Download presentation
Presentation is loading. Please wait.

1
Case Review and Community Action Tools to Address Perinatal HIV Prevention in South Carolina Zakiya Grubbs, MPH Public Health Associate Office for State, Tribal, Local and Territorial Support Centers for Disease Control and Prevention PHAP Spring Training April 4, 2016 Centers for Disease Control and Prevention Office for State, Tribal, Local and Territorial Support

2
http://www.asylumprojects.org/index.php?title=South_Carolina_State_Hospital_Image_Gallery From Miami, FL Host site: South Carolina Department of Health and Environmental Control (DHEC), Division of STD/HIV in Columbia, SC Year 1 & 2 assignments: HIV/AIDS About Me
, Division of STD/HIV in Columbia, SC Year 1 & 2 assignments: HIV/AIDS About Me")
3
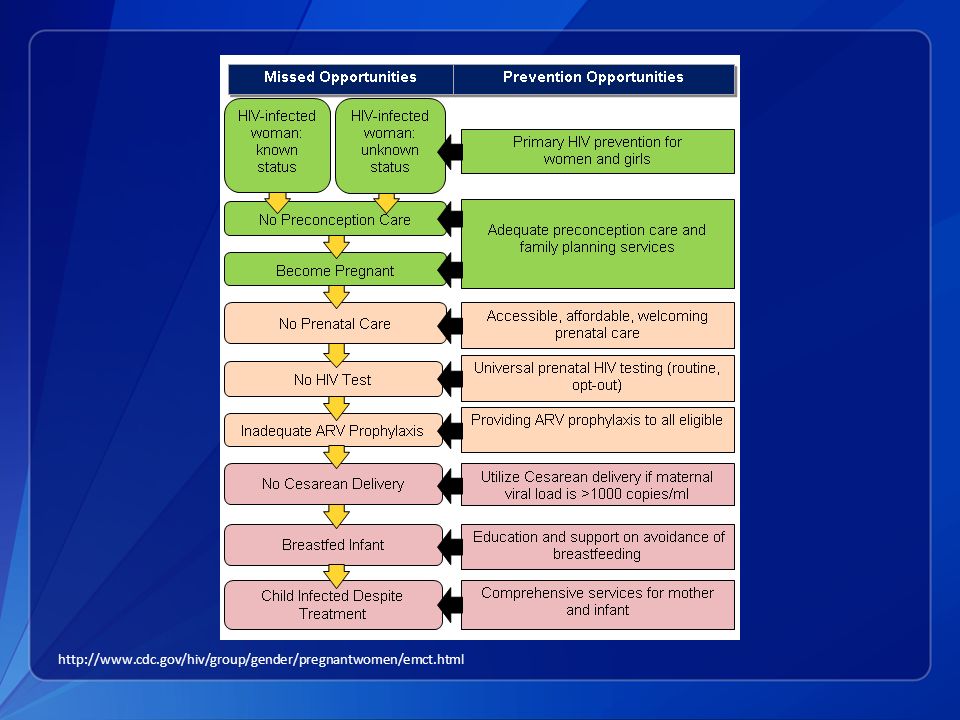
Perinatal HIV Transmission of HIV infection from a mother to child is the most common mode of infection in children and a largely preventable occurrence. When the proper precautions are taken during pregnancy, delivery, and after birth, the rate of transmission can fall below 1%. If no precautions are taken, the rate of transmission is about 25%. http://www.cdc.gov/hiv/group/gender/pregnantwomen/index.html http://sfghf.org/funded-initiatives/preventing-perinatial-hiv /

4
http://www.cdc.gov/hiv/group/gender/pregnantwomen/emct.html
5
Fetal Infant Mortality Review/HIV (FIMR/HIV) Prevention methodology for perinatal HIV transmission To identify and address missed opportunities for prevention Process leads to changes in perinatal and HIV care systems for all women Since 2008, sites have used FIMR/HIV to: Legislate opt-out 3 rd trimester HIV testing Increase integration of MCH and HIV services National Resource Center: http://fimrhiv.org/ http://www.fimrhiv.org/
 Prevention methodology for perinatal HIV transmission To identify and address missed opportunities for prevention Process leads to changes in perinatal and HIV care systems for all women Since 2008, sites have used FIMR/HIV to: Legislate opt-out 3 rd trimester HIV testing Increase integration of MCH and HIV services National Resource Center:")
6
FIMR/HIV Prevention Methodology

7
FIMR/HIV in South Carolina Goal: Improve perinatal HIV prevention services and outcomes Objectives: Identify cases of perinatal HIV exposure and create case reports from medical records and maternal interviews Assemble a multi-disciplinary team to review cases and propose recommendations to improve HIV services and interventions Use community mobilization to enact changes based on committee recommendations

8
Case Identification Focus on HIV exposed infants from across the state with greater than 24 weeks gestation and less than 24 months of age at the time of the review Case Priority Any cases of HIV infection When was the mother diagnosed with HIV? Did the mother receive adequate prenatal care? Did the mother receive HIV treatment during delivery? Other factors: poverty, homelessness, substance abuse, mental health

9
Medical Record Abstraction & Maternal Interview Medical records are collected by the area surveillance coordinators (ASCs) for data abstraction. Records include: Maternal HIV carePrenatal care Labor and deliveryPostpartum care Newborn/pediatric care records Maternal interview is conducted by DHEC HIV social workers Mother’s perspective of her pregnancy and delivery process Adds information that is not captured in the medical records

10
Case Review Team (CRT) Multidisciplinary team reviews 3 to 5 cases every quarter and creates recommendations for systems change Guiding questions during review: Did the pregnant woman with HIV infection and her newborn receive the services or community resources they needed? Were the systems and services culturally and linguistically appropriate? Are there gaps in the system? Are there specific missed opportunities for HIV prevention, treatment or follow-up? What can this case tell us about how families are able to access the existing local services resources?

11
Community Action Team (CAT) The Community Action Team uses CRT recommendations to create and implement a plan of action Members include “those with the political will and resources to create large-scale systems change, and members who have an accurate community perspective on how best to create the desired change in the community.” http://www.fimrhiv.org/
 The Community Action Team uses CRT recommendations to create and implement a plan of action Members include those with the political will and resources to create large-scale systems change, and members who have an accurate community perspective on how best to create the desired change in the community.")
12
Case review team Two meetings held (5 cases reviewed, 4 with interviews) Issues/needs identified in case review Low income/ limited education HIV diagnosis during pregnancy Missed opportunities for HIV testing (mother and infant) Infrequent health care usage (before and during pregnancy) Problems with infant formula No preconception counseling Rural location Limited transportation access Infant lost to follow-up Depression/mental health Need for peer/social support Early childhood trauma Sexual assault Inadequate prenatal care Obesity and other health issues Program Implementation
 Issues/needs identified in case review Low income/ limited education HIV diagnosis during pregnancy Missed opportunities for HIV testing (mother and infant) Infrequent health care usage (before and during pregnancy) Problems with infant formula No preconception counseling Rural location Limited transportation access Infant lost to follow-up Depression/mental health Need for peer/social support Early childhood trauma Sexual assault Inadequate prenatal care Obesity and other health issues Program Implementation")
13
CRT Recommendations Intensive Case Management Referrals to social services Education/work support Continuing case management one year after pregnancy Mental health counseling Using trauma informed care approach Nutrition Education WIC services for HIV positive mothers Pre-mastication education Promotion of Milk Bank for HIV exposed infants Mother’s nutrition and weight management

14
CRT Recommendations (continued) Peer Advocacy and Social Support Centering during HIV care visits HIV support services aimed at women (especially for issues surrounding pregnancy) Creation of a referral card of all HIV/health/social services available to women living with HIV Evaluate DHEC HIV Reporting Policies Exposed baby protocols for referrals to nurses, social workers, or partner services Standardized policies across the state for HIV testing of exposed infants Outreach to providers on protocols
 Peer Advocacy and Social Support Centering during HIV care visits HIV support services aimed at women (especially for issues surrounding pregnancy) Creation of a referral card of all HIV/health/social services available to women living with HIV Evaluate DHEC HIV Reporting Policies Exposed baby protocols for referrals to nurses, social workers, or partner services Standardized policies across the state for HIV testing of exposed infants Outreach to providers on protocols")
15
CRT Recommendations (cont.) Provider Education Preconception counseling, birth control and LARCs Training for traditionally non-HIV care providers on providing HIV care Hotline for providers to receive assistance on HIV care Training on domestic and sexual violence Using a trauma informed care approach Universal HIV testing (normalizing testing as a standard part of care) Outreach to rural providers and facilities (especially those that may not have experience in care/delivery of an HIV exposed infant)
 Provider Education Preconception counseling, birth control and LARCs Training for traditionally non-HIV care providers on providing HIV care Hotline for providers to receive assistance on HIV care Training on domestic and sexual violence Using a trauma informed care approach Universal HIV testing (normalizing testing as a standard part of care) Outreach to rural providers and facilities (especially those that may not have experience in care/delivery of an HIV exposed infant)")
16
Next Steps Program Implementation Begin implementing changes recommended by CRT Committees for each of the five recommendation areas Develop strategic partnerships with local agencies and the community Consider congenital syphilis reviews Program Evaluation Process and outcome evaluation Annual review of program activities https://dph.georgia.gov/TitleV

17
For more information, please contact CDC’s Office for State, Tribal, Local and Territorial Support 4770 Buford Highway NE, Mailstop E-70, Atlanta, GA 30341 Telephone: 1-800-CDC-INFO (232-4636)/TTY: 1-888-232-6348 E-mail: OSTLTSfeedback@cdc.govWeb: http://www.cdc.gov/stltpublichealthOSTLTSfeedback@cdc.govhttp://www.cdc.gov/stltpublichealth The findings and conclusions in this presentation are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention. Questions? Zakiya Grubbs, MPH 803-898-0365 ypl8@cdc.govypl8@cdc.gov | grubbsz@dhec.sc.govgrubbsz@dhec.sc.gov Centers for Disease Control and Prevention Office for State, Tribal, Local and Territorial Support

Similar presentations







: What Will it Take to Eliminate MTCT? Jessica Rodrigues Presentation for UNICEF Written.>")







>")



