Download presentation
Presentation is loading. Please wait.

1
Depart. Of Pulmonology & Critical Care Medicine R4 백승숙

2
In the late 1980s, Innovators first began using non-invasive ventilation in patients with acute respiratory failure as a potential alternative to endotracheal intubation The use of non-invasive ventilation varies greatly between hospitals and geographical regions, and has changed over time The low rate of use in some hospitals Little knowledge about or experience with the technique Insufficient technical equipment, and inadequate funding

5
Pressure-support ventilation Assists inspiration via a preset positive-pressure boost triggered by the patient Higher pressure is delivered until the inspiratory flow rate falls below a target pressure Allows the patient to set not only breathing rate but also inspiratory and expiratory durations Pressure-control ventilation Fluctuates between high inspiratory and low expiratory pressures The ventilator cycles into expiration when a preset inspiratory time is reached Patient is unable to control the duration of inspiration

6
Bilevel ventilation Pressure support - reduce inspiratory work Extrinsic positive end-expiratory pressure – counterbalance intrinsic positive end-expiratory pressure Achieves a greater reduction in work of breathing than does either mode alone, at least in patients with COPD CPAP Raise functional residual capacity Open flooded alveoli (ie, cardiogenic pulmonary edema) Lessen left ventricular transmural pressure Reducing afterload and increasing cardiac output
 Lessen left ventricular transmural pressure Reducing afterload and increasing cardiac output")
7
Proportional-assist ventilation Targets spontaneous inspiratory flow rate as a surrogate of patients’ effort Improve synchrony between patient and ventilator More comfortable and needs fewer adjustments More complex to use than pressure-support ventilation and has not been widely adopted

8
Skill of the caregivers and their extent of experience are important to the success of this technique Skill of the caregivers and their extent of experience are important to the success of this technique

9
Compared with invasive mechanical ventilation Same physiological benefits of reduced work of breathing and improved gas exchange Lower risk of nosocomial infections Less antibiotic use Less sedation requirement More rapid weanning Shorter lengths of stay in the intensive care units Lower mortality

11
Non-invasive ventilation can be used in a wide range of disorders that lead to acute respiratory failure The success of this technique depends Diagnosis of respiratory failure and patients’ characteristics When the ventilation is started The setting in which the patient is treated

14
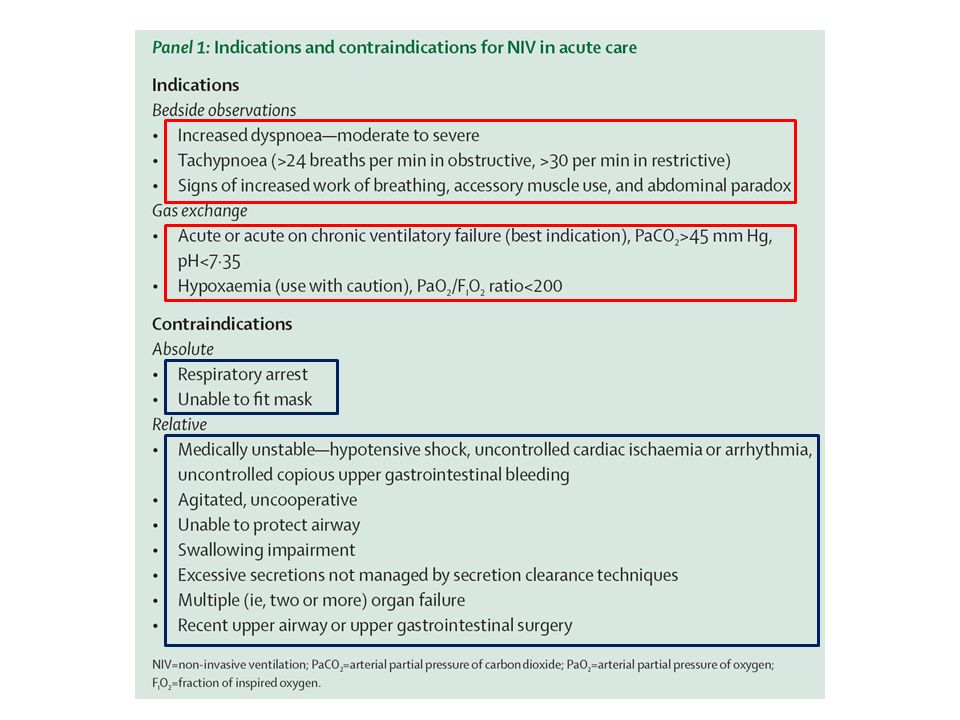
Early use of non-invasive ventilation is recommended The opportunity for a successful start Patients who are not in immediate life-threatening situations can be managed outside the intensive care units Not to be started too early‼

15
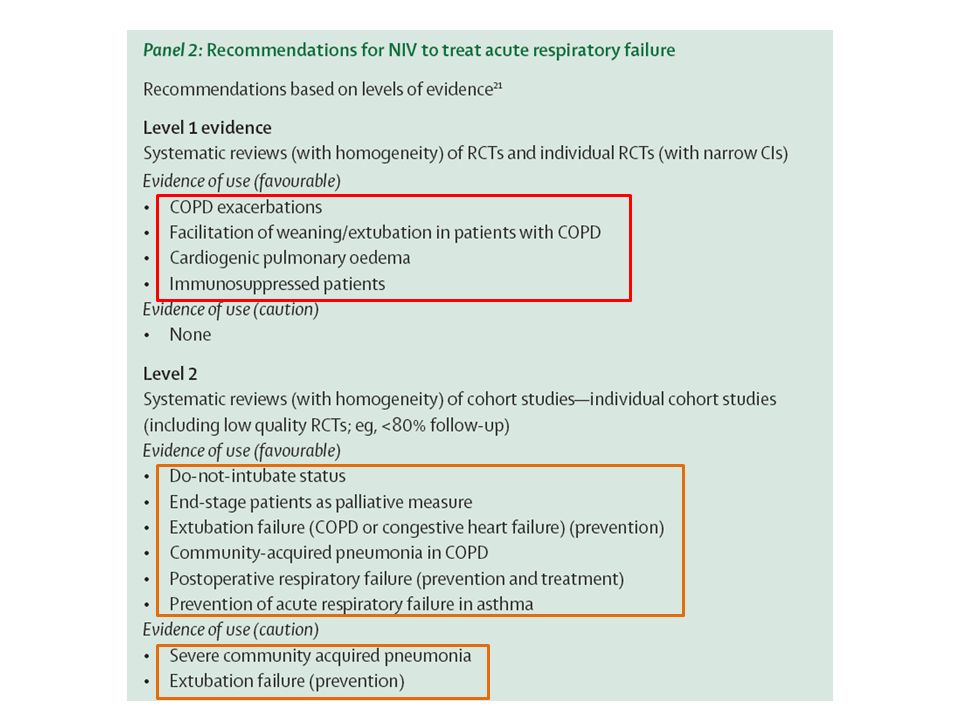
Patients with acute respiratory acidosis caused by an exacerbation of COPD are the group that benefits most from non-invasive ventilation A large multicentre trial Patients with mild to moderate acidotic COPD Intubation and mortality rates were lower with non-invasive ventilation than with standard therapy alone Subgroup analysis showed that these rates did not differ when pH at enrolment was less than 7.30 - Plant et al. 1. 보조 호흡근의 사용과 기이 복부운동 (paradoxical abdominal motion) 이 관찰되는 중등도 이상의 호흡곤란 2. 중등도 이상의 산증 (pH ≤7.35) 과 과탄산혈증 (PaCO2≥6.0 kPa or 45 mmHg) 3. 호흡수 > 25 회 이상 GOLD Guideline, 2005 1. 보조 호흡근의 사용과 기이 복부운동 (paradoxical abdominal motion) 이 관찰되는 중등도 이상의 호흡곤란 2. 중등도 이상의 산증 (pH ≤7.35) 과 과탄산혈증 (PaCO2≥6.0 kPa or 45 mmHg) 3. 호흡수 > 25 회 이상 GOLD Guideline, 2005
 이 관찰되는 중등도 이상의 호흡곤란 2. 중등도 이상의 산증 (pH ≤7.35) 과 과탄산혈증 (PaCO2≥6.0 kPa or 45 mmHg) 3. 호흡수 > 25 회 이상 GOLD Guideline, 보조 호흡근의 사용과 기이 복부운동 (paradoxical abdominal motion) 이 관찰되는 중등도 이상의 호흡곤란 2. 중등도 이상의 산증 (pH ≤7.35) 과 과탄산혈증 (PaCO2≥6.0 kPa or 45 mmHg) 3. 호흡수 > 25 회 이상 GOLD Guideline,")
16
Non-invasive ventilation has been used to treat acute respiratory failure in patients with cardiogenic pulmonary edema Oxygen therapy vs. –Reduction of intubation rate and mortality vs. CPAP –Intubation and mortality rates did not differ –More rapid improvements in dyspnea scores, oxygenation, PaCO2 Non-invasive ventilation and CPAP are regarded as first-line treatments together with standard medical therapy when acute respiratory failure ensues CPA P Non-invasive ventilation

17
Use of CPAP or non-invasive ventilation in the postoperative setting Postoperative complications (eg, Hypoxemia, Respiratory failure, Pulmonary atelectasis) CPAP ; reduced atelectasis and prevented pneumonia more effectively Non-invasive ventilation ; improved gas exchange and abnormal changes in pulmonary function Preventive use for a week before or immediately after surgery ; mitigate loss of lung volume and development of atelectasis
 CPAP ; reduced atelectasis and prevented pneumonia more effectively Non-invasive ventilation ; improved gas exchange and abnormal changes in pulmonary function Preventive use for a week before or immediately after surgery ; mitigate loss of lung volume and development of atelectasis")
18
Acute respiratory failure in patients who are immunocompromised, Early use of non-invasive ventilation could be very helpful Reduced intubation rate, complications, mortality, and duration of stay in intensive care units In view of the risk of admitting immunosuppressed to intensive care, Some institutions now use non-invasive ventilation or CPAP early in hematology wards, to avert transfer to intensive care

19
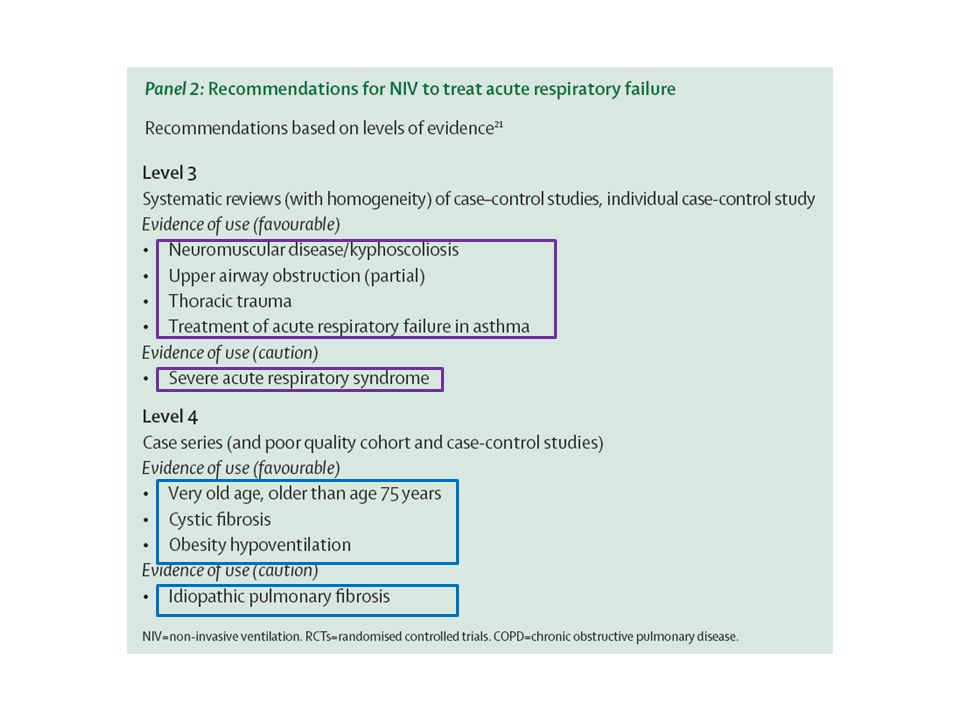
Obesity Chronic alveolar hypoventilation Usually in association with obstructive sleep apnea Non-invasive ventilation ; improved alveolar hypoventilation Patients with severe irreversible chronic diseases Non-invasive ventilation ; relieve symptoms and to achieve survival in hospital in some pts Underlying disease was an important determinant of survival

20
Use of non-invasive ventilation during severe, non-life threatening asthma attacks before development of acute respiratory failure Improved flow rates and reduced admissions Prevention of acute respiratory failure in patients with asthma who do not respond adequately to initial bronchodilator therapy

21
Use of non-invasive ventilation during fibreoptic bronchoscopy Patients at high risk for developing respiratory failure (eg, immunocompromised, have pneumonia and pulmonary fibrosis with a low PaO2, or have bleeding diatheses) Improved oxygenation, and reduced postprocedure respiratory failure in patients with severe hypoxemia
 Improved oxygenation, and reduced postprocedure respiratory failure in patients with severe hypoxemia")
22
The closely monitored intensive-care setting allows safe application of non-invasive ventilation even in very sick patients Staff with much experience in this technique are needed Prepared to intubate promptly if goals are not met Delays in intubation runs the risk of unanticipated respiratory or cardiac arrest with attendant morbidity and mortality

23
Predictors of failure for non-invasive ventilation For hypercapnic respiratory failure –No improvement or a fall in pH –No change or a rise in breathing frequency after 1–2 h –High-acuity illness at admission –Lack of cooperation For hypoxemic respiratory failure –No or a minimum rise in the ratio of PaO 2 to FIO 2 after 1–2 h –Patients older than 40 years (one study) –High acuity illness at admission –Presence of acute respiratory distress syndrome –Community acquired pneumonia with or without sepsis –Multi-organ system failure
 –High acuity illness at admission –Presence of acute respiratory distress syndrome –Community acquired pneumonia with or without sepsis –Multi-organ system failure")
24
Hypoxemic respiratory failure –Patients with dyspnea and tachypnea –Ratios of PaO 2 to FI O2 less than 200 –Non-COPD diagnosis (eg, pneumonia, ARDS, acute lung injury) In clinical trials –Large differences between enrolled patients in type of respiratory failure and severity of illness is major confounders –In a subgroup analysis only patients with COPD is effective –Not useful for community-acquired pneumonia in the absence of COPD
 In clinical trials –Large differences between enrolled patients in type of respiratory failure and severity of illness is major confounders –In a subgroup analysis only patients with COPD is effective –Not useful for community-acquired pneumonia in the absence of COPD")
25
Used to enable weaning from mechanical ventilation in stable patients recovering from an episode of hypercapnic acute respiratory failure (ie, COPD exacerbations) Applied immediately after extubation in patients considered at high risk of extubation failure lowered the rate of reintubation No reduction in reintubation rates Significantly higher mortality in the intensive care (one study), associated with longer delays in re-intubation than in the control group (12 h vs 2 h)
 Applied immediately after extubation in patients considered at high risk of extubation failure lowered the rate of reintubation No reduction in reintubation rates Significantly higher mortality in the intensive care (one study), associated with longer delays in re-intubation than in the control group (12 h vs 2 h)")
26
This technique has a role in treatment of extubation failure, but mainly in patients with hypercapnic and congestive heart failure who are at high risk for extubation failure Patients should be monitored closely to avoid delays in intubation

27
Systematically assessed the cost effectiveness of this technique

28
Non-invasive ventilation has an important role in the management of respiratory failure in acute-care hospitals Its use to treat acute respiratory failure related to COPD exacerbations, cardiogenic pulmonary edema, and patients in immunosuppressed states has gained wide acceptance Other potential applications are undergoing further investigation Use of this technique outside intensive care units is becoming common in many hospitals, but patients should be selected carefully to assure safety

Similar presentations








>")

 Dr. Meg-angela Christi Amores.>")








