Download presentation
Presentation is loading. Please wait.

1
Vascular Checks in Bolton Industrially Scaled and Systematically Applied Dr Stephen Liversedge PEC Chair Lynda Helsby Project Lead

4
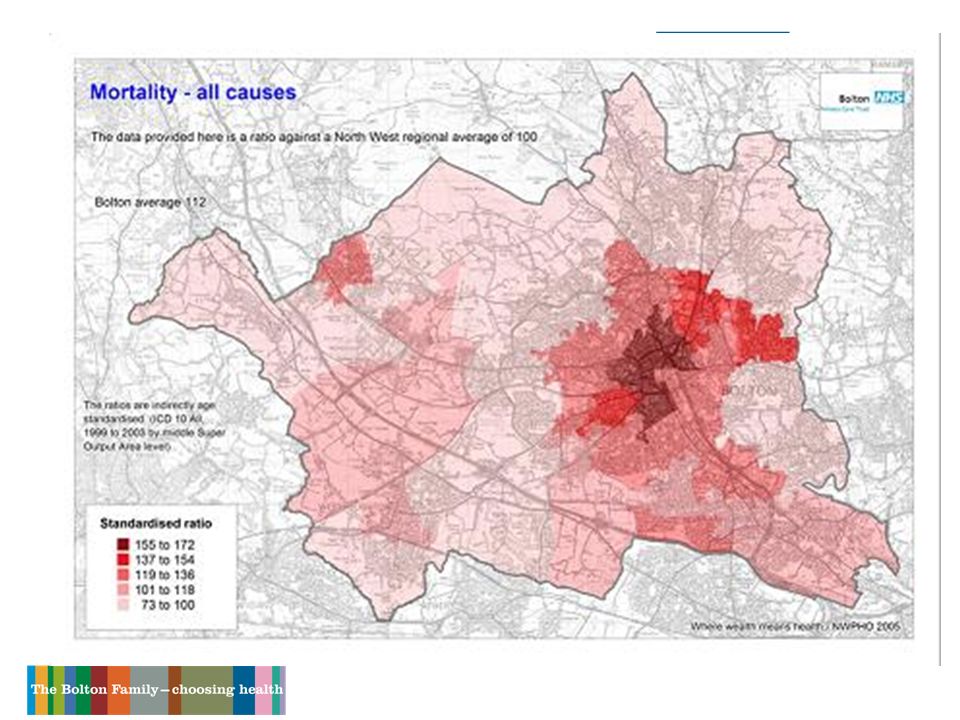
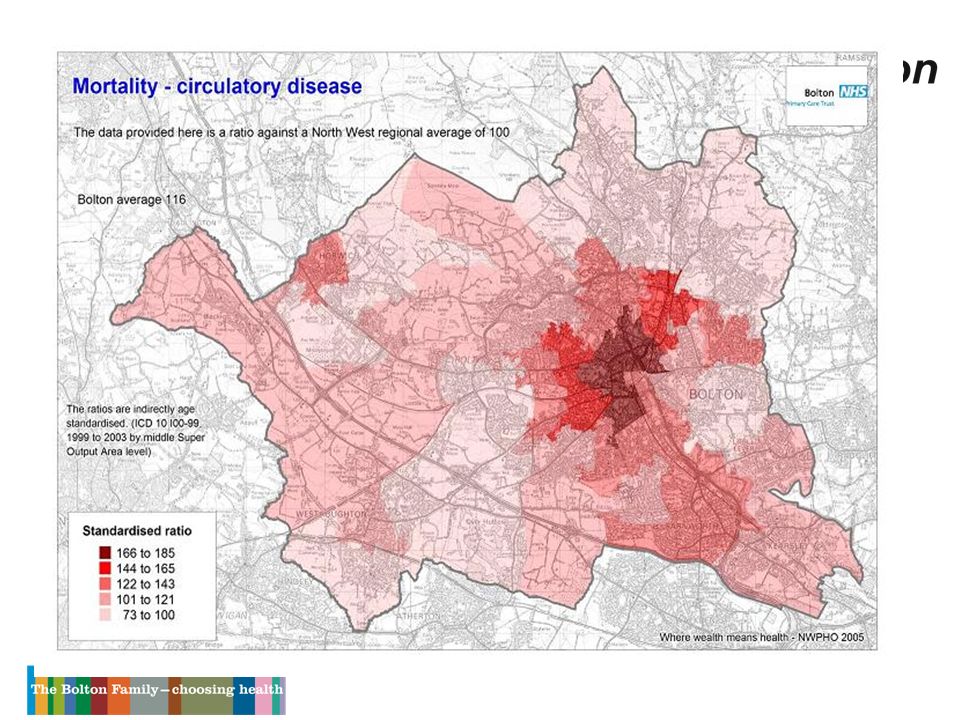
Health Inequalities 2010 Reduce deaths from heart disease and stroke and related diseases by 40% in people under 75

5
Health Inequalities 2010 Narrowing the Gap Males 74.6 years 2.3 year gap Females 79.0 years 2.1 year gap Great Lever, Halliwell and Crompton 67.5 years Bradshaw 82.2 years

6
Health Inequalities 2010 National Support Team visit 3 most ‘profitable’ areas to address Existing cardiovascular disease Diabetes Prevention of cardiovascular disease

7
Health Inequalities 2010 National Support Team visit Industrial scaling Systematically applied

8
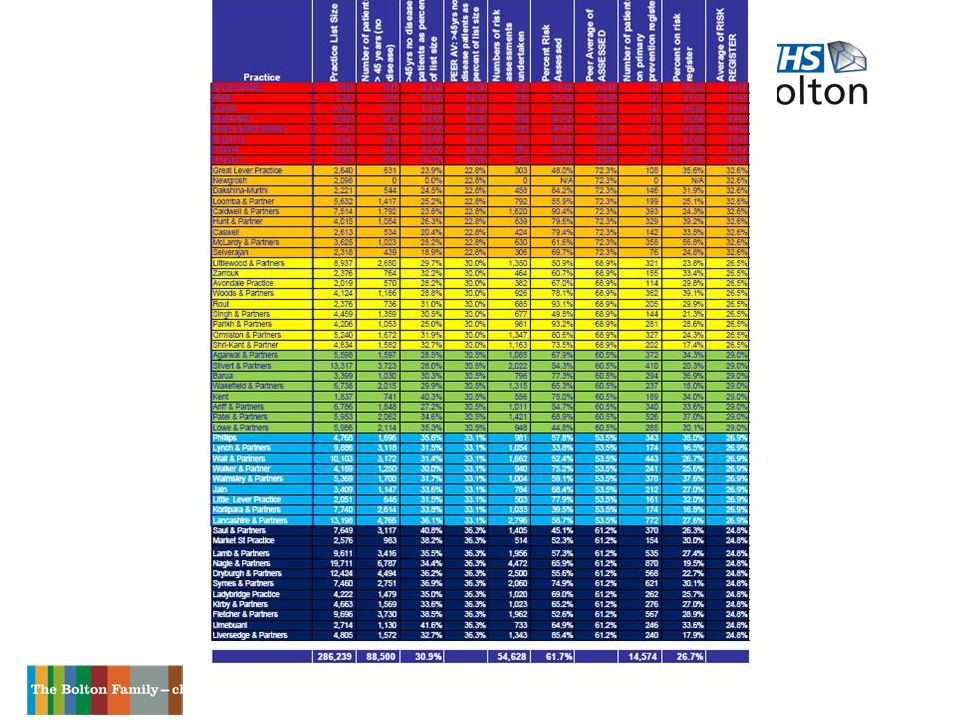
Primary Prevention of CHD 2006-2008 Incentive scheme Improve your position by 10% or 20% 10 practices didn’t participate Poor data in a further12 practices 74,769 target 31,518 assessed as at April 2007 Missing 43,251 Registers 15% to 25%

9
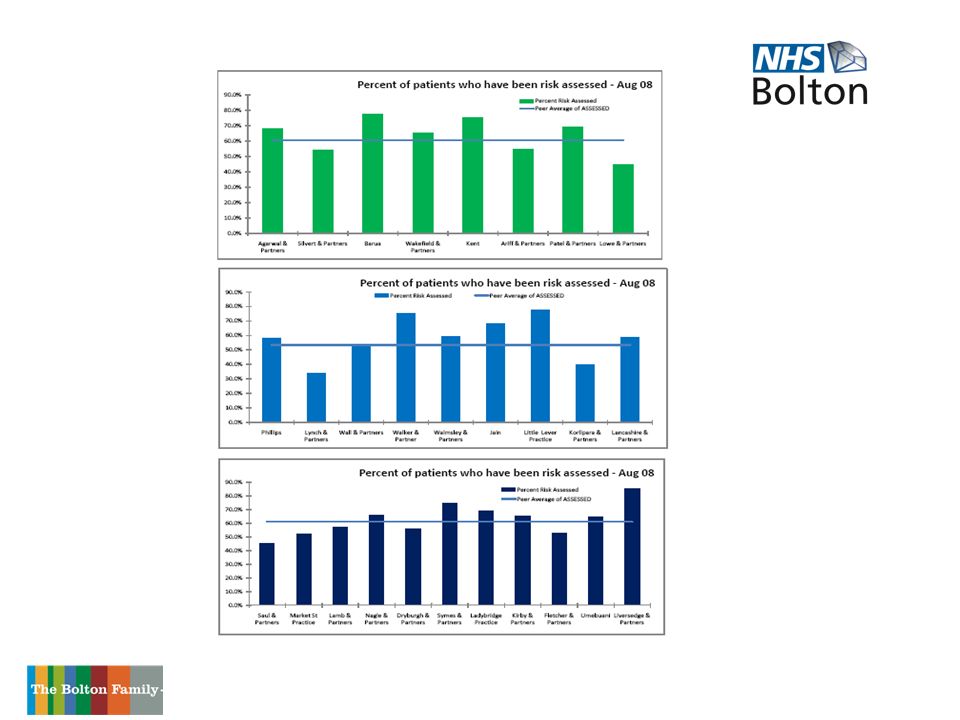
How were we doing?

10
Primary Prevention of CHD Logarithmic Incentivisation 30%£ 1.00 40%£ 1.50 50%£ 2.00 60%£ 3.00 70%£ 4.50 80%£ 6.50 90%£ 9.00 100%£12.00

11
Logarithmic Incentivisation

12
Costs 286,000 population 88,660 need assessment (31% of list) 70% is 62,062 @ 4.50 £279,275 80% is 70,925 @ 6.50 £471,651 90% is 79,794 @ 9.00 £789,960 100% is 88,660 @ 12.00 £1,003,920
 70% is 4.50 £279,275 80% is 6.50 £471,651 90% is 9.00 £789, % is £1,003,920")
13
Work and Pay How much? 31% of list 620 for each GP 80% achievement – 496 patients – £3224 90% achievement – 558 patients – £5022

14
Everyone must be involved - Staff Project Manager Health Trainers Data Quality Facilitators Practice Managers and reception staff Practice Nurses All GPs All Primary Care Staff And Secondary Care Staff

15
Everyone must be involved –The Public Local Authority The Bolton News Local Radio - Tower FM Work Places Supermarkets Pubs Betting shops Mosques

17
Practice Reports – Monthly Audit

18
Practice Trajectory

21
What is left to do? GreenAriff & Partners1,8401,2595813.20182 IndigoUmebuani1,1207943261.75186 YellowShri-Kant & Partner1,5991,2263732.00187 IndigoThe Market Surgery9735983752.00188 YellowLittlewood & Partners2,6401,6949465.00189 GreenSilvert & Partners3,7352,4291,3066.50201 GreenAgarwal & Partners1,5729106623.25204 IndigoFletcher & Partners3,7392,5521,1875.80205 GreenBarua1,0268192071.00207 IndigoNagle & Partners6,8554,7372,11810.00212 YellowSingh & Partners1,3419004412.00221 IndigoDryburgh & Partners4,3672,9451,4226.00237 GreenLowe & Partners2,0981,3757233.00241 BlueWall & Partners3,1961,8631,3335.50242 BlueLynch & Partners3,1261,9851,1414.67244 BluePhillips1,6751,1665092.00255 IndigoLamb & Partners3,4382,1181,3205.00264 BlueKorlipara & Partner2,6371,3761,2614.20300 OrangeNewgrosh602301 1.00301

22
How are we doing?

23
Results Preventing Heart Disease Improved performance ‘Beyond QOF’ Better Diabetes, Hypertension, CKD registers Better Primary Health Care Teams Better Primary Prevention Registers 9,097 on register at 2007 Currently 17,646 @ January 2009 24,000 expected on register…….eventually

24
Before

25
After!

26
Workstreams Information Data Quality Clinical Engagement Outreach work Health trainers Marketing Local Enhanced Scheme Near Patient testing Clinical Governance

27
Learning Points - Information Regular reports vital for practice and project team Adapt information depending on outcomes Interpretation of information is variable Project team must focus on information and act accordingly

28
Learning Points - Data Quality Assume nothing Ensure searches are systematic Support is necessary for running searches Training requirements exposed Capacity of Data Quality Facilitators

29
Learning Points - Clinical Engagement Clinical Leadership is essential Time to build relationships Understand your Primary Care Get a lead in each practice Culture and ethos determines the success

30
Learning Points - Outreach work Good marketing exercise Well received everywhere Data quality and transfer Cost issue Duplication Targeted outreach the most effective

31
Learning Points - Health Trainers Vital Moveable resource Adaptable Flexible Resilient Enthusiastic

32
Learning Points - Marketing Branding – appealing, recognised, catchy Launch event success Publicity Media involvement Banners Cost

33
Learning Points - Local Enhanced Scheme Grab attention Different - logarithmic incentivisation Acknowledges work already done Acknowledges it gets harder No strings attached Aims for 100%

34
Learning Points - Near Patient Testing One stop shop Helps with needle phobics Training /Quality assurance issues Cost Laboratory support

35
Learning Points - Clinical Governance Risk calculation tools Management of risk register patients Training Support NICE guidance

36
Final Learning Points 1 Select your project team carefully Shared ambition Enthusiastic Informed Prepared to challenge Prepared to support

37
Final Learning Points 2 Health Inequalities: Deprivation Score No. of Practices % Achieved >401479.4% 30 – 401873.7% 20 – 301275.2% <201174.3%

38
Final Learning Points 3 The Last 20% – Half (10%) mean to attend – Busy…. and Well – Work commitments Last 10% – Ghosts – Needle phobics – 4 urban myths – Leave me alone

39
Final Learning Points 4 To do it this way you need Clinical Leader Project Team Incentive scheme Peer group cluster analysis Practice Visits Health Trainers Outreach Publicity All equally important

40
Before

41
After!

Similar presentations










 (13.45 – 15.00)>")








