Download presentation
Presentation is loading. Please wait.

1
Centering Pregnancy in FM Residency Can we do it? Donna M Cohen MD Beth E Freedman MD Michael R Loeven MD Lancaster General Family Medicine Residency Lancaster, PA

2
Disclosures No Disclosures

3
Today’s Objectives Present our experience as a family medicine residency program with Centering Pregnancy Discuss the pros and cons of implementing Centering Pregnancy within one’s curriculum

4
What is Centering Pregnancy? Model of Healthcare that integrates Health Assessment, Education and Support in a group setting. Women are empowered to choose health- promoting behaviors. Lower rate of pre-term birth, higher birth weight, higher rate of breastfeeding initiation and higher rates of post partum contraception use. Increased satisfaction of care for patients and providers.

5
Lancaster General Hospital Family Practice Residency Located in downtown Lancaster PA Provide care for largely Hispanic, underserved population 39 residents Strong obstetric/ maternal-child health curriculum –Approximately 800 deliveries/ year –Approximately 400 prenatal/ year @ downtown clinic

6
Our History with Centering Pregnancy Initially began providing Centering in 2009 Small fraction of prenatal patients participated Small fraction of residents, faculty, and nurses served as co-facilitators Only a few faculty/residents received Centering Pregnancy training

7
Early Barriers Poor awareness of Centering (benefits/ logistics) Poor continuity within groups –Patients –Residents Providers struggled with “losing their personal patients” Funding (relied heavily on grants) –Snacks –Incentives –Curriculum guides
 Poor continuity within groups –Patients –Residents Providers struggled with losing their personal patients Funding (relied heavily on grants) –Snacks –Incentives –Curriculum guides")
8
Our Turning Point… Resident champion(s) Faculty champion(s) Partnership with Healthy Beginnings Plus –Department of Health grant funding In 2011, began opt-out approach and became a fully integrated part of resident curriculum In 2012, we committed to obtaining CHI certification October 2013 Site Visit March 2014 Site Approval
 Faculty champion(s) Partnership with Healthy Beginnings Plus –Department of Health grant funding In 2011, began opt-out approach and became a fully integrated part of resident curriculum In 2012, we committed to obtaining CHI certification October 2013 Site Visit March 2014 Site Approval")
9
Approval Process 2009 2011 2014 …

10
Approval Process Connect with CHI through website –Readiness assessment tool Start training a few faculty/residents Pilot with interested residents 1-2 groups Always keep in mind expansion, or it won’t happen! Once you’ve worked out the kinks-expand to full capacity and start collecting data Site visit-1.5 days with group observation and review of your process Conditional Approval vs Approval

11
Centering Pregnancy in Family Medicine Residency Benefits and Challenges

12
Challenges Time! Scheduling! Cost! Space! Patients!

13
Time CHI requires recording of outcomes Monthly Steering Committee Meetings Pre-Visit Planning time for residents Time for data analysis Ongoing Faculty Training Resident training (1/2 day)
")
14
Time Need support and buy in from Program Director, Medical Director, Staff Administrative Assistant dedicated to Centering would be ideal!

15
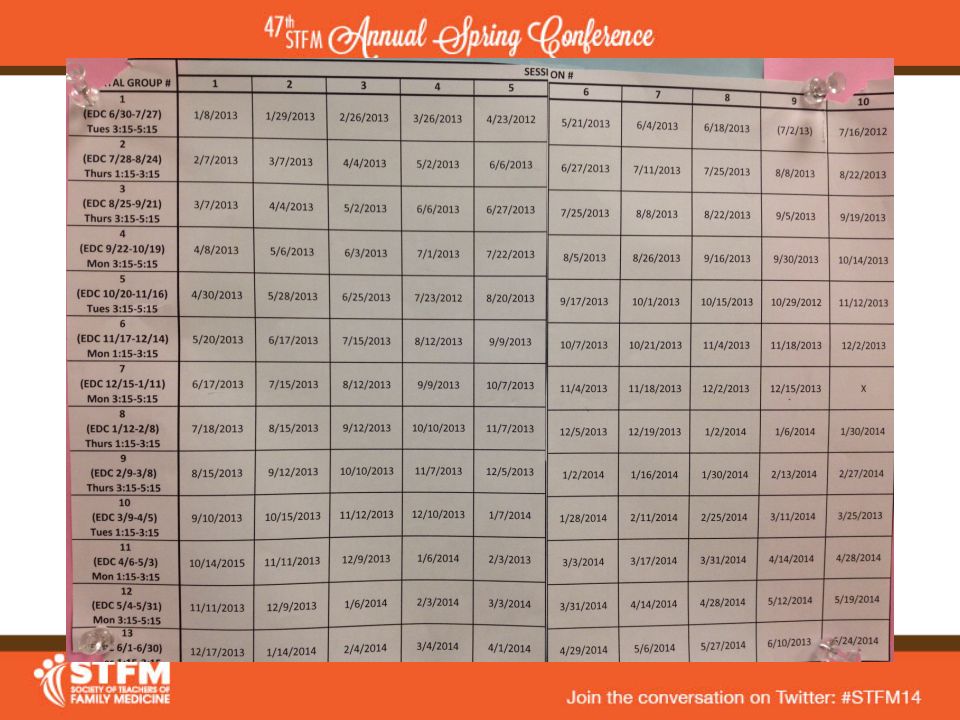
Scheduling CHI requires that women are assigned to a group cohort and remain in same group Each group meets 10 times (16, 20, 24, 28, 30, 32, 34, 36, 38, 40 wks) Each group lasts 2.5 hours (including set up/tear down time) Ideally should take place of a half-day clinic for resident
 Each group lasts 2.5 hours (including set up/tear down time) Ideally should take place of a half-day clinic for resident")
16
Scheduling CHI requires stability of group leadership R2 and R3 do initial prenatal visit in office R2 and R3 share each group; ideally both should be present at each session Continuity of faculty/nurse facilitator Residents scheduled to facilitate groups that will deliver during their OB service month

19
Cost Training $$$ –CHI requires all facilitators to have level 1 training; 30% to have level 2 training –Level 1 training=$850/person –Level 2 training=$500 For LGH: 10 Level 1 providers, 4 Level 2 providers ($10,500)
")
20
Cost Site Approval $$ ($5,000) Annual CHI membership fee $250 Patient Supplies $ –Notebooks $22 each ($4000) –Snacks (~$30 per group) –Promotional Items –Incentives 2 $25 Baby’s R Us Gift Cards Baby Items (~$15/each)
 Annual CHI membership fee $250 Patient Supplies $ –Notebooks $22 each ($4000) –Snacks (~$30 per group) –Promotional Items –Incentives 2 $25 Baby’s R Us Gift Cards Baby Items (~$15/each)")
21
Cost Local March of Dimes Chapter Women’s Giving Circle Grant-$3,475 Wal-Mart Grant-$500 Healthy Beginning Plus-DOH Grant Donations

22
Space CHI requires: –Assessments occur within the group space and is set ‐ up to ensure privacy –All group participants sit in the circle –Centering space is private and conducive to group sharing –Seating is around an open space that allows for activities –Snacks are provided at each group session, music overhead –Centering has priority for use of the space; other uses do not hinder Centering –Space is of sufficient size for a group of at least 10 mothers, their support people, and Centering staff to comfortably sit in a circle, with additional room for assessment –The space is comfortable and inviting to participants

26
Number of Prenatal Patients CHI require 60% of eligible patients to be enrolled in Centering CHI requires average group size 8-12 patients For LGH: –300 prenatal patients/year at DFM –95 Enrolled in Centering –72 Completed

27
Strategies to Increase Patients Decrease Denominator by removing Spanish Speaking patient Increase Numerator by making Centering “Opt Out” Enroll at any time of pregnancy “Standard of Care”-Staff Education Advertisements Incentives

29
Benefits to Patients Improved Outcomes Increased prenatal education (20 vs 2 hrs) Better continuity of prenatal care and delivery Increased patient satisfaction Ongoing social support and connections Community Building
 Better continuity of prenatal care and delivery Increased patient satisfaction Ongoing social support and connections Community Building")
30
First Year Outcomes Centering Group (N=72) LGH FM Residency (N=790) National Average (CDC 2012) C-Section Rate 24% 30-33%32% Preterm Birth Rate 7% 10.8%11.5% Low Birth Weight 7% 8% Breastfeeding at DC 74% 76% Breastfeeding at PP 28% 37% Rate of PP Follow Up 83% 44-65%
 LGH FM Residency (N=790) National Average (CDC 2012) C-Section Rate 24% 30-33%32% Preterm Birth Rate 7% 10.8%11.5% Low Birth Weight 7% 8% Breastfeeding at DC 74% 76% Breastfeeding at PP 28% 37% Rate of PP Follow Up 83% 44-65%")
31
Benefits to Resident Develop skills in facilitating group visits Learn and practice team-based care Learn and practice facilitative leadership Develop skills in pre-visit planning Standardized prenatal curriculum Increased provider satisfaction Increased continuity deliveries

32
Benefits to Faculty Relaxed and fun environment Direct observation of resident Milestones: PC3 Partners with patient, families and communities to improve health SBP4 Coordinates team based care PROF3 Demonstrates humanism and cultural proficiency

33
Resident Feedback “It is the hardest thing I have done in residency, which is saying a lot. The work pays off though, you see the difference with Centering patients as soon as you see them come through the door at Women and Babies Hospital.” R3 “It was a huge draw to this (residency) program specifically.” R1
 program specifically. R1.")
34
Resident Feedback “I have the luxury to spend time digging into difficult and important issues in pregnancy and I thought, THIS is why I went into medicine!” R1 “I get to know patients and their families well. Patients seem to bond well with each other.” R2

35
Resident Feedback “I feel like it takes prenatal patients away from 1st years and I want them to be my patients (and deliveries)!” R1 who hasn’t done Centering yet
! R1 who hasn’t done Centering yet")
36
Faculty Feedback OB Attending during a high-risk delivery: "You know, the whole time I was seeing her, I kept wondering why she even attended Centering with all of her risk factors. Now I get it."

37
Next Steps Call Local March of Dimes Chapter Assess program’s ability to handle cost, scheduling, patient flow Contact Centering Healthcare Institute to arrange training Connect with other residencies running group prenatal visits/Centering!

38
Questions/Discussion

39
References Group prenatal care and perinatal outcomes: A randomized controlled trial. Ickovics JR, Kershaw TS, Westdahl C, Magriples U, Massey Z, Reynolds H, Rising Obstet Gynecol. 2007;110(2 Pt 1):330 Group prenatal care and preterm birth weight: results from a matched cohort study at public clinics. Ickovics JR, Kershaw TS, Westdahl C, Rising SS, Klima C, Reynolds H, Magriples U Obstet Gynecol. 2003;102(5 Pt 1):1051 The effect of CenteringPregnancy group prenatal care on preterm birth in a low-income population.Picklesimer AH, Billings D, Hale N, Blackhurst D, Covington-Kolb S Am J Obstet Gynecol. 2012;206(5):415.e1 The impact of Centering Pregnancy Group Prenatal Care on postpartum family planning. Hale N, Picklesimer AH, Billings DL, Covington-Kolb Am J Obstet Gynecol. 2014 Jan;210(1):50.e1-7. Epub 2013 Sep 7 Wendy L. Bennett, Hsien-Yen Chang, David M. Levine, Lin Wang, Donna Neale, Erika F. Werner, Jeanne M. Clark. Utilization of Primary and Obstetric Care After Medically Complicated Pregnancies: An Analysis of Medical Claims Data. Journal of General Internal Medicine, 2014;
:330 Group prenatal care and preterm birth weight: results from a matched cohort study at public clinics. Ickovics JR, Kershaw TS, Westdahl C, Rising SS, Klima C, Reynolds H, Magriples U Obstet Gynecol. 2003;102(5 Pt 1):1051 The effect of CenteringPregnancy group prenatal care on preterm birth in a low-income population.Picklesimer AH, Billings D, Hale N, Blackhurst D, Covington-Kolb S Am J Obstet Gynecol. 2012;206(5):415.e1 The impact of Centering Pregnancy Group Prenatal Care on postpartum family planning. Hale N, Picklesimer AH, Billings DL, Covington-Kolb Am J Obstet Gynecol Jan;210(1):50.e1-7. Epub 2013 Sep 7 Wendy L. Bennett, Hsien-Yen Chang, David M. Levine, Lin Wang, Donna Neale, Erika F. Werner, Jeanne M. Clark. Utilization of Primary and Obstetric Care After Medically Complicated Pregnancies: An Analysis of Medical Claims Data. Journal of General Internal Medicine, 2014;.")
Similar presentations
















, Executive.>")






