Download presentation
Presentation is loading. Please wait.

1
Fluorescene Angiogram Conference Russell Swan 3-25-2015

2
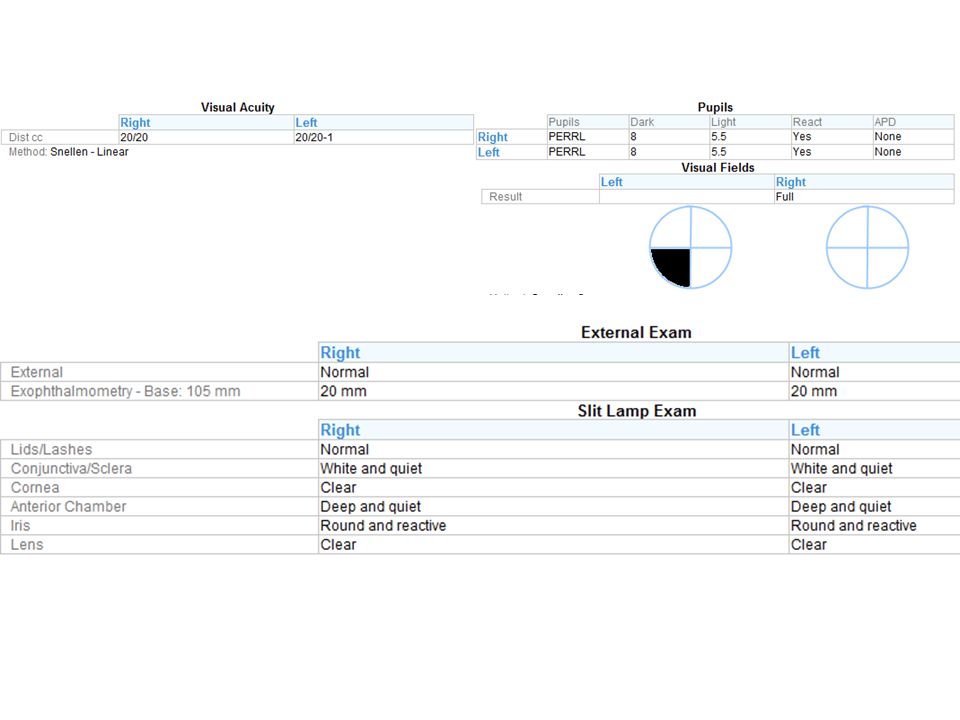
History CC: Blurry vision OS for ~1 week HPI: 27 year old female with ~ 1 week of vision changes in the left eye. Poor historian 2/2 difficulties with cognition – Per mom, mid December 2 weeks of recurrent dizziness and increased confusion. Seen OSH with normal head CT and treated for migraines – 12-25-14: developed nausea, vomiting, HA, and worsening dizziness; – 1-3-15: seen again at OSH ER; not oriented to date, not able to perform ADL’s or take care of children – 1-5-15: Admitted OSH: oriented to person only transferred to U of U for further care and eval

3
History Cont. PMH: – PFO – Hypothyroid – Migraines – Depression – HLD – GERD – Gestational DM and HTN during 2 nd pregnancy

4
History Cont. PSH: – Right ankle surgery x2 – Cyst removal from chin FH: – Brother with epilepsy 2/2 hypoxic brain injury as a child – No eye problems SH: – Divorced, 2 children

5
History Cont. Meds: – Lipitor – Klonipin – Prilosec – Metformin – Topamax – Levothyroxine – Imitrex prn – Mirena IUD – Vortioxetine

19
What does she have? Differential Ddx? Other testing? Recommendations to primary team?

20
Differential: Vasculitis, Churg Strauss, SLE, Sarcoid, Behcets, Eales, Lyme, Syphillis, TB, viral encehpalitis, primary CNS lymphoma, MELAS, isolated BRAO

21
MRI: multiple subcortical lesions in multiple vascular territories (most noticable in corpus collosum), leptomeningeal enhancement Doppler US of legs: no DVT TEE: no vegetation, right to left PFO LDL: 102 CTA: normal without stenosis Cerebral angiogram: no stenosis or vasculitis Labs: nl CBC, CMP, negative cardiolipi ab, normal CRP, A1C, lupus anticoagulant, Factor V, Protein C/S, antithrombin III, homocysteine, ACE, ANCA, SSA/SSB, ANA, Rf, ESR LP: unremarkable
, leptomeningeal enhancement Doppler US of legs: no DVT TEE: no vegetation, right to left PFO LDL: 102 CTA: normal without stenosis Cerebral angiogram: no stenosis or vasculitis Labs: nl CBC, CMP, negative cardiolipi ab, normal CRP, A1C, lupus anticoagulant, Factor V, Protein C/S, antithrombin III, homocysteine, ACE, ANCA, SSA/SSB, ANA, Rf, ESR LP: unremarkable")
22
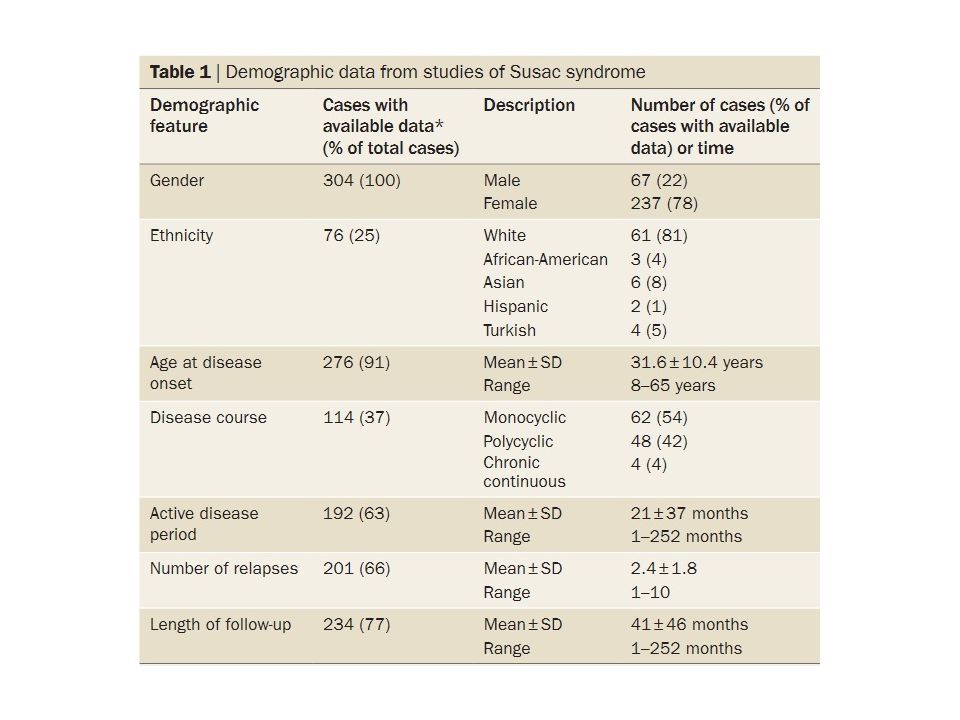
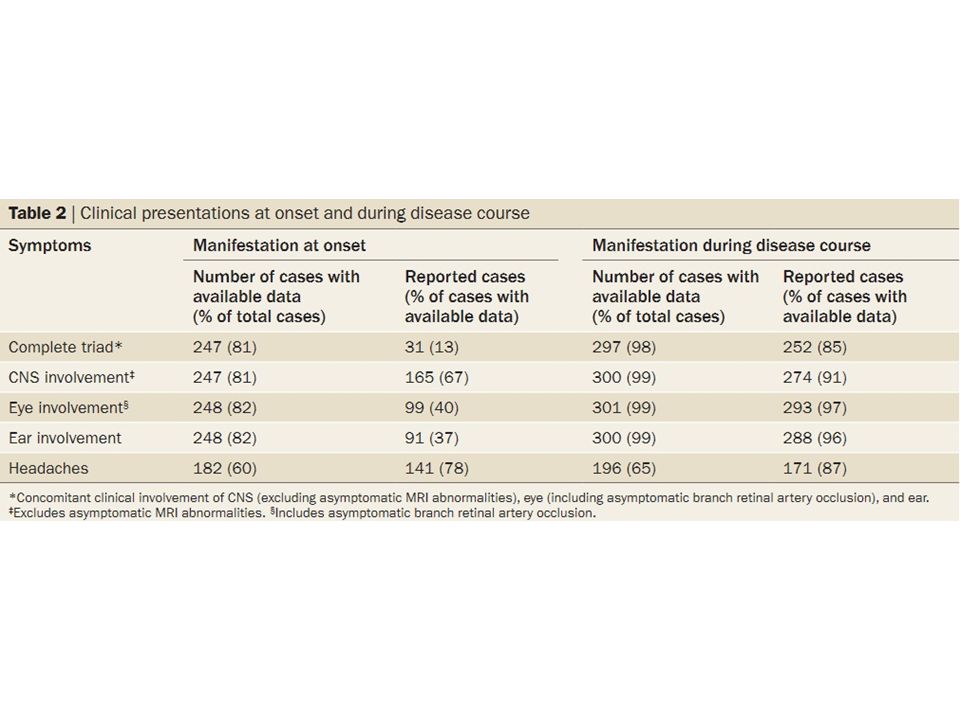
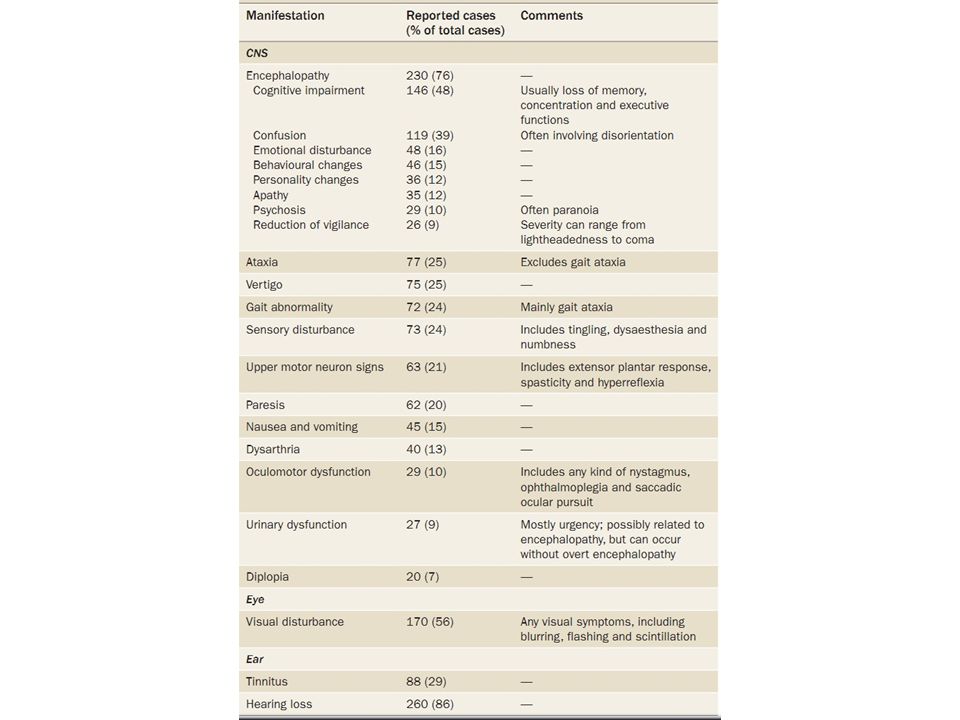
Susac Syndrome Autoimmune disease first described in 1979 by Dr John Susac Epidemiology: Most often affects females between the ages of 20 to 40; 3:1 F:M; ages 8-58 Classic Symptoms: – Brain HA with associated vomiting Confusion, cognitive difficulties Change in personality and psychiatric problems – Eye: Visual field changes – Ear: Hearing loss Vertigo Tinnitus

26
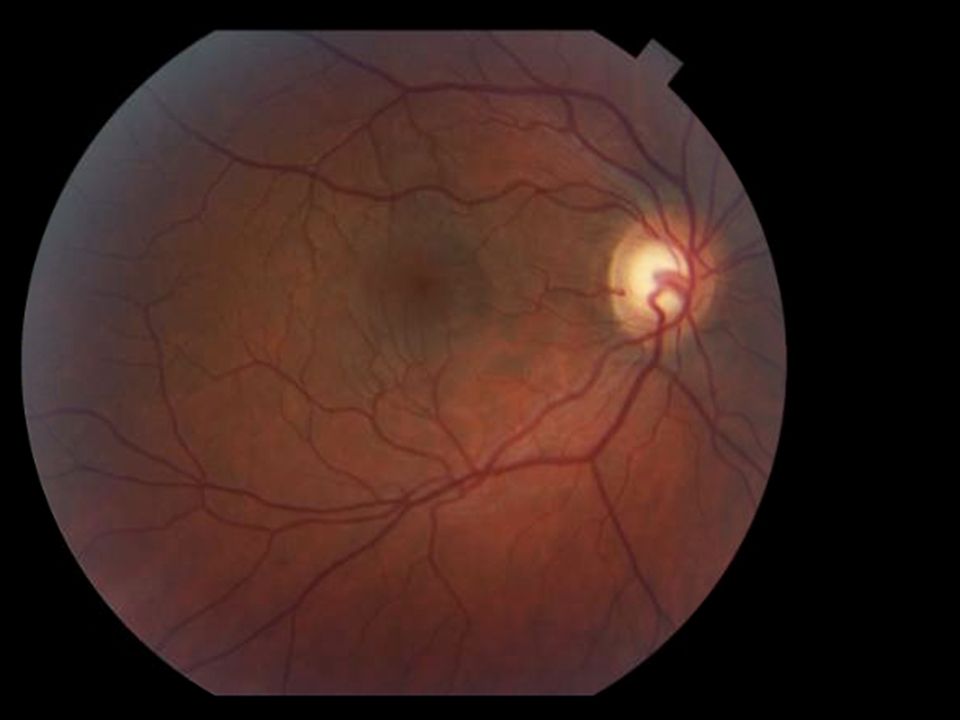
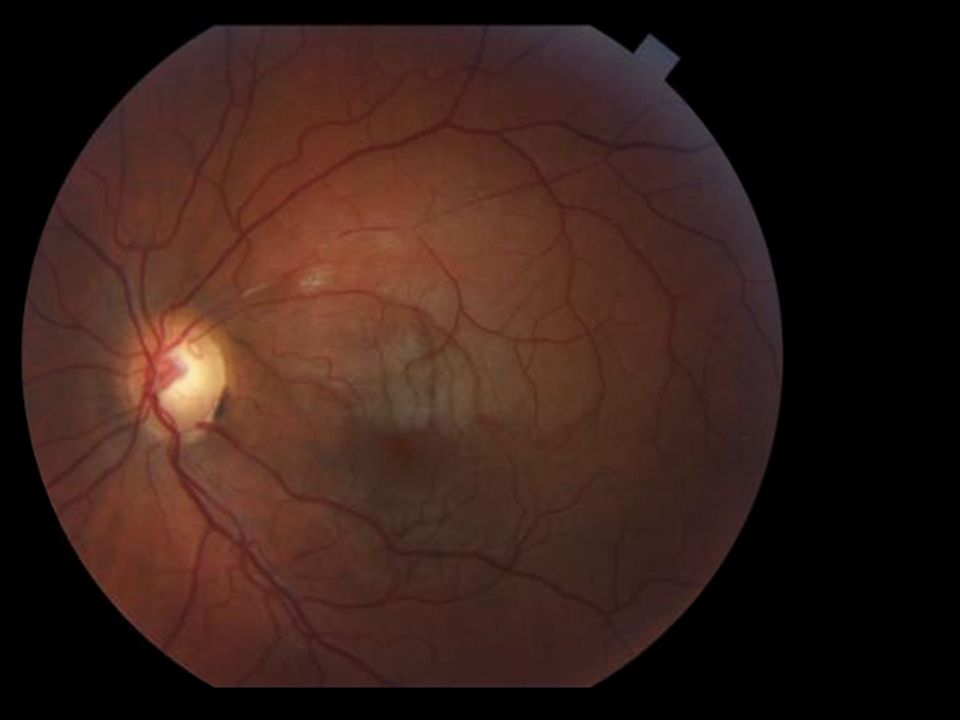
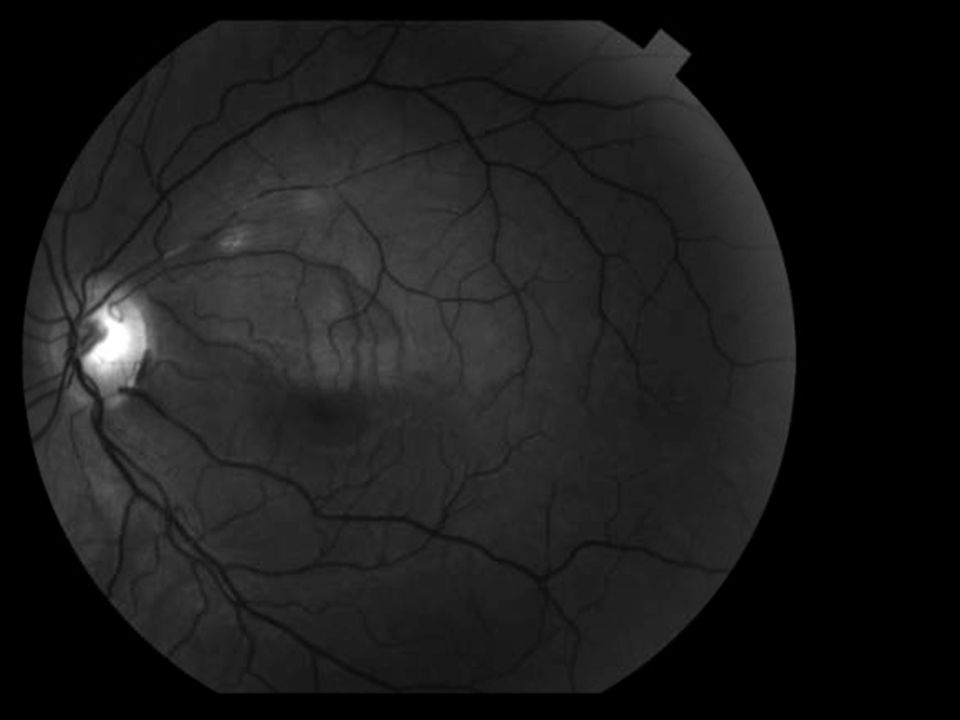
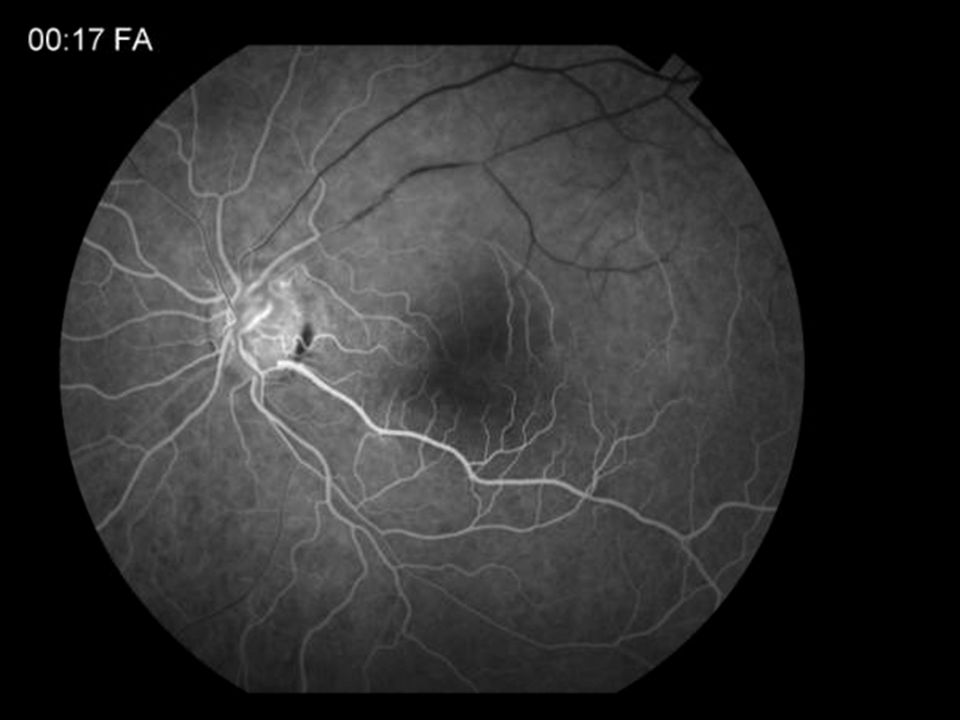
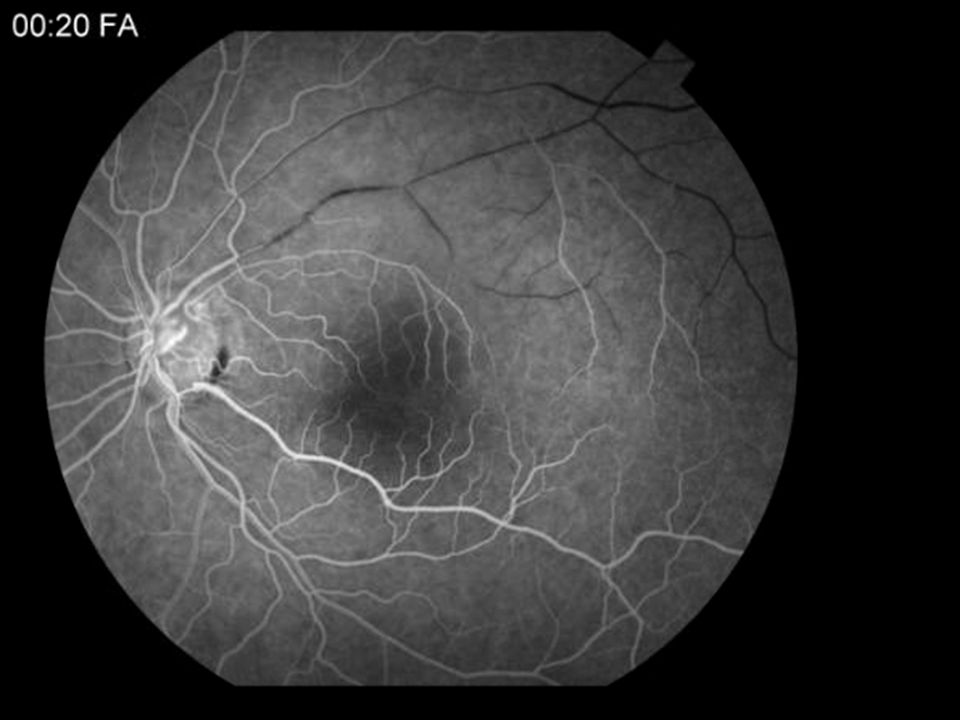
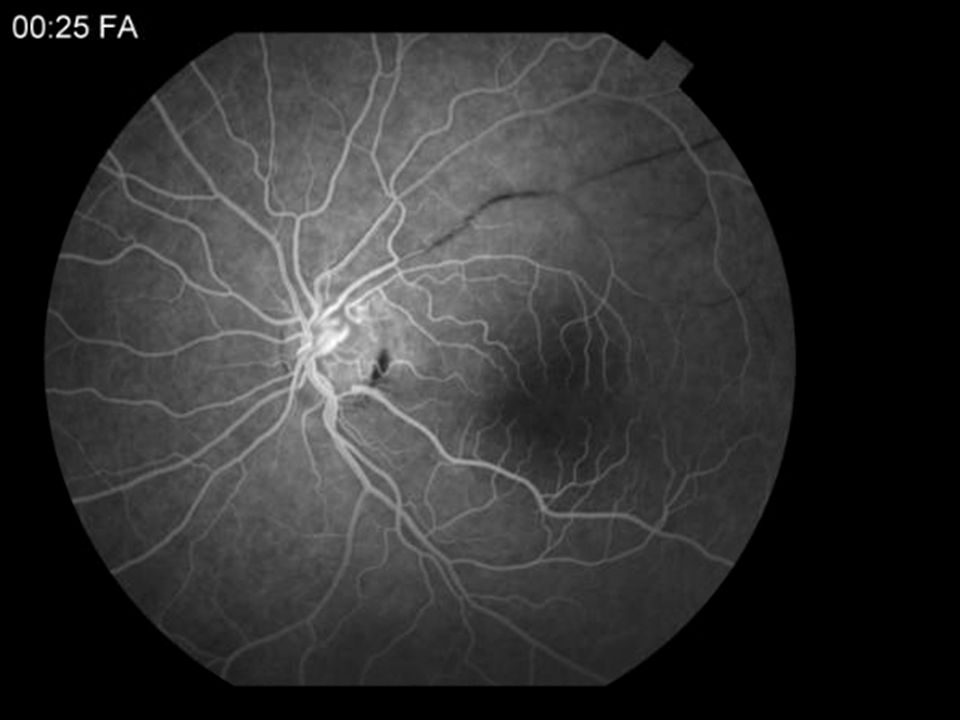
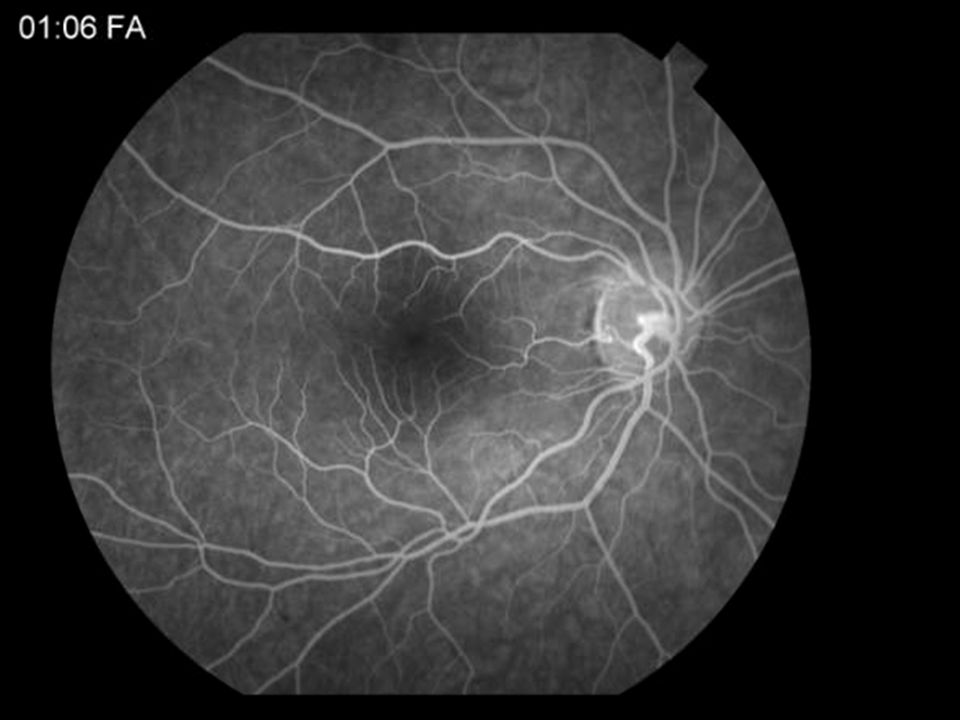
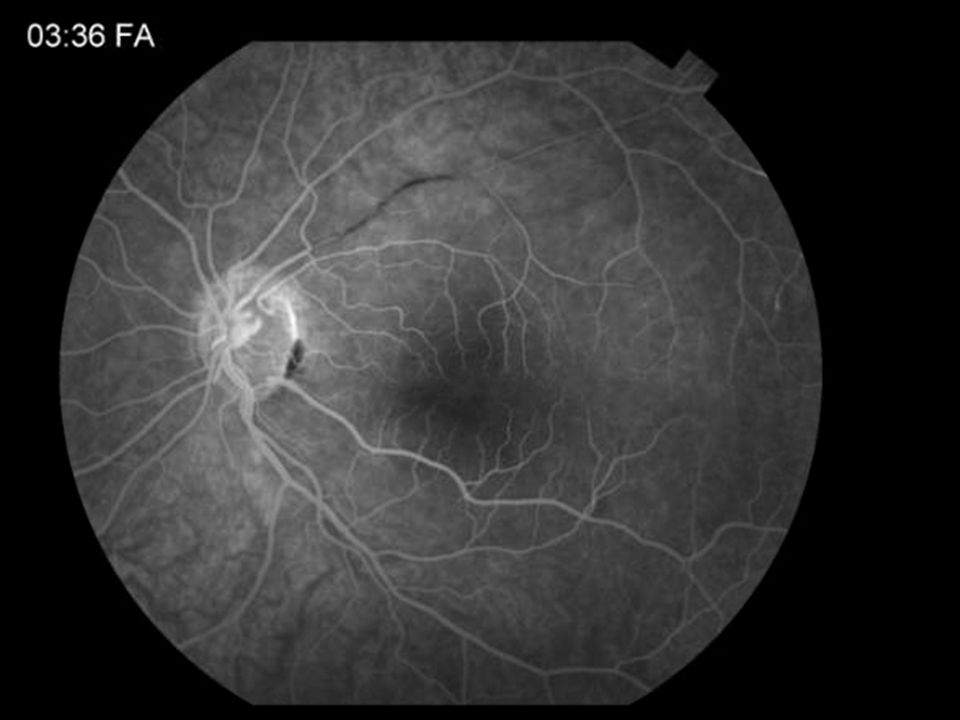
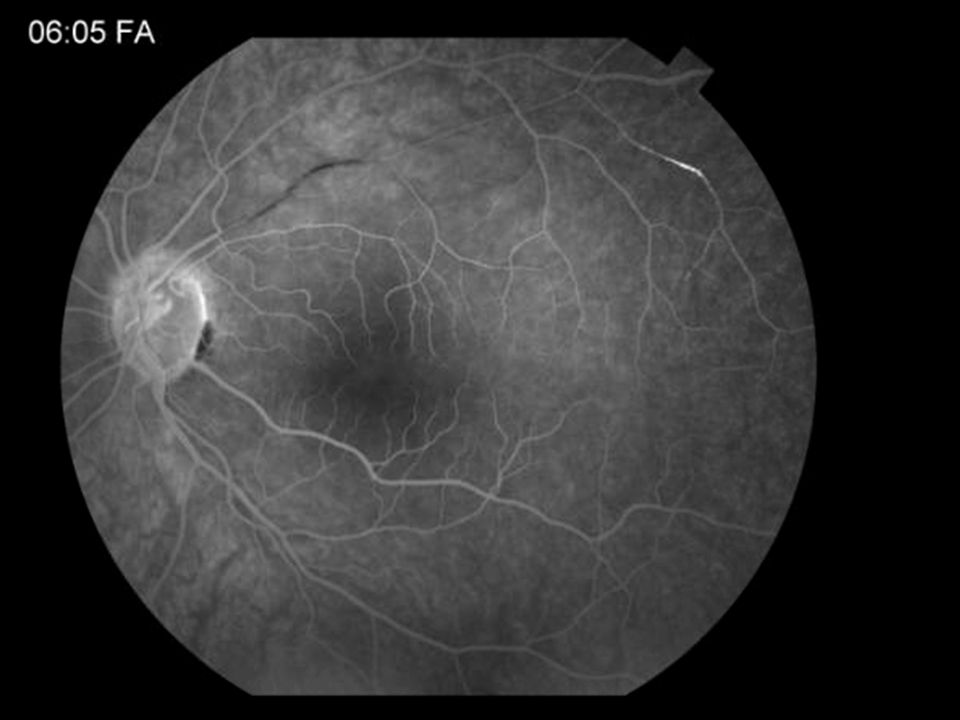
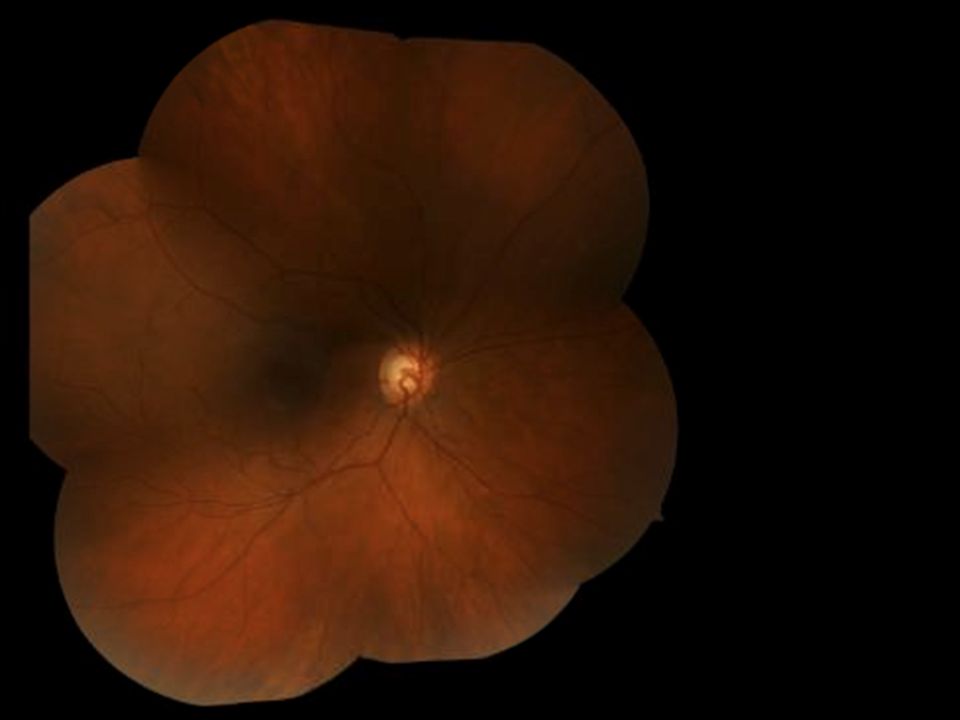
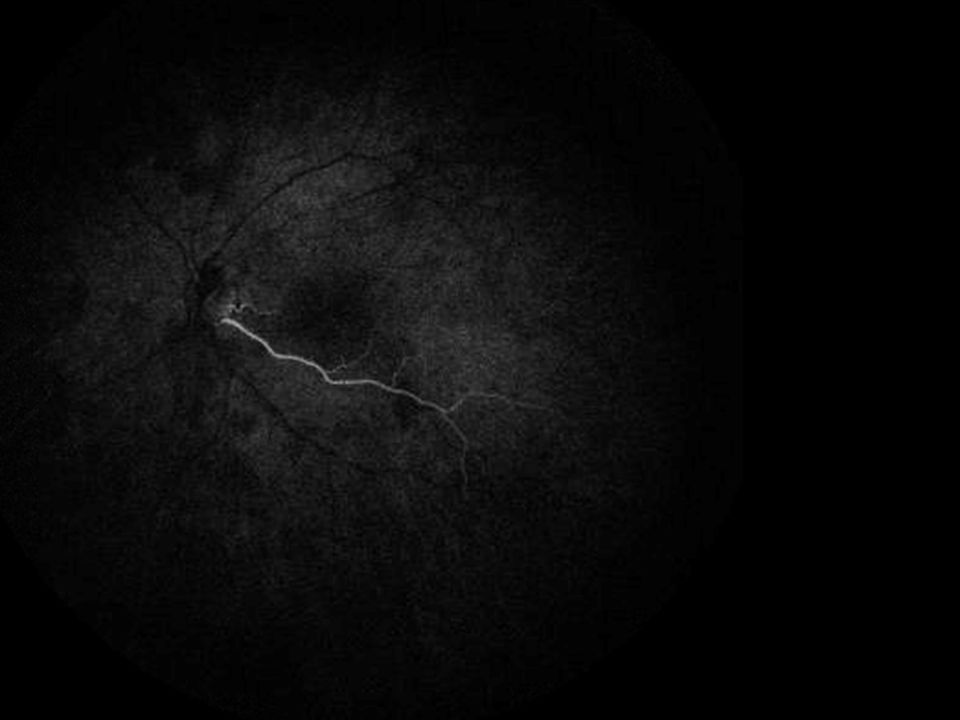
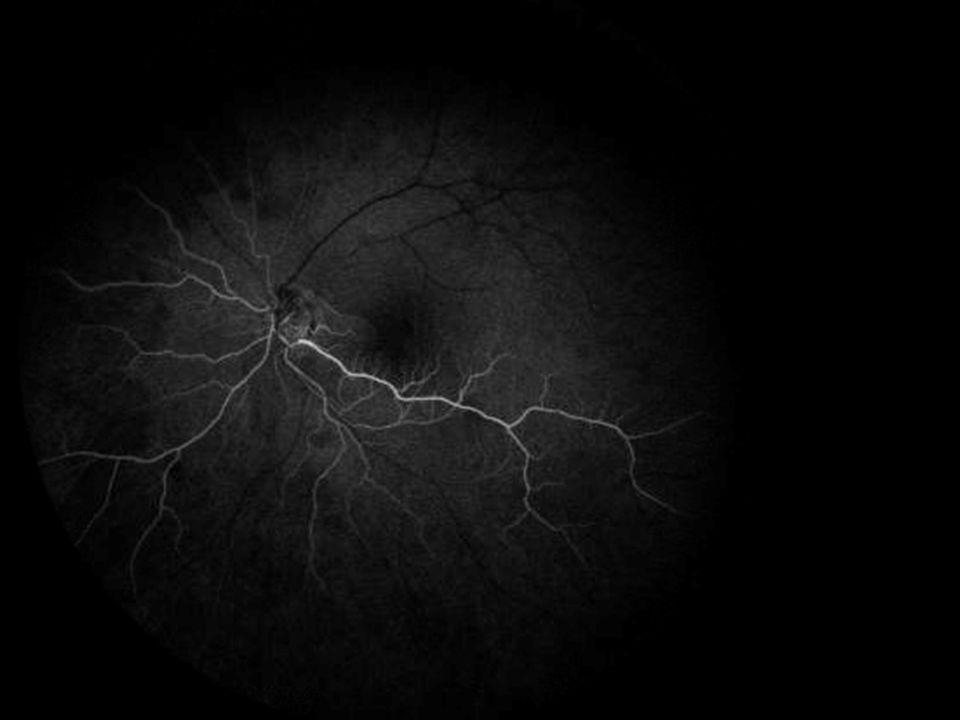
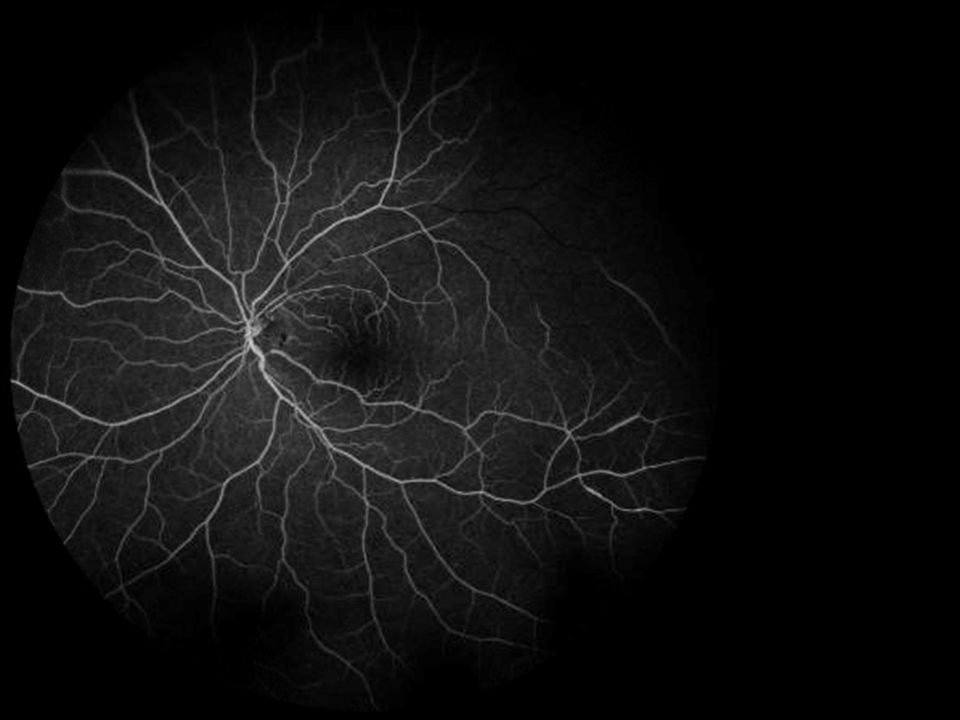
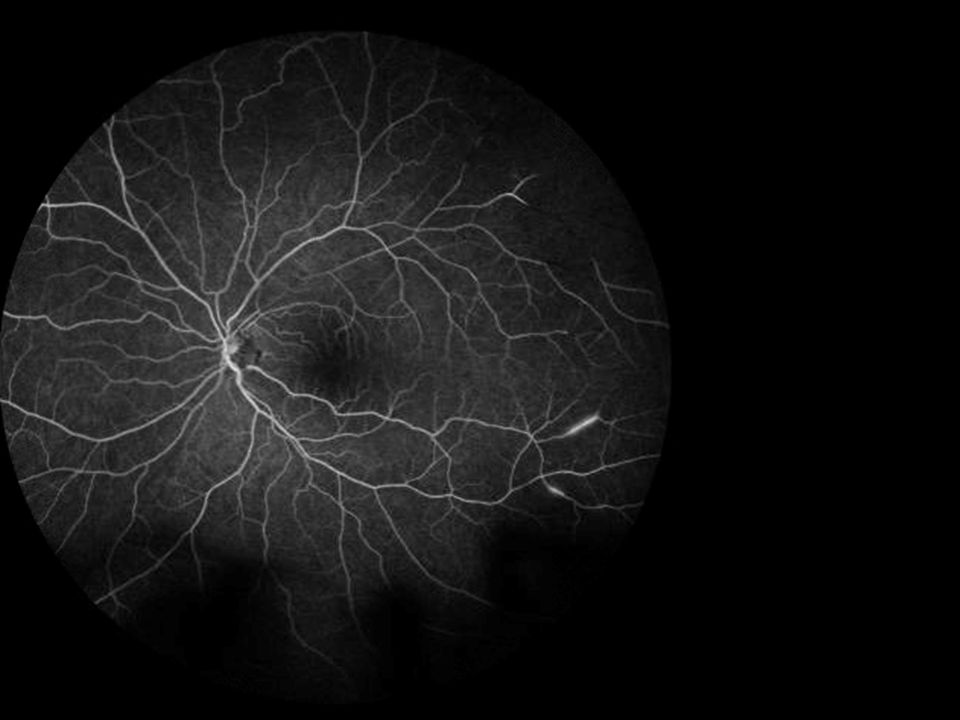
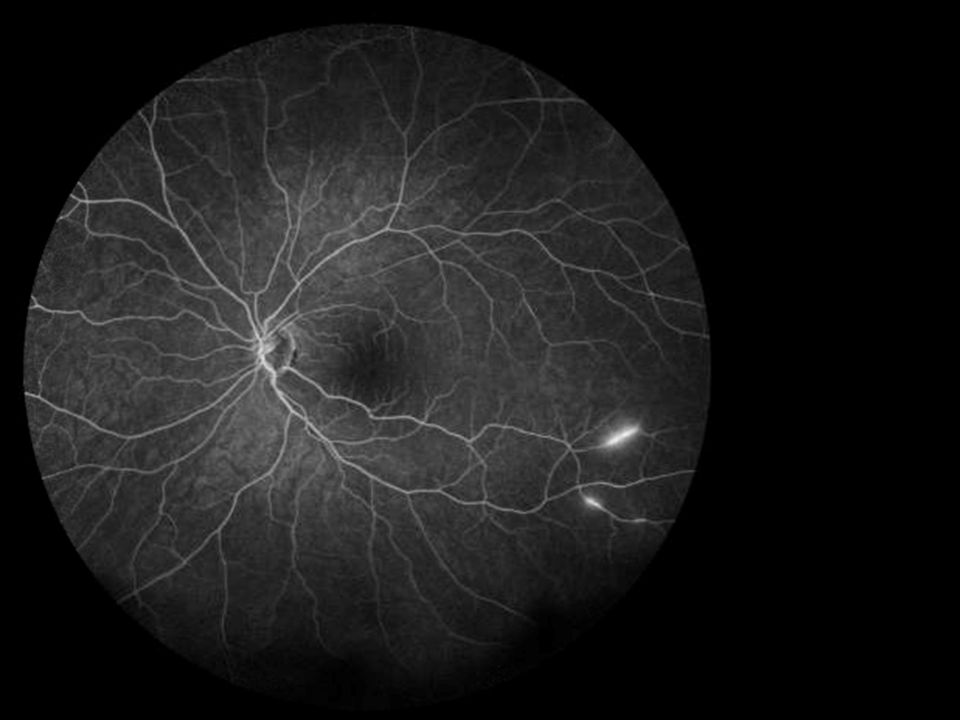
Clinical Findings Examination: Gass plaques: yellow-white retinal arteriolar wall plaques occurring at the midarteriolar segments (not at bifurcations) MRI Findings: classic is multifocal white matter changes including in the corpus collosum, enhance during the acute stage (70%), letomeningeal enhancement (30%) Cerebral angiogram: usually normal (involved precapillary arterioles are <100um) FA: BRAO and multifocal fluorescence of branch arterioles
 MRI Findings: classic is multifocal white matter changes including in the corpus collosum, enhance during the acute stage (70%), letomeningeal enhancement (30%) Cerebral angiogram: usually normal (involved precapillary arterioles are <100um) FA: BRAO and multifocal fluorescence of branch arterioles")
27
Treatment: – Steroids – IMT: cyclophsophamide, mcophenolate, azathioprine, newer biologics – IVIG

28
Pathophysiology: Unknown to date Prognosis: – Difficult to predict at onset as some doe well with limited treatment while others have a recurrent disease process – Usually self-limited lasting 2-4 years – Unfortunately some patients end up suffering long term congitive deficits, gait disturbances, and hearing loss

29
3 month follow-up apt Vision stable On Cellcept 1000mg and Prednisone taper, repeat MRI in 4 months

39
References Egan, R., Gass, J. et al. Retinal arterial wall plaques in Susac Syndrome. American Journal Ophthalmology 2003, April 135 (4) 483-486 Susac, J. Susac’s Syndrome. American Journal of Neuroradiology 2004, 25:352-352
 Susac, J. Susac’s Syndrome. American Journal of Neuroradiology 2004, 25:")
Similar presentations















 HPI: A 74-y Caucasian.>")



 Etiology is.>")




