Download presentation
Presentation is loading. Please wait.

1
Aging Q3 ACOVE #10 Pain Management in the Elderly Rog Kyle, MD Medical University of South Carolina 10/7/11 rev. 9/20/13

2
Background Chronic pain (cancer and non-cancer) problematic in 25-50% of elders in the community Osteoarthritis (and other musculoskeletal) is most common cause Low back pain (LBP) most prevalent condition
 problematic in 25-50% of elders in the community Osteoarthritis (and other musculoskeletal) is most common cause Low back pain (LBP) most prevalent condition")
3
Cancer pain – 80% of elderly with cancer report pain – Probably under detected and under treated – Deficiencies Under documented Under treated – opioids and non-opioids

4
Reporting by patients – Most feared complication of illness – Pain is the second leading complaint in physicians’ offices – Effects on mood, functional status, and quality of life – Associated with increased health resources use

5
Hospitalized patients – No randomized trials – Prospective studies on cancer patients Underestimate pain Probably do not assess frequently enough

6
Challenges in the elderly Comparatively little data Cognitive impairment and compliance Underreported by patients Drug-drug interaction and polypharmacy a serious concern Reduced hepatic function, reduced renal function

7
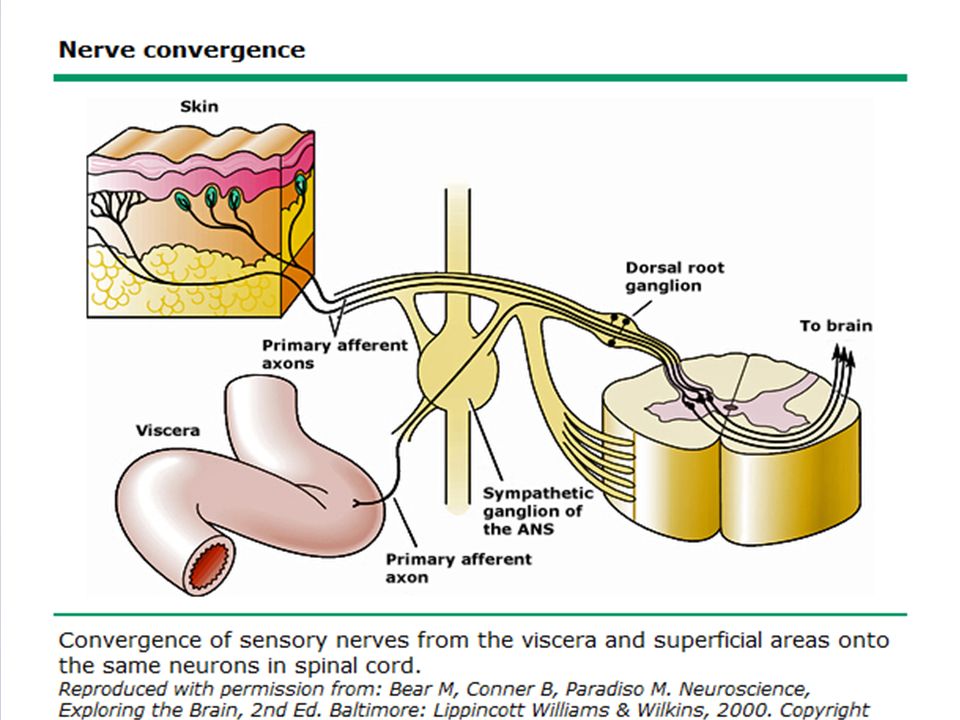
Mechanisms for pain Nociceptive – Nociceptors = pain fiber sensitive to noxious stimuli Somatic – injury to tissues, well localized Visceral – injury to organs (stretch receptors), poorly localized
, poorly localized")
8
Neuropathic – Abnormal neural activity secondary to disease, injury, or dysfunction (allodynia). – Persists without ongoing injury (trigeminal neuralgia, DM neuropathy) – Types: Sympathetic – from peripheral nerve injury with autonomic changes – “New” term – Complex Regional Pain Syndrome (CRPS) Type I = RSD Type II = causalgia Peripheral autonomic pain – – Same but without autonomic change (PHN) Central Pain (spinal cord injury)
 – Types: Sympathetic – from peripheral nerve injury with autonomic changes – New term – Complex Regional Pain Syndrome (CRPS) Type I = RSD Type II = causalgia Peripheral autonomic pain – – Same but without autonomic change (PHN) Central Pain (spinal cord injury).")
9
Pain pathways Nociceptive fibers – afferent fibers to dorsal horn – Two types A-delta – sharp pain (fast) C polymodal – dull pain (slow)
 C polymodal – dull pain (slow)")
11
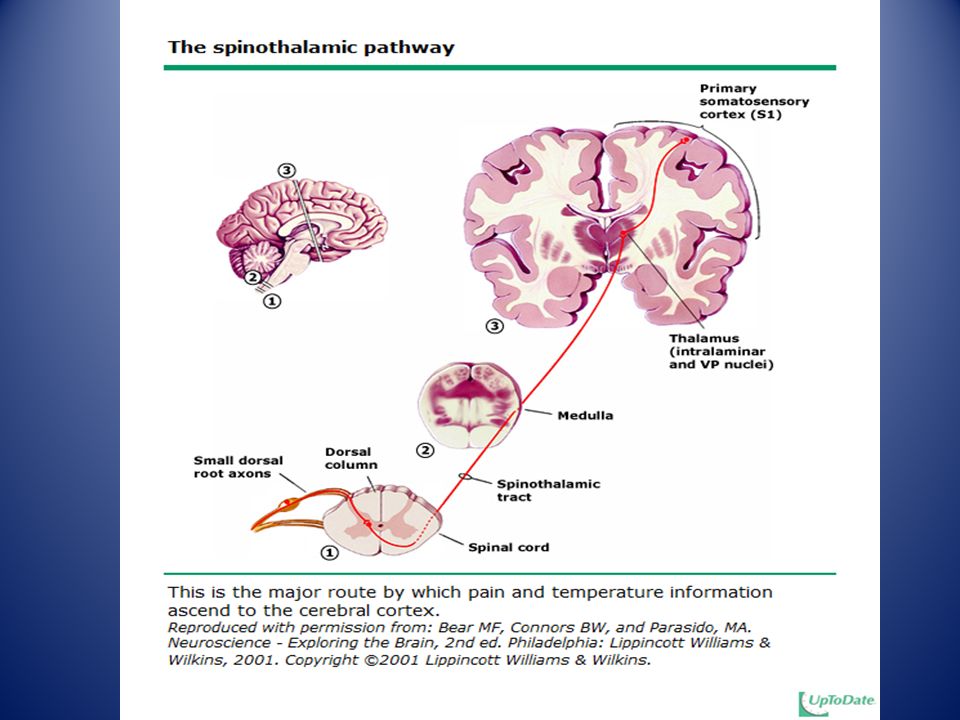
Nociceptive fibers – afferent fibers to dorsal horn – Two types A-delta – sharp pain (fast) C polymodal – dull pain (slow) Pathways Central processing – Interneurons between spinal cord/thalamus/cortex modulate pain and may be either excitatory of inhibitory – endogenous systems also control pain perception – opioid, noradrenergic (fight or flight), and serotonergic
 C polymodal – dull pain (slow) Pathways Central processing – Interneurons between spinal cord/thalamus/cortex modulate pain and may be either excitatory of inhibitory – endogenous systems also control pain perception – opioid, noradrenergic (fight or flight), and serotonergic")
13
Mechanisms for chronic pain Peripheral sensitization Central sensitization Disinhibition Desensitization Ectopic excitability Structural reorganization Phenotypic switch of neurons Primary sensory degeneration

14
Sensitization Main cause for hypersensitivity to pain after an injury (nociceptive sensitizer) Each has it’s own proposed mechanism at the cellular level – Peripheral – injury/inflammation releases cytokines, chemokines, bradykinin, histamine, prostaglandins – Central – amplifies info from nociceptors – NMDA receptor upregulated (controls pain – ketamine), GABA inhibition - disinhibition - “inhibits inhibition”
 Each has it’s own proposed mechanism at the cellular level – Peripheral – injury/inflammation releases cytokines, chemokines, bradykinin, histamine, prostaglandins – Central – amplifies info from nociceptors – NMDA receptor upregulated (controls pain – ketamine), GABA inhibition - disinhibition - inhibits inhibition")
15
Treatment – non drug strategies Exercise – PT, OT, stretching, strengthening – general conditioning Physical methods – ice, heat, massage Cognitive-behavioral therapy

16
Chiropracty Acupuncture TENS Alternative therapies – relaxation, imagery – herbals

17
WHO Ladder (adapted for elderly) –Level 3 (severe pain): Strong opioids—morphine, hydromorphone, fentanyl, oxycodone ±adjuvants –Level 2 (moderate to severe pain): Acetaminophen plus opioid (hydrocodone, oxycodone, codeine); tramadol ±adjuvants, Propoxyphene (X) –Level 1 (mild to moderate pain): Acetaminophen, aspirin (X), nonspecific NSAIDs (X), COX-2–specific NSAIDs±adjuvants Figure 1. WHO ladder (adapted for the elderly). Note: Therapies marked with an “X” are not appropriate for use in the elderly.
. Note: Therapies marked with an X are not appropriate for use in the elderly..")
18
Non-opioid options Acetaminophen Alpha-adrenergic agents Anticonvulsants Antidepressants Muscle relaxants Neuroleptic agents NMDA-receptor antagonists NSAIDs Oral local anesthetics Topical analgesics

19
Acetaminophen First line 4000mg max – 2000mg recommended with etoh use, liver disease, elderly Watch for other OTC’s containing acetaminophen

20
Alpha-adrenergics Epidural clonidine for neuropathic pain (FDA) Tizanidine outside US
 Tizanidine outside US")
21
Anticonvulsants Neuropathic pain Second gen may have fewer side effects (gabapentin, topiramate) Many approved for HA/pain – Carbamazepine (trigeminal neuralgia) – Divalproex (migraine) – Gabapentin (PHN) – Pregabalin (PHN, diabetic neuropathy) – Topiramate (migraine) – Duloxetine (diabetic neuropathy, fibromyalgia, DJD)
 Many approved for HA/pain – Carbamazepine (trigeminal neuralgia) – Divalproex (migraine) – Gabapentin (PHN) – Pregabalin (PHN, diabetic neuropathy) – Topiramate (migraine) – Duloxetine (diabetic neuropathy, fibromyalgia, DJD)")
22
Off label – Lamotrigine for HIV neuropathy (and others) – PDN Carbamazepine, phenytoin, gabapentin – Chronic musculoskeletal pain
 – PDN Carbamazepine, phenytoin, gabapentin – Chronic musculoskeletal pain")
23
Antidepressants Analgesia independent of antidepressant effects Tricyclics (amitriptyline) for neuropathic pain – Nortriptyline has safer side effect profile in > 60 – Amitriptyline relatively contraindicated in elderly (cardiac, anticholinergic) SNRI’s – Duloxetine, venlafaxine Others – Bupropion, venlafaxine, duloxetine (neuropathic) SSRI’s/SNRI’s not shown to have efficacy comparable to tricyclics
 for neuropathic pain – Nortriptyline has safer side effect profile in > 60 – Amitriptyline relatively contraindicated in elderly (cardiac, anticholinergic) SNRI’s – Duloxetine, venlafaxine Others – Bupropion, venlafaxine, duloxetine (neuropathic) SSRI’s/SNRI’s not shown to have efficacy comparable to tricyclics")
24
TRICYCLIC SSRI OTHER Amitriptyline Fluoxetine Venlafaxine Desipramine Paroxetine Duloxetine* Doxepin Sertraline Trazodone Imipramine Fluvoxamine Bupropion Nortriptyline Citalopram *FDA approved for pain

25
Muscle relaxants Cyclobenzaprine – Similar to tricyclic's – Acute LBP (2 trials) – Anticholinergic side effects, cardiac arrhythmia – Avoid in elderly Carisoprodol (meprobamate precursor) – Acute LBP – Dependency (physical, psychological), drowsiness Metaxalone (Skelaxine) – Non-sedating, watch for liver tox Baclofen – GABA agonist
 – Anticholinergic side effects, cardiac arrhythmia – Avoid in elderly Carisoprodol (meprobamate precursor) – Acute LBP – Dependency (physical, psychological), drowsiness Metaxalone (Skelaxine) – Non-sedating, watch for liver tox Baclofen – GABA agonist")
26
Neuroleptics Fluphenaxine (Prolixin) – Not recommended
 – Not recommended")
27
NMDA receptor antagonists Scientific promise – Dextromethorphan – Ketamine – Methadone – Memantine – Amitriptyline

28
NSAIDS 60 million Rx’s/yr (3.6 fold higher in elders) Clinical efficacy of equipotent doses is similar Individual responses highly variable – especially toxicity – cox-1 vs. cox-2 – naprosyn may have greatest relative cardiovascular safety profile – diclofenac - available as a topical patch for pain due to trauma and as a gel for treatment of painful joints – sulindac – increased hepatoxicity – indomethacin - GI and central nervous system adverse effects may be more frequent or severe than with other NSAIDs – ketorolac - Risk of gastropathy is increased when use exceeds five days – piroxicam – high GI toxicity – celecoxib – no antiplatelet function. Increased CV risk above 200mg/day

29
Generally indicated in mild to moderate pain Mostly for pain of somatic origin although has a CNS effect as well Each trial should last a couple weeks May have an opioid sparing effect as adjunct Protein bound – may interfere with other protein bound drugs (dilantin. coumadin)
.")
30
Noted variability in the response to NSAIDS between patients – Does not appear related to serum concentrations – Degree of Cox inhibition doesn’t correlate with effect – Non-prostaglandin effects may predominate in some patients – Switching between classes of NSAIDS may be beneficial

31
Topicals Lidoderm – FDA approved for PHN (intact skin) – Often used in musculoskeletal pain Diclofenac patch – Topical treatment of acute (short-term) pain due to minor strains, sprains, and contusions (bruises) Capsaicin – Neurotransmitter depletion – PHN, musculoskeletal
 – Often used in musculoskeletal pain Diclofenac patch – Topical treatment of acute (short-term) pain due to minor strains, sprains, and contusions (bruises) Capsaicin – Neurotransmitter depletion – PHN, musculoskeletal")
32
Tramadol Mu receptor and SNRI effects Effective in neuropathic pain, fibromyalgia, OA Similar side effects to opioids – Seizures, suicide

33
Benzodiazepines Adjuvant only Anxiolytic Limitations – Sedation – Addictive potential – Respiratory depression – Avoid in elderly Clonazepam – Effective in PHN and myoclonus

34
Opioids Role in treatment of pain is well established for acute pain, malignant pain and care of the terminally ill Role in chronic non-cancer pain is more controversial No specific studies have been performed in the elderly Decision to begin long term opioid therapy in chronic, non-cancer pain “must be weighed carefully”

35
Most of the literature on opioid therapy consists of reports of surveys and uncontrolled case series Most find that chronic pain can be controlled with nonescalating doses of opiates – up to 6 years of rx, 180 mg morphine – Function is improved by pt report – Cognitive function is preserved – Ability to drive or operate machinery is preserved – High drop out due to side effects (25%)
")
36
Establish diagnosis Confirm inadequacy of nonopioid and nonmedical treatments Ensure that the balance of risk and benefit favors treatment Explain benefits and risks and clinic’s monitoring policies Establish treatment goals Request written consent or contract, when necessary

37
Side effects Constipation Nausea, vomiting Sedation Impaired judgment Impaired psychomotor function Respiratory depression Hypotension Myoclonus GU Pruritus

38
Constipation – Fluids, fiber, stool softener, cathartic – methylnaltrexone Sedation – Methylphenidate, modafinil

39
Dosing – no universal agreement – Start with lowest dose of short acting preparation – Up titrate no more often than weekly – Convert to sustained release formulations when possible (25-50% of 24 hour total) – Monitor for efficacy, side effects
 – Monitor for efficacy, side effects")
40
“Blue Sheet”

41
Practice Partner Template – Is patient currently taking an opioid medication? – If yes is clicked, then: Is patient taking any adjuvant pain medications? Does patient report side effects? Based on pain assessment, plan to: (pick list of :) – Increase dosage of opioid pain medication – Decrease dosage of opioid pain medication – Add adjuvant pain medication – No changes planned to pain medication regimen
 – Increase dosage of opioid pain medication – Decrease dosage of opioid pain medication – Add adjuvant pain medication – No changes planned to pain medication regimen.")
Similar presentations















 Jason.>")



