Download presentation
Presentation is loading. Please wait.

1
Mona Saraiya, MD, MPH National Immunization Conference March 7, 2006 Division of Cancer Prevention and Control National Center for Chronic Disease Prevention and Health Promotion Burden of Cervical Cancer and Other HPV-Related Cancers Pap Screening Recommendations

2
Outline Surveillance Burden of Cervical Cancer Screening Diagnosis Costs Burden of other HPV-related cancers

3
The Most Common Cancers in Women Breast Cervix Ovary Endometrium Annual number of cases (thousands) More developed countries Less developed countries Colon/rectum Lung Stomach Adapted from Parkin et al, Eur J Cancer 37:S4, 2001 6000 200 400 200400 600
 More developed countries Less developed countries Colon/rectum Lung Stomach Adapted from Parkin et al, Eur J Cancer 37:S4,")
4
The Global Burden of Cervical Cancer Source: International Agency for Research on Cancer, 2003

5
Cervical Cancer Surveillance in the U.S. Cervical cancer incidence CDC’s National Program of Cancer Registries (NPCR) NCI’s Surveillance Epidemiology and End Results Program (SEER) Data from these two programs represent 96% of US population Cervical cancer deaths CDC’s National Center for Health Statistics Cervical cancer estimates American Cancer Society (ACS) Cervical pre-cancer/cytology No national registry
 NCI’s Surveillance Epidemiology and End Results Program (SEER) Data from these two programs represent 96% of US population Cervical cancer deaths CDC’s National Center for Health Statistics Cervical cancer estimates American Cancer Society (ACS) Cervical pre-cancer/cytology No national registry.")
6
Cancer Surveillance

7
Cervical Cancer Disease Burden in the U.S. Two types of cervical cancer Squamous cell carcinoma Adenocarcinoma (20% of all invasive cases) 2002 – 12,085 new cervical cancer cases (NPCR)* 2002 – 3,952 cervical cancer deaths (NCHS) # 2006 Estimates (ACS) + 9,710 new cervical cancer cases 3,700 cervical cancer deaths *U.S. count includes state cancer registries in the National Program of Cancer Registries that met certain data quality criteria for cancer incidence, and cover approximately 93% of the U.S. population. # Mortality data are from the National Vital Statistics Surveillance System, NCHS, and cover 100% of the U.S. population (www.cdc.gov/nchs)www.cdc.gov/nchs + Cancer Facts and Figures, 2006; American Cancer Society
 2002 – 12,085 new cervical cancer cases (NPCR)* 2002 – 3,952 cervical cancer deaths (NCHS) # 2006 Estimates (ACS) + 9,710 new cervical cancer cases 3,700 cervical cancer deaths *U.S. count includes state cancer registries in the National Program of Cancer Registries that met certain data quality criteria for cancer incidence, and cover approximately 93% of the U.S. population. # Mortality data are from the National Vital Statistics Surveillance System, NCHS, and cover 100% of the U.S. population ( + Cancer Facts and Figures, 2006; American Cancer Society.")
8
Age-Adjusted Invasive Cancer Incidence Rates, Among Women, U. S., 2000 United States Cancer Statistics: 2000 Incidence; NPCR

9
Cervical Cancer Mortality Rates, U.S., 1946-1984 Source: Program for Improving Clinical Pap Smear Programs and Management, Office of Population Affairs, DHHS, 1987.

10
Invasive Cervical Cancer Incidence and Mortality Rates,* by Race, SEER in US, 1975-2002 * Rates are per 100,000 and are age-adjusted to the 2000 U.S. standard population. Source: SEER Cancer Statistics Review, 1975-2002 Incidence Black Incidence White Death Black Death White

11
Invasive Cervical Cancer Incidence and Mortality Rates* by Race/Ethnicity, U.S., 1998-2001 Source: Saraiya M., et al., IPV Conference, 2005. *Incidence rates cover 77%, and mortality rates cover 100% of the U.S. population. † Hispanic is not mutually exclusive from white, black, and Asian/Pacific Islander. Hispanic † Non- Hispanic Age Adjusted Rates per 100,000 1510505 White Black Asian/Pacific Islander MORTALITYINCIDENCE

12
Invasive Cervical Cancer Incidence and Mortality Rates,* by Age Group, SEER in U.S., 1998-2002 *Source: SEER Cancer Statistics Review, 1975-2002 Incidence Death

13
Saraiya, M IPV Conference 2005

14
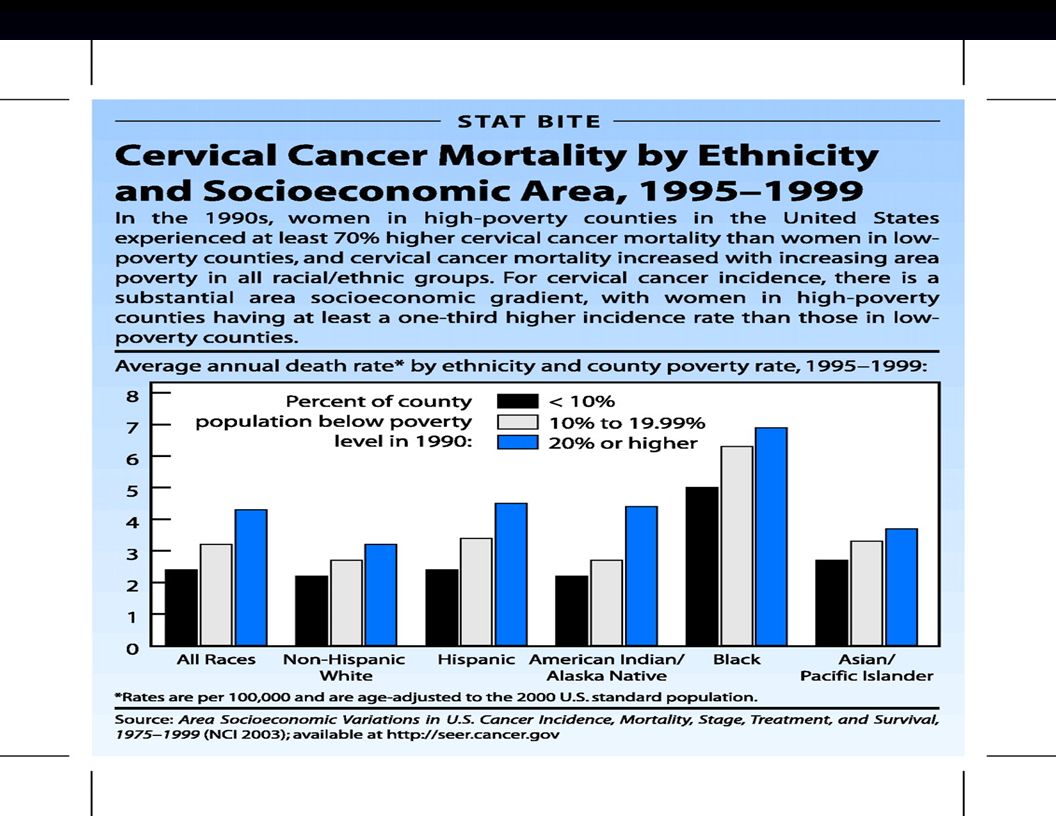
Age-adjusted Cervical Cancer Mortality Rates by State Economic Areas*, All Women, U.S., 1995-1999 Source: Grauman D., NCI; http://www3.cancer.gov/atlasplus/ *State Economic Area: One or more socio-economically similar counties within a state 3.93-6.76 3.21-3.93 2.53-3.21 0.90-2.53 Sparse

16
Cervical Cancer Mortality Rates, U.S. Born and Foreign-Born Women, U. S., 1985-1996 Foreign Born Total US Born Modified from Seeff et al., Cancer Detect Prev. 2003;27(3):203-8.
:")
17
Factors Contributing to Cervical Cancer Sources:NIH Consensus Conference Janerich, Connecticut Sung, California Never or Rarely Screened Cytology test abnormal, patient lost to follow-up Cytology test abnormal, mismanaged Rapidly progressive Uncommon cancers difficult to detect 5%-10% 10%-15% 5%-10% 9%-12% False negative cytology test 10%-15% 50%-60%

18
Cervical Cancer Screening Methods Conventional Cytology Sensitivity: 51–88% Specificity: 95–98% Liquid-based Cytology Sensitivity: 61-95% Specificity: 78-82% Source: Meyers et al., 2000; Nanda, et al., 2000; Belinson, et al., 2001

19
Cervical Cancer Screening Recommendations USPSTF 2003 ACS 2002 ACOG 2003 Age to start Age 21 or within 3 yrs of sexual activity Interval <30 yr ≥ 30 yr Conv: at least every 3 yrs Conv: 1 yr LBC: 2 yr 2-3 yrs 1 yr 2-3 yrs USPSTF – U.S. Preventive Services Task Force ACS – American Cancer Society ACOG – American College of Obstetricians and Gynecologists Conv – Conventional Cervical Cytology LBC – Liquid-based Cytology

20
Prevalence of Cervical Cancer Screening, National Health Interview Survey, United States, 2000 Swan J, Breen N, Coates RJ, Rimer BK, Lee NC. Progress in cancer screening practices in the United States: results from the 2000 National Health Interview Survey. Cancer. 2003;97:1528-40. Group % Pap test past 3 years All women82% Insured yes no 85% 62% Country of birth US born Foreign born in U.S. <10 yrs 83% 61% Race/Ethnicity Hispanic Non-Hispanic White Non – Hispanic Black Asian 77% 83% 84% 71%

21
Recent Pap Test Prevalence by Region of Birth and Time in the U.S., NHIS 1998-2003 Tsui J, ASCCP 2006 J et al, ASCCP

22
HPV Test – Hybrid Capture 2 (HC2) A nucleic acid solution hybridization assay with signal amplification that uses long synthetic RNA probes complementary to the DNA sequence of the 13 high risk HPV types. Easy to perform in clinical practice and amenable to automation The only system approved by FDA

23
FDA Approved Use of HPV Test Triage: Hybrid Capture II high risk panel (HC2) for ASC-US Pap test results Primary screening: HC2 as adjunct to Pap test in women 30 years of age and older. If both tests are negative, next cervical cancer screening should not occur for at least 3 years.

24
Organization Recommendations for HPV DNA Use in Cervical Cancer Screening USPSTFACSACOGASCCP ASC-US triageInsufficient Evidence Not addressedRecommended Primary screening with Pap test Not addressedOptionRecommended USPSTF – U.S. Preventive Services Task Force ACS – American Cancer Society ACOG – American College of Obstetricians and Gynecologists ASCCP – American Society of Colposcopy and Cytopathology

25
Abnormal Pap Test Results (Bethesda 2001) Squamous Cell Atypical squamous cells of undetermined significance (ASC-US) Atypical squamous cells cannot exclude high grade squamous intraepithelial lesion (ASC-H) Low grade squamous intraepithelial lesion (LSIL) HSIL Squamous Cell Cancer Glandular Cell Atypical glandular cells (AGC) Adenocarcinoma in situ (AIS) Adenocarcinoma
 Squamous Cell Atypical squamous cells of undetermined significance (ASC-US) Atypical squamous cells cannot exclude high grade squamous intraepithelial lesion (ASC-H) Low grade squamous intraepithelial lesion (LSIL) HSIL Squamous Cell Cancer Glandular Cell Atypical glandular cells (AGC) Adenocarcinoma in situ (AIS) Adenocarcinoma")
26
HSIL 300,000 CA 15,000 LSIL 1,000,000 ASC-US 2,000,000 Modified from Hildesheim, A., National Cancer Institute Estimated Annual Abnormal Pap Tests, U.S.

27
Evaluation of an Abnormal Pap Test Repeat cytology HPV DNA test Vaginal and cervical inspection Colposcopy with directed biopsy Endocervical curettage Bimanual pelvic examination

28
Modified from Chesson et al. Perspectives on Sexual and Reproductive Health 2004, 36(1): 11-19 Weinstock et al. Perspectives on Sexual and Reproductive Health 2004, 36(1): 6-10. Based on estimated incidence rates in 2000, in 2000 $US
: Weinstock et al. Perspectives on Sexual and Reproductive Health 2004, 36(1): Based on estimated incidence rates in 2000, in 2000 $US.")
29
Modified from Chesson et al. Perspectives on Sexual and Reproductive Health 2004, 36(1): 11-19) 90% 6%4%
: 11-19) 90% 6%4%.")
30
Cancers Attributable to Infection with Oncogenic HPV Types, U.S., 2002 SiteTotal Cancers* % Estimated HPV Attributable Fraction + Cervix12,085100 Anus 3,703 85 Vulva/Vagina 4,480 40 Penis 985 40 Oral/Pharyngeal10,088 15 *2002 US Cancer Statistics, CDC/NCI, 2005 +Parkin M. International Papillomavirus Conference, Vancouver, Canada, 2005/Trotter H, Franco E, Vaccine; 2006 in press

31
Summary Cervix Ca is the 11 th most common cancer in U.S. women; occurs mainly among rarely or never screened 12,085 new cancer cases and 3,952 cancer deaths in 2002 There are racial and socioeconomic disparities in cervical cancer incidence and mortality rates Cervical cancer screening has resulted in a 75% decrease in cervical cancer incidence in the U.S. Survival is high among women detected with early stage disease Cost of screening and managing results of abnormal Pap tests is in excess of $4 billion per year Other cancers also attributed to HPV; variation by site

32
Acknowledgement Herschel Lawson, MD Lauri Markowitz, MD Eileen Dunne, MD Beth Unger, MD, PhD HPV Vaccine Workgroup

Similar presentations



















 Connects the body.>")