Download presentation
Presentation is loading. Please wait.

1
Cough(咳) Pathophsiology, Dx & Tx
박 명재 호흡기내과

2
Cough Chronic cough is a major unmet[목표가 채워지지 않은] clinical need and safe and effective therapies are urgently needed. Major Sx. in 10-30% of respiratory Dr. Total world market for cough Rx:40억$ Barnes PJ. The problem of cough and development of novel antitussives. Pulm Pharmacol Ther 2007; 20:
![Cough Chronic cough is a major unmet[목표가 채워지지 않은] clinical need and safe and effective therapies are urgently needed.](http://slideplayer.com/slide/10768594/38/images/2/Cough+Chronic+cough+is+a+major+unmet%5B%EB%AA%A9%ED%91%9C%EA%B0%80+%EC%B1%84%EC%9B%8C%EC%A7%80%EC%A7%80+%EC%95%8A%EC%9D%80%5D+clinical+need+and+safe+and+effective+therapies+are+urgently+needed..jpg "Major Sx. in 10-30% of respiratory Dr. Total world market for cough Rx:40억$ Barnes PJ. The problem of cough and development of novel antitussives. Pulm Pharmacol Ther 2007; 20:")
3
RAR Barnes PJ. The problem of cough and development of novel antitussives. Pulm Pharmacol Ther 2007; 20:

5
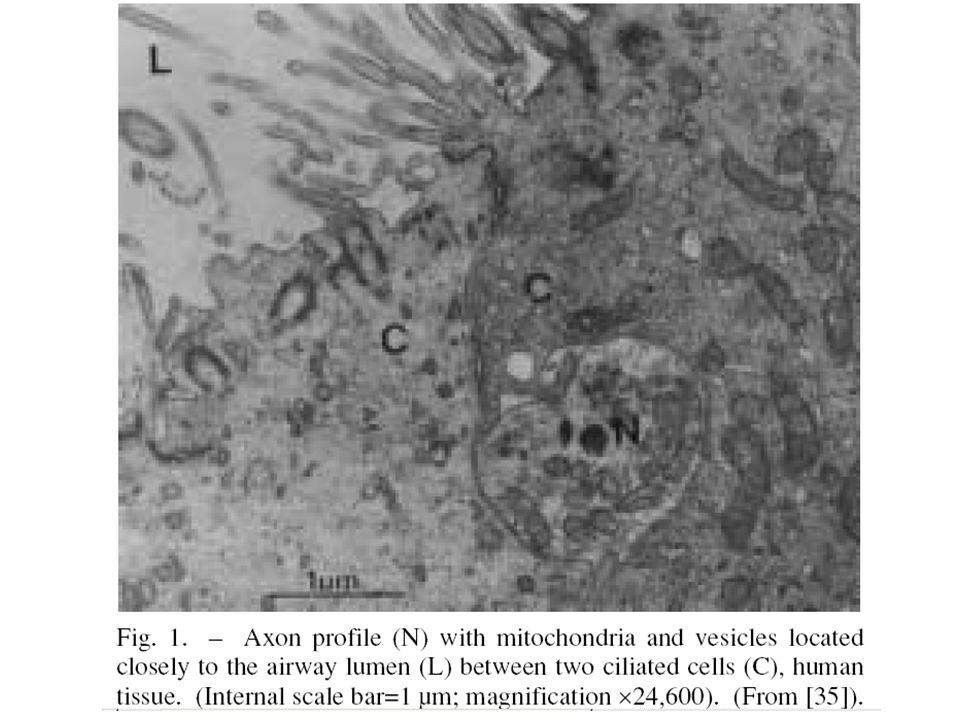
Types of sensory receptors in the lungs and lower respiratory tract
Receptor Site Fibre Slowly adapting stretch Smooth muscle airway Aα-β Rapidly adapting stretch Airway epithelium Aδ(M) (irritant receptor) Pulmonary C-fibre Alveolar wall C(NM) Bronchial C-fibre Airway wall C(NM) Neuroendocrine body Airway epithelium ?
 (irritant receptor) Pulmonary C-fibre Alveolar wall C(NM) Bronchial C-fibre Airway wall C(NM) Neuroendocrine body Airway epithelium")
6
Eccles R. Understanding the symptoms of the common cold and influenza
Eccles R. Understanding the symptoms of the common cold and influenza. Lancet Infect Dis. 2005;5:

7
Tennis ball=80kph Base ball=140kph Intarthoacic Pressure 300mmHg↑ Cough=160kph

9
Cough-induced rib fracture
from October 2003 to December 2007. Among 54 patients suspected cough-induced rib fractures, 20 patients were confirmed the diagnosis of cough-induced rib fracture. Mean age = 46±18.8 years male:female=12:8 Bone scan demonstrated all (20) cases of rib fracture. Only one case was revealed by chest radiography. Right-sided rib fractures alone in 15 patients(21 Fx ribs), Left-sided alone in 4 patients(4 Fx ribs), Bilateral lesion in 1 patient. The fractures were most common at the anterior aspect of the Rt. side, from 5th to 8th Rib.
 cases of rib fracture. Only one case was revealed by chest radiography. Right-sided rib fractures alone in 15 patients(21 Fx ribs), Left-sided alone in 4 patients(4 Fx ribs), Bilateral lesion in 1 patient. The fractures were most common at the anterior aspect of the Rt. side, from 5th to 8th Rib.")
10
Reflex responses to receptor stimulation
C-fiber receptors RARs Pulmonary Bronchial Apnoea Apnoea Cough Tachypnoea Tachypnoea Tachypnoea Cough inhibition Augmented breaths Bronchoconstriction Bronchoconstriction Bronchoconstriction Mucus secretion Mucus secretion Mucus secretion Laryngoconstriction Laryngoconstriction Vasodilation Vasodilation Somatic inhibition capsaicin, bradykinin, acid hypo,hypertonic saline low Cl soultion mechanical stimuli

12
Summary of Studies on the Effects of Mucociliary Drugs on Cough
Guaifenesin(페나투신) vs placebo 2:2 Iodinated glycerol(뮤코라마) vs placebo 2:1 Ipratropium vs placebo 2:0 Oxitropium vs placebo 0:1 Tiotropium vs placebo 0:1 Bromhexine vs placebo 1:3 Carbocysteine vs placebo 0:2 Acetylcysteine vs placebo 1:2 Mercaptoethane sulphonate vs placebo 0:2 Hypertonic saline vs placebo 0:1 Donald C. Bolser, Clinical Practice Guidelines Protussive Therapy: ACCP Evidence-Based Cough Suppressant and Pharmacologic Chest 2006;129
 vs placebo 2:2. Iodinated glycerol(뮤코라마) vs placebo 2:1. Ipratropium vs placebo 2:0. Oxitropium vs placebo 0:1. Tiotropium vs placebo 0:1. Bromhexine vs placebo 1:3. Carbocysteine vs placebo 0:2. Acetylcysteine vs placebo 1:2. Mercaptoethane sulphonate vs placebo 0:2. Hypertonic saline vs placebo 0:1. Donald C. Bolser, Clinical Practice Guidelines Protussive Therapy: ACCP Evidence-Based. Cough Suppressant and Pharmacologic Chest 2006;129.")
13
Drugs That Affect Mucociliary Factors
Recommendations 1. In patients with chronic bronchitis, agents that have been shown to alter mucus characteristics are not recommended for cough suppression. Level of evidence, good; benefit, none; grade of recommendation, D 2. In patients with cough due to URI or chronic bronchitis, the only inhaled anticholinergic agent that is recommended for cough suppression is ipratropium bromide. Level of evidence, fair; benefit, substantial; grade of recommendation, A

14
Drugs That Affect the Afferent Limb of the Cough Reflex
Summary of Studies on the Actions of Peripheral Cough Suppressants Levodropropizine(레보투스) vs placebo 1:0 Moguisteine vs placebo 2:0 Na cromoglycate(Intal®)
 vs placebo 1:0. Moguisteine vs placebo 2:0. Na cromoglycate(Intal®)")
15
Drugs That Affect the Afferent Limb of the Cough Reflex
Recommendations 3. In patients with chronic or acute bronchitis, peripheral cough suppressants, such as levodropropizine and moguisteine, are recommended for the short-term symptomatic relief of coughing. Level of evidence, good; benefit, substantial; grade of recommendation, A 4. In patients with cough due to URI, peripheral cough suppressants have limited efficacy and are not recommended for this use. Level of evidence, good; benefit, none; grade of recommendation, D

16
Drugs That Affect the Central Mechanism for Cough
Codeine vs placebo 3:1 Dextromethorphan vs placebo 3:3 Pipazethate vs placebo 0:1 Sensory information spurapotine

17
Drugs That Affect the Central Mechanism for Cough
Recommendations 5. In patients with chronic bronchitis, central cough suppressants, such as codeine and dextromethorphan, are recommended for the short-term symptomatic relief of coughing. Level of evidence, fair; benefit, intermediate; grade of recommendation, B 6. In patients with cough due to URI, central cough suppressants have limited efficacy for symptomatic relief and are not recommended for this use. Level of evidence, good; benefit, none; grade of recommendation, D

18
Drugs That Affect the Efferent Limb of Cough Reflex
Baclofen:muscle relaxant with spinal action ACEI induced cough Drugs That Affect the skeletal muscles Succinylcholine Propofol Atracurium+propofol > propofol alone Recommendation 7. In patients with chronic or acute cough requiring symptomatic relief, drugs that affect the efferent limb of the cough reflex are not recommended. Level of evidence, low; benefit, none; grade of recommendation, D

19
Pharmacologic Enhancement of Cough Clearance
hypertonic saline solution and erdosteine: effective agents for increasing in patients with bronchitis Amiloride: effective cough clearance in patients with CF. Ineffective agents (in bronchitic patients); carbocysteine, mercaptoethane sulfonate, bromhexine, and guaifenesin. recombinant Dnase: improve PFT dry-powder mannitol increased
; carbocysteine, mercaptoethane sulfonate, bromhexine, and guaifenesin. recombinant Dnase: improve PFT dry-powder mannitol increased")
20
Potential Future Antitussive Therapies
Opioid:by inhalation, nociceptin (dual) Large-conductance potassium (maxi-K) channel openers; inhibit sensory N activation: NS169 TRP receptor (vanilloid receptor); capsaicin activated specific ion channel of C-fiber :capsazepine , menthol Chloride channel;Furosemide inhalation (cough with low Cl- solution, not with capsaicin induced cough) Tachykinin receptor antagonists; NK2 RA;SR48968 Prostaglandin inhibitors; sulindac, aspirin Neurotrophin inhibitors; NGF blocking Ab Cannabinoid agonist: CP55940, JWH133 5-HT1A(serotonin) receptor agonists: methysergide Theobromine;chocolate, cocoa inhibit capsaicin cough
 Large-conductance potassium (maxi-K) channel openers; inhibit sensory N activation: NS169. TRP receptor (vanilloid receptor); capsaicin activated specific ion channel of C-fiber :capsazepine , menthol. Chloride channel;Furosemide inhalation (cough with low Cl- solution, not with capsaicin induced cough) Tachykinin receptor antagonists; NK2 RA;SR Prostaglandin inhibitors; sulindac, aspirin. Neurotrophin inhibitors; NGF blocking Ab. Cannabinoid agonist: CP55940, JWH HT1A(serotonin) receptor agonists: methysergide. Theobromine;chocolate, cocoa inhibit capsaicin cough.")
21
만성기침은? 1. 2주 이상 지속되는 기침 2. 4주 이상 지속되는 기침 3. 8주 이상 지속되는 기침
4. 12주 이상 지속되는 기침 5. 16주 이상 지속되는 기침 6. 6개월 이상 지속되는 기침 7. 기침에 대한 초치료가 실패한 경우 3. 8주 이상 지속되는 기침

23
Chronic cough 동시에 여러 질환이 원인이 될 수 있다.
문진으로 얻을 수 있는 힌트는 원인 진단에 sensitive하지도 specific하지도 않다. 따라서 조직적으로 접근하는 것이 정확한 “진단 및 치료”의 기초이다.

24
Chronic cough Prevalence;11-20% US, Sweden, European study
In England 4003pts; 12% (7% severe) Smoking; 9.2%(C-S), 3.3% (N-S), 3.0%(Ex-S) PM10; reduction in peak flow, cough, sputum
 Smoking; 9.2%(C-S), 3.3% (N-S), 3.0%(Ex-S) PM10; reduction in peak flow, cough, sputum.")
26
ACE inhibitors: 일단 STOP!
기침 시작 전 1년 이내 투약을 시작하였다면 의심해 보아야 한다. 투약 전부터 기침이 있었더라도 의심의 눈초리를 거두면 안된다. – 다시 보자 ACEI! ACEI 중지 후 : 1-3주 사이 기침호전, 3개월까지도 지속가능 (median time 26일) 기침원인1=GERD 기침원인2=ACE ACEI
 기침원인1=GERD. 기침원인2=ACE. ACEI.")
27
ACE inhibitors ACEI 중지 후 증상 호전 ACE를 꼭 처방해야 하면 재투여 시도가능
Na cromoglycate(intal®), NSAID(sulidac, indomethacin), Aspirin, Theophylline, Amlodipine, Nifedipine, Ferrous sulfate, Picotamide, Baclofen
, NSAID(sulidac, indomethacin), Aspirin, Theophylline, Amlodipine, Nifedipine, Ferrous sulfate, Picotamide, Baclofen.")
28
Smoking : 일단 STOP! 금연 후 4주 이내 증상 호전 금연 4주 이후에도 지속되는 기침:
COPD 급성악화 vs. 중증 COPD vs. 안정적 COPD (다른 원인에 의한 만성기침이 동반된)
")
29
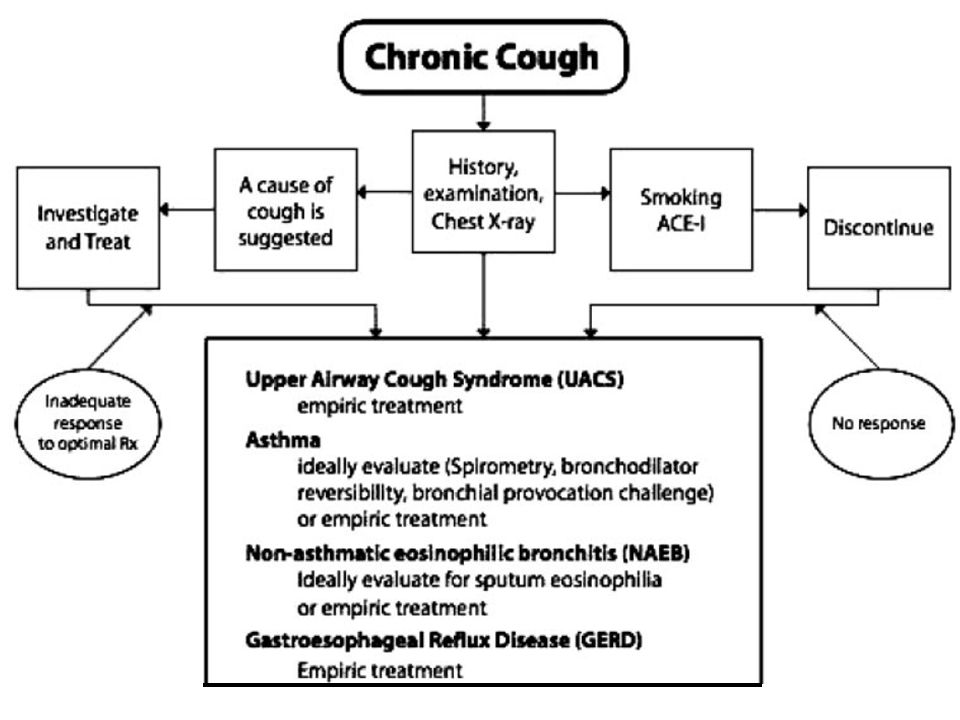
UACS(PNDS) Chronic Cough Smoking ACEI Chest PA stop
1st antihistamin + Decongestant UACS(PNDS) Metha Prov Test Asthma Non asthmatic eosinophilic bronchitis Induced sputum PPI GERD Bronchoscopy HRCT Specific Tx
 Metha Prov Test. Asthma. Non asthmatic eosinophilic bronchitis. Induced sputum. PPI. GERD. Bronchoscopy. HRCT. Specific Tx.")
30
UACS(upper airway cough syndrome)
M/C cause of chronic cough 1st G antihistamine (Ucerax, Avil, Primalan) + decongestant(pseudoephedrine) cf)PhenylPropAnolamine(콘택600®; 뇌출혈) 수일 ~ 1,2주 내 증상 호전: UACS로 진단 Nasal Sx: Nasal-ICS, Anticholinergic, Antihistamine 추가 Sinus imaging PNS CT vs PNS : air-fluid level, polyp Provaocation test
 + decongestant(pseudoephedrine) cf)PhenylPropAnolamine(콘택600®; 뇌출혈) 수일 ~ 1,2주 내 증상 호전: UACS로 진단. Nasal Sx: Nasal-ICS, Anticholinergic, Antihistamine 추가 Sinus imaging. PNS CT vs PNS : air-fluid level, polyp. Provaocation test.")
31
Asthma Chronic Cough Smoking ACEI Chest PA stop
1st antihistamin + Decongestant UACS Metha Prov Test Asthma Non asthmatic eosinophilic bronchitis Induced sputum PPI GERD Bronchoscopy HRCT Specific Tx

32
Cough Variant Asthma 문진: 알러지,비염, 가족력, 계절, 야간증상 등 힌트는 되나 천식을 rule in/rule out할 수 없다. Provocation test; NPV 100%, PPV 60~88% Positive result: Inhaled CS+BA Partial response 1주 내 Complete response 8주 까지 Oral steroid: 30-40mg/D 5~20일 (LTRA를 미리 써보기도) 1/3~1/2 full-blown asthma
 1/3~1/2 full-blown asthma.")
33
C.C. cough chronic 기류제한: (-) Aggravate at night Eosinophil: 13.5% IgE: 205IU MAST: (-)
 Aggravate at night Eosinophil: 13.5% IgE: 205IU MAST: (-)")
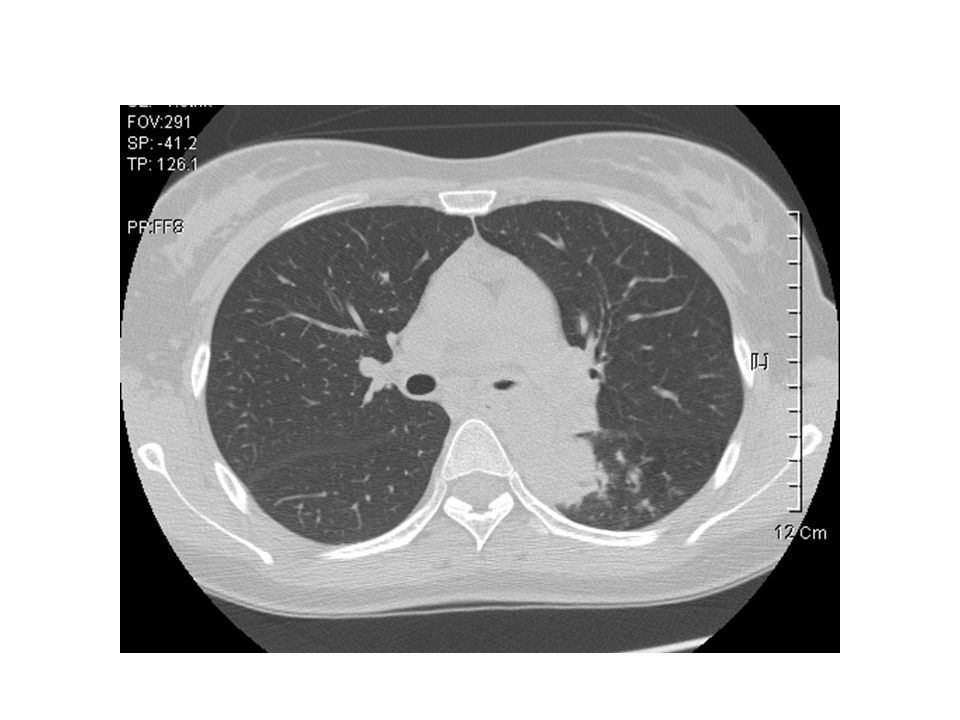
34
Cough variant asthma

35
Non Asthmatic Eosinophilic Bronchitis
Chronic Cough Smoking ACEI Chest PA stop 1st antihistamin + Decongestant UACS Metha Prov Test Asthma Non Asthmatic Eosinophilic Bronchitis Induced sputum PPI GERD Bronchoscopy HRCT Specific Tx

36
Non asthmatic eosinophilic bronchitis (NAEB)
Incidence: GERD >> NAEB Dx & Tx: 쉽고 명확 Sputum induction (3% NaCl): ICS로 치료: 4주 이내 대부분 호전 검사 불가능 시: ICS
: ICS로 치료: 4주 이내 대부분 호전. 검사 불가능 시: ICS.")
37
In this table the similarities and differences of asthma and eosinophilic bronchitis without asthma can be observed. The main difference is the absence of variable airflow limitation and airway hyperresponsiveness in eosinophilic bronchitis. The pathological findings are remarkably similar, with the exception of the presence of mast cell infiltration in asthma but not in eosinophilic bronchitis.

38
Observational study of the natural history of eosinophilic bronchitis
52 patients with EB, 32 with follow-up 1 year Mean duration of follow-up: 3.1 years (1-6 years) 3 patients developed asthma (9%) 5 patients FEV1/FVC (post-bd) <70% (16%) 1 complete resolution of cough & eosinophilia (3%) 13 persistent cough & eosinophilia >3% on one or more occasions (41%) 7 persistent cough & eosinophilia < 3% (22%) 3 Sx. free & eosinophilia >3% occasionally (9%) Berry MA et al. Clin Exp Allergy 2005
 3 patients developed asthma (9%) 5 patients FEV1/FVC (post-bd) <70% (16%) 1 complete resolution of cough & eosinophilia (3%) 13 persistent cough & eosinophilia >3% on one or more occasions (41%) 7 persistent cough & eosinophilia < 3% (22%) 3 Sx. free & eosinophilia >3% occasionally (9%) Berry MA et al. Clin Exp Allergy")
39
GERD Chronic Cough Smoking ACEI Chest PA stop
1st antihistamin + Decongestant UACS Metha Prov Test Asthma Non asthmatic eosinophilic bronchitis Induced sputum PPI GERD Bronchoscopy HRCT Specific Tx

40
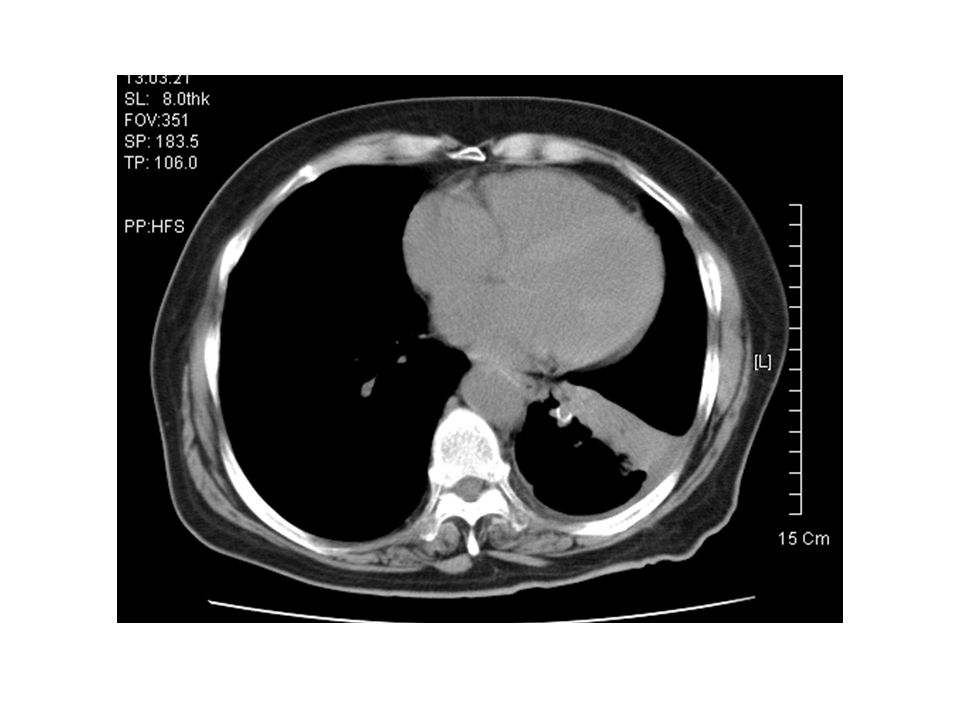
GERD(gastroesophageal reflux)
만성기침 중 UACS, asthma, NAEB가 아닌 환자의 92% GERD 따라서 검사보다는 먼저 치료 해보자! Antireflux diet:기자탄 금주쵸아 생활습관교정:체중감량, 수면 시 머리높임 PPI: 2주~6개월 Prokinetic Tx(?) 증상 계속 시: 24시간 식도 pH, 내시경
 증상 계속 시: 24시간 식도 pH, 내시경.")
41
Specific Tx Chronic Cough Smoking ACEI Chest PA stop
1st antihistamin + Decongestant UACS Metha Prov Test Asthma Non asthmatic eosinophilic bronchitis Induced sputum PPI GERD AFB Bronchoscopy HRCT Specific Tx

Similar presentations









>")





,>")
 BONUS.>")









 Diagnosis and management of chronic asthma in line with current BTS guidelines (Dr Lowery) 3 x Case.>")

