5 mg/dL within 3 days) was 1.4% in the saline/bicarbonate arm versus 12.5% in the saline-only arm (P = 0.017) More trials on the role of sodium bicarbonate in preventing CI-AKI are likely
, incidence of reported CI-AKI (>25% rise in serum creatinine or >0.5 mg/dL within 3 days) was 1.4% in the saline/bicarbonate arm versus 12.5% in the saline-only arm (P = 0.017) More trials on the role of sodium bicarbonate in preventing CI-AKI are likely")
Similar presentations
 Sepehr Khashaei, MD Assistant professor Department of Internal Medicine.>")
:>")



: RenalGuard™ System In High-Risk Patients for Contrast-Induced.>")













 Trial: The ACT Trial Investigators Presenter: Otavio Berwanger (MD; PhD) Chair.>")