Download presentation
Presentation is loading. Please wait.

1
U.RADHAKRISHNAN.M.P.T.(ORTHOPAEDICS)
BIOMECHANICS OF HIP JOINT U.RADHAKRISHNAN.M.P.T.(ORTHOPAEDICS)
")
2
INTRODUCTION TYPE SYNOVIAL JOINT VARIETY BALL & SOCKET JOINT
THE MAJOR FUNCTION OF HIP JOINT IS STABILITY IT SUPPORTS THE BODY WEIGHT TRANSMIT FORCES FROM PELVIS TO LEGS AND FROM LEGS TO PELVIS

3
HIP JOINT

4
ARTICULATION Cup like concave structure on the hip bone called ACETABULUM ,articulates with a spherical shaped HEAD OF FEMUR The acetabulum is deepened by peripheral ring called as ACETABULUM LABRUM.It helps to hold the head of Femur in the socket

5
ANGLE OF INCLINATION IN FRONTAL PLANE
The axis of Femoral neck and Femoral shaft forms an angle Normal angle is 120 degree Increase in the angle is called COXA VALGA Decrease in the angle is called COXA VARA

6
ANGLE OF INCLINATION

7
ANGLE OF TORSION In TRANSVERSE PLANE:
The angle formed by the head and neck of femur with the axis of Femoral condyles Normal angle is 8-25 degrees The increase in the Angle of Torsion is called as ANTEVERSION The decrease in the Angle of Torsion is called as RETROVERSION

8
ANGLE OF TORSION

9
TORSION ANGLE

10
TRABECULAR SYSTEM The Trabecular lines of stress found in Femur and Pelvis to meet the stress requirements 1.Medial Trabecular system 2.Lateral Trabecular system 3.Medial accessory system 4.Lateral accessory system

11
MEDIAL TRABECULAR SYSTEM
It arises from Medial cortex to upper Femoral shaft and radiates outwards to cortical bone of superior aspect of Femoral head. It helps to resist the Joint reaction forces during Single Limb Support.

12
LATERAL TRABECULAR SYSTEM
It arises from Lateral cortex of Upper Femoral Shaft after crossing the Medial system and end on Inferior aspect of head of Femur. It is developed in response to force created by contraction of abductor Muscle

13
ACESSORY SYSTEM Medial Accessory system crosses lateral and fans out into region of Greater Trochanter Lateral Accessory system runs parallel to Greater Trochanter. The areas where the Trabecular system cross each other in right angles are areas of strength

14
ZONE OF WEAKNESS The areas where Trabeculae does not cross at Right angles are area of Weakness The Zone of Weakness is the Femoral neck

15
ZONE OF WEAKNESS

16
JOINT CAPSULE The articular capsule of Hip is very strong and dense
The capsule extends the periphery of acetabulum to Femoral neck The anterior capsule is stronger than the Posterior capsule because of two ligaments

17
JOINT CAPSULE

18
ANTERIOR LIGAMENTS ILIO FEMORAL LIGAMENT---Strongest ligament of hip,Y shaped attached to ASIS and INTERTROCHANTERIC LINE. It checks HIP HYPEREXTENSION PUBO FEMORAL LIGAMENT--- it arises from anterior aspect of Pubic ramus and passess to anterior surface of Intertrochanteric fossa It checks Hip Abduction and Extension

19
ANTERIOR LIGAMENTS

20
POSTERIOR LIGAMENT ISCHIO FEMORAL LIGAMENT
Attached to posterior surface of Acetabulum Labrum to Femoral neck and inner surface of Greater Trochanter Checks Hip Hyperextension

21
ISCHIO FEMORAL LIGAMENT

22
MOVEMENTS OF HIP JOINT THREE DEGREE OF FREEDOM FLEXION –EXTENSION
Saggital plane----Medio lateral axis ABDUCTION-ADDUCTION Coronal plane Anterio Posterio axis MEDIAL LATERAL ROTATION Transverse plane---- Vertical axis

23
MUSCLES FLEXORS: Ilio Psoas , Pectenius, Tensor fasciae lata,Rectus femoris, Sartorius EXTENSORS: Gluteus Maximus Posterior fibers of Gluteus Medius,Piriformis TWO JOINT EXTENSORS: Long head of BICEPS,Semimembranosus, Semitendosus

24
ADDUCTORS Adductor Magnus Adductor Longus Adductor Brevis
The Adductors are stronger than the Abductors.

25
ABDUCTORS Gluteus Medius is a powerful Abductor
The Abductors able to generate maximum Isometric Torque in the Supine position when they are in Lengthened position

26
MEDIAL ROTAT & LATERAL ROTATOR
Gluteus Medius, Gluteus Minimus, they have fibers lie anterior to axis of motion of Hip and are Medial Rotators Adductor Longus and Magnus are also active in Medial Rotation LATERAL ROTATORS, Obturator internus & externus ,Piriformis,Gemellus

27
MOTION OF PELVIS Anterior –Posterior Pelvic tilting Saggital plane Lateral pelvic tilting coronal plane Pelvic rotation Transverse plane

28
ANTERIOR TILTING Anterior pelvic tilting causes Symphysis pubis to move inferiorly, anterior surface of pelvis moves closer to anterior surface of Femur Causes Hyper extension of Lumbar spine Increase the Lumbar anterior convexity Hip Flexors work with Trunk Extensors as a force couple

29
ANTERIOR TILT

30
POSTERIOR TILT Posterior tilting brings the posterior aspect of pelvis closer to posterior surface of Femur It causes Flexion of Lumbar spine It decreases the Lumbar anterior convexity Hip extensors works with Trunk flexors as a force couple to produce Posterior tilting

31
POSTERIOR TILT

32
LUMBAR PELVIC RHYTHM It refers to specific type of coordinated activity in which anterior pelvic tilting occurs with flexion of Lumbar spine and posterior tilt occurs with Extension of Lumbar Spine It helps to gain more range of motion during trunk bending

33
LUMBAR PELVIC RHYTHM

34
LATERAL TILT Pelvis tilt Inferiorly or Superiorly
It causes lateral flexion and rotation of spine and abduction or adduction of Hip. Hip Hiking is produced by Quadratus Lumborum muscle Pelvic drop is controlled by Gluteus Medius of opposite side Excessive tilting due to Abductor weakness is called TRENDELENBURG SIGN

35
LATERAL TILT & ROTATION OF PELVIS

36
PELVIC ROTATION Forward and Backward rotation of Pelvis
If the right side pelvis is forwardly rotating on the side of Swinging extremity,left hip serves as a axis for motion Lateral rotation takes place in right hip due to posterior movement of Right acetabulum over Right head of Femur

37
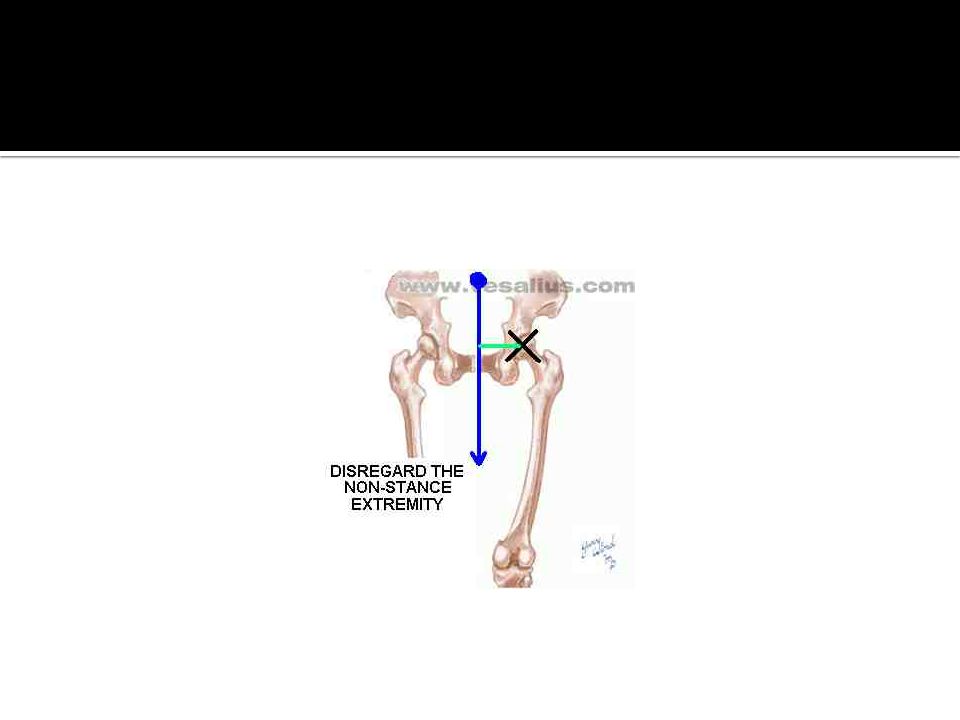
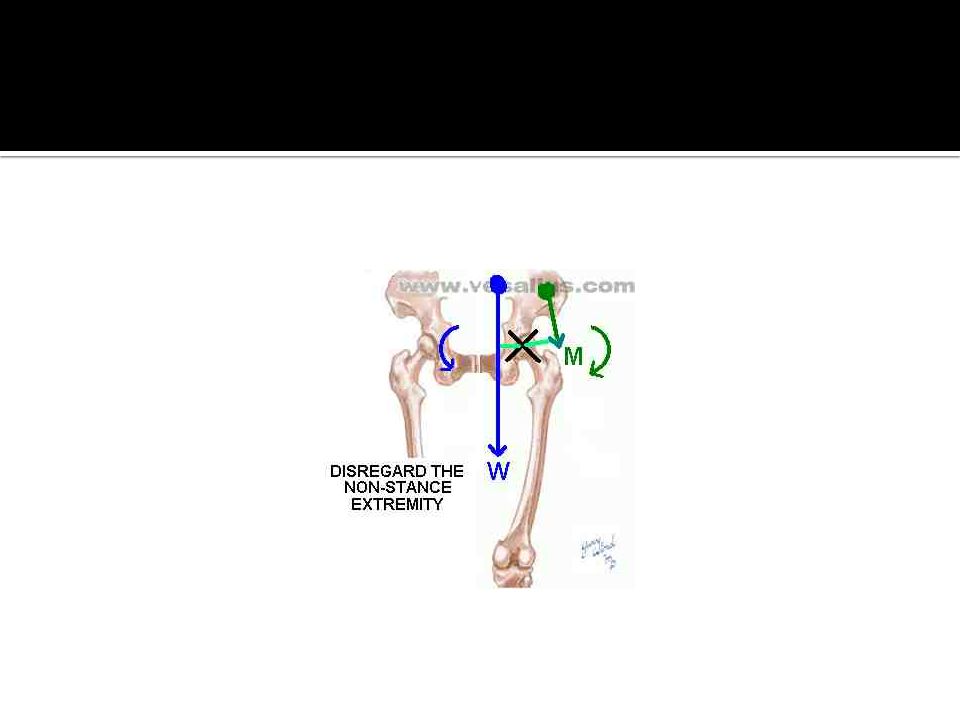
Gravity's effect on hip joint movement unilateral stance (frontal plane)
This figure provides a posterior view of the pelvis, might have of a person as he or she walks and bears weight momentarily on the right lower limb.

38
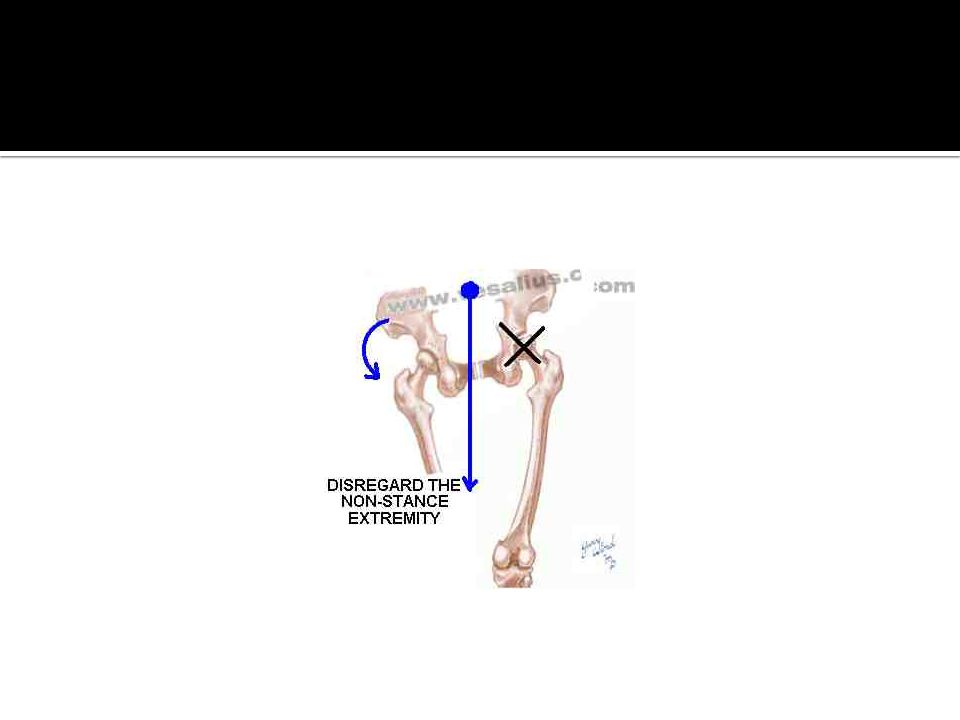
Because the stance phase of walking occurs in a closed kinetic chain, we analyze right (stance) hip movement by considering the mass superincumbent to the joint as the moving part. By placing the gravity vector on the approximate center of gravity of the moving part, we determine that its force, the weight of the mass superincumbent to the hip joint, produces adduction of the right hip.

41
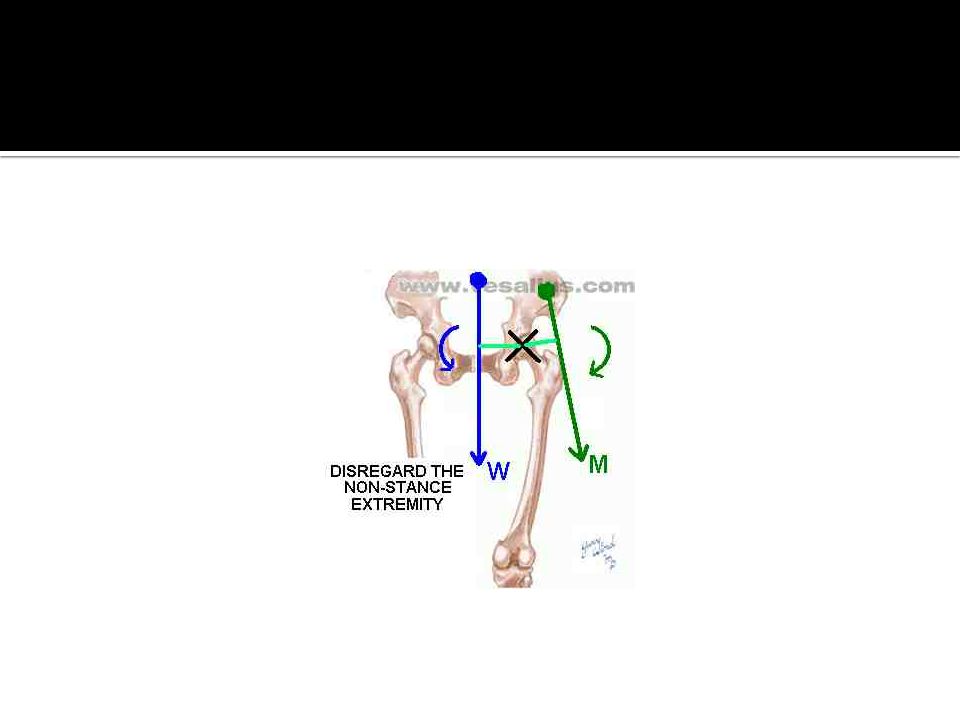
When people walk, their pelvises don't drop dramatically on the non-stance side because gravity's adductor moment is balanced by an equal and opposite abductor moment. "A major function of the hip abductors is in closed-chain motion to maintain a level pelvis in unilateral stance" (Smith, Weiss, & Lehmkuhl, 1996, p.294)
.")
43
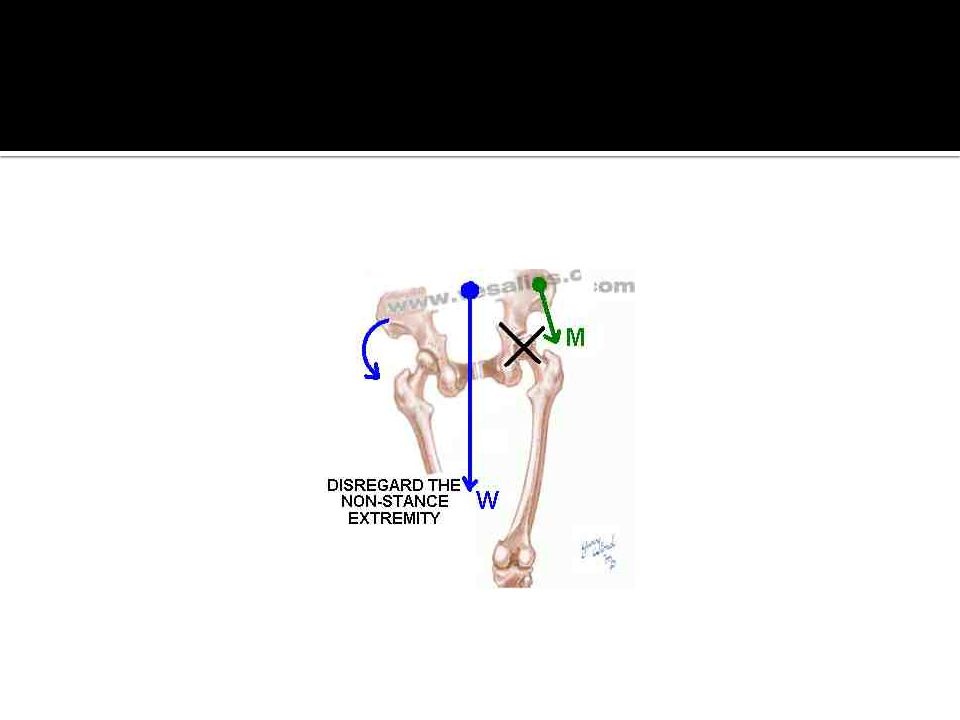
Compensation for muscle weakness
Because hip abductor activity is necessary to stabilize the hip in the frontal plane during unilateral stance, including the stance phase of walking, people with hip abductor weakness (note the relatively short vector M in the figure below) have a problem.
 have a problem.")
44
Trendelenburg’s sign We might see the pelvis drop on the unsupported side if we ask a person to stand briefly on the limb whose hip abductors are weak. The, inability to maintain a level pelvis in unilateral stance is called a positive Trendelenburg sign.

46
The most direct way to reorient the line of application of the gravity vector (note how vector W has shifted to the right), and so to shorten its moment arm with respect to the hip joint, is to lean the trunk toward the side of the hip whose abductor muscles are weak. This characteristic way of walking, in which the person leans laterally during stance, is sometimes called a Trendelenburg gait pattern or a gluteus medius limp

48
REDUCTION OF FORCES IN HIP JOINT
WEIGHT SHIFTING: When body weight is shifted totally to supporting leg then the resultant force acting on the Femur is reduced (If the line of gravity is shifted directly to the axis of Hip joint then the clock wise gravitational moment is eliminated and need for abductor muscle activity is reduced)
")
49
REDUCTION OF FORCES IN HIP JOINT
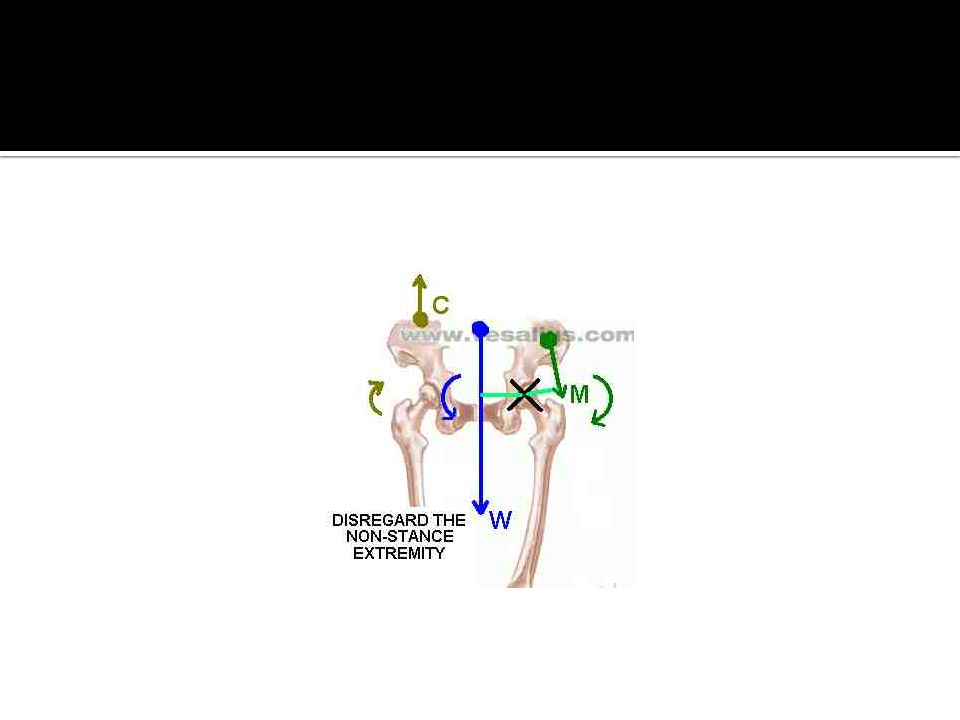
USE OF CANE: To reduce the force acting at the supporting hip is by use of cane on unsupported side of pelvis The gravitational moment acting at the Right hip tends to produce a drop of pelvis on Left unsupported side. The ground reaction force created as a result of downward thrust of body weight on cane will counterbalance moment in opposite direction.

50
The secret in using an assistive device, like a cane, is to create an additional force that keeps the pelvis level in the face of gravity's tendency to adduct the hip during unilateral stance. The cane's force must substitute for the hip abductors. A force that levels the pelvis efficiently, because its moment arm is relatively long, is directed upward from a point of application on the pelvis (vector C). The force originates on the side opposite the hip whose abductor muscles (vector M) are weak .
. The force originates on the side opposite the hip whose abductor muscles (vector M) are weak .")
52
To produce a force like vector C with a cane, one must push the cane firmly into the ground in a vertical direction. Doing so generates an upward reaction force (vector R) whose magnitude equals the downward force one exerts on the cane. Additionally, the person needs adequate strength in the muscles of the wrist, elbow, shoulder girdle, and trunk, whose effect is symbolized by the dashed line that connects vectors R and C. If not, he or she cannot efficiently transfer the cane's vertical reaction force (vector R) to the top of the pelvis (vector C) where it is needed.
 to the top of the pelvis (vector C) where it is needed.")
53
USE OF CANE – IN UNAFFECTED SIDE

54
PROBLEMS OF HIP COXA VARA,COXA VALGA ANTEVERSION ,RETROVERSION
ANTEVERSION causes anterior dislocation of Head of Femur ,intoeing, RETROVERSION causes Lateral rotation gives more stability to Hipjoint Fracture Neck Of FEMUR

Similar presentations
 by Susan J. Hall, Ph.D.>")


















