Download presentation
Presentation is loading. Please wait.

1
Depart. Of Pulmonology & Critical Care Medicine R4 백승숙

2
CASE

3
Asthma ; a heterogeneous disease, with varied triggers, manifestations, and responsiveness to treatment The reasons for this difference in responsiveness to treatment –The degree of airway inflammation –Presence or absence of mucus plugging, –Individual responsiveness to β 2 -adrenergic and corticosteroid

4
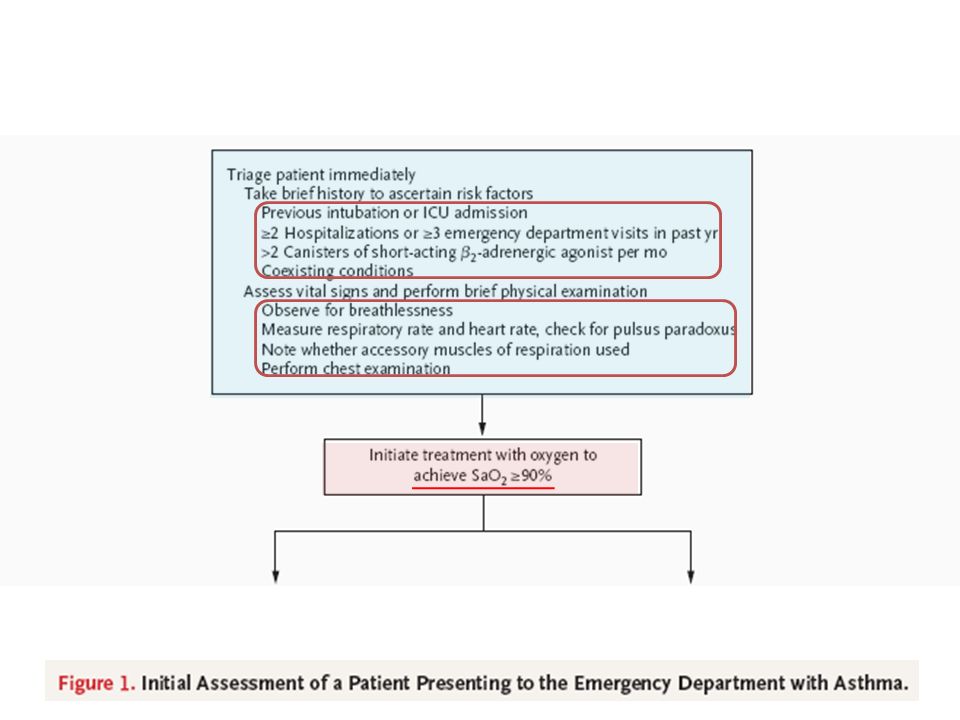
Initial Assessment in the Emergency Department The major challenge in the emergency department Determining which patients can be discharged quickly and which need to be hospitalized Patients presenting to the emergency department with asthma should be evaluated and triaged quickly to assess the severity of the exacerbation and the need for urgent intervention A brief history should be obtained & A limited physical examination performed This assessment should not delay treatment It can be performed while patients receive initial treatment This assessment should not delay treatment It can be performed while patients receive initial treatment

5
Initial Assessment in the Emergency Department Signs of life-threatening asthma which necessitate admission –Altered mental status –Paradoxical chest or abdominal movement –Absence of wheezing Factors that are associated with an increased risk of death from asthma –Previous intubation or admission to an ICU –Two or more hospitalizations for asthma during the past year –Low socioeconomic status –Various coexisting illnesses The measurement of lung function Laboratory and imaging studies

6
Treatment in the Emergency Department All patients should be treated initially –Oxygen to achieve an arterial oxygen saturation of 90% or greater –Inhaled short-acting β2-adrenergic agonists –Systemic corticosteroids The dose and timing of these agents and the use of additional pharmacologic therapy depend on the severity of the exacerbation

9
Treatment in the Emergency Department Inhaled short-acting β 2 -adrenergic agonists should be administered immediately on presentation, and administration can be repeated up to three times within the first hour Metered-dose inhalers vs. Nebulizer - Cates CJ, Crilly JA, Rowe BH. Cochrane Database Syst Rev 2006 Intermittent administration vs. Continuous administration - Rodrigo GJ, Rodrigo C. Chest 2002 - Camargo CA Jr, Spooner CH, Rowe BH. Cochrane Database Syst Rev 2003 Oral administration of β 2 - adrenergic agonists is not recommended The long-acting inhaled β 2 -adrenergic salmeterol has not been studied for the treatment of exacerbations β 2 -Adrenergic Agonists

10
Adverse effects ; tachycardia, palpitations, tremor, hypokalemia R-enantiomer of albuterol

11
Treatment in the Emergency Department Because of its relatively slow onset of action, inhaled ipratropium is not recommended as monotherapy in the emergency department It can be added to a short-acting β 2 -adrenergic agonist for a greater and longer-lasting bronchodilator effect Ipratropium + β 2 - adrenergic vs. β 2 -adrenergic agonist alone –Reduce rates of hospitalization by approximately 25% –No apparent benefit of continuing ipratropium after hospitalization - Plotnick LH, Ducharme FM. Cochrane Database Syst Rev 2000 Anticholinergic Agents

12
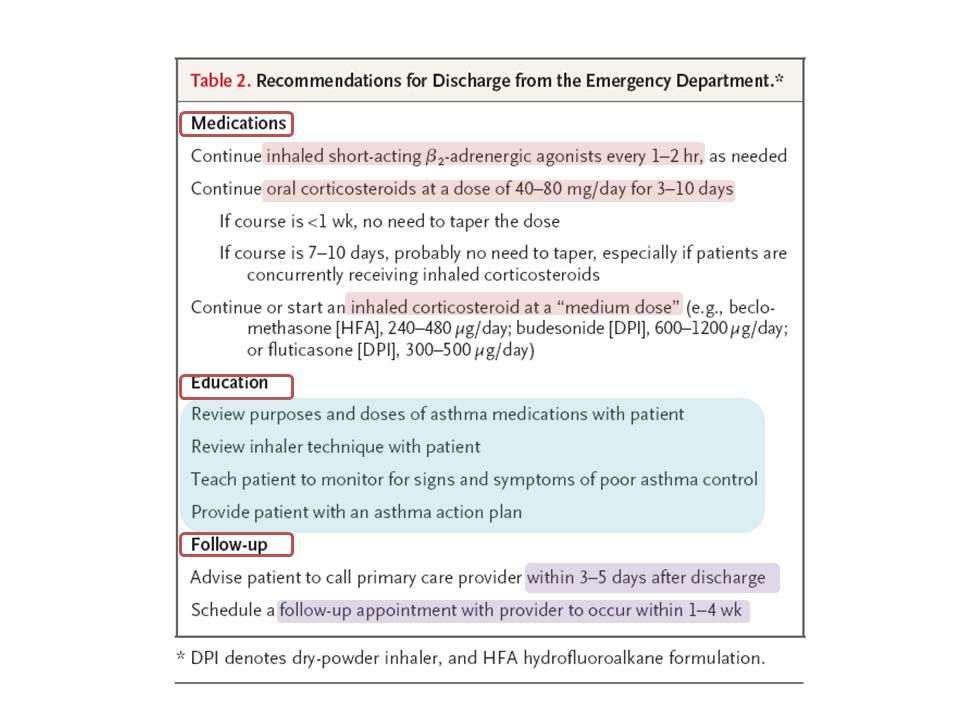
Treatment in the Emergency Department Systemic corticosteroids is associated with a more rapid improvement in lung function, fewer hospitalizations, and a lower rate of relapse after discharge from the emergency department Oral corticosteroids vs. Intravenous corticosteroids - Jonsson S, Kjartansson G, Gislason D, Helgason H. Chest 1988 No significant advantage of doses greater than 100 mg per day of prednisone equivalent The most recent guidelines from the National Asthma Education and Prevention Program (NAEPP) recommend - 40 to 80 mg per day in one dose or two divided doses Systemic Corticosteroids
 recommend - 40 to 80 mg per day in one dose or two divided doses Systemic Corticosteroids.")
13
Treatment in the Emergency Department Inhaled corticosteroids preferred for long-term asthma control A randomized, controlled trial –1006 consecutively enrolled patients with acute asthma –Treated in a Canadian emergency department Inhaled budesonide + Oral corticosteroids vs. Oral corticosteroids –48% reduction in the rate of relapse at 21 days –Improvement in the quality of life and asthma symptoms - Rowe BH, Bota GW, Fabris L, Therrien SA, Milner RA, Jacono J. JAMA 1999 Inhaled Corticosteroids

14
Adverse effects ; dry mouth, cough, and blurred vision Adverse effects ; adrenal suppression, growth suppression, osteoporosis, muscle weakness, hypertension, weight gain, diabetes, cataracts, dermal thinning

15
Treatment in the Emergency Department Methylxanthines ; Increases the risk of adverse events without improving outcomes Antibiotics ; should not be used routinely, but rather should be reserved for patients in whom bacterial infection seems likely Neither aggressive hydration nor administration of mucolytic agents is recommended for acute exacerbations Treatments That Are Not Recommended

16
Assessment of Response to Treatment Patients should be reassessed after the first treatment with an inhaled bronchodilator and again at 60 to 90 minutes (i.e., after three treatments) Assessment after 1 hour vs. Initial assessment - Kelly AM, Kerr D, Powell C. Respir Med 2004 This assessment should include a survey of symptoms, a physical examination, and measurement of FEV1 or PEF (and ABGA)
.")
19
Education of Patients The need for treatment in the emergency department often reflects inadequate maintenance therapy and insufficient knowledge of how to deal with a worsening of asthma control Presentation to the emergency department provides a unique opportunity to educate patients

20
Management of Respiratory Insufficiency Patients with altered mental status, exhaustion, or hypercapnia Considered for immediate intubation and ventilatory support The procedure should be semi-elective and performed under controlled conditions (vs. performed as an emergency procedure by the first available staff) Noninvasive positive-pressure ventilation Higher FEV1 value at 4 hours and a lower rate of hospitalization - Soroksky A, Stav D, Shpirer I. Chest 2003 –Patients who decline intubation –Selected patients who are likely to co-operate with mask therapy
 Noninvasive positive-pressure ventilation Higher FEV1 value at 4 hours and a lower rate of hospitalization - Soroksky A, Stav D, Shpirer I. Chest 2003 –Patients who decline intubation –Selected patients who are likely to co-operate with mask therapy.")
21
In patients with severe asthma that is refractory to standard treatment, intravenous magnesium sulfate is widely used, but there is controversy regarding its efficacy A meta-analysis of 1669 patients in 24 studies weakly –Intravenousmagnesium sulfate (used in 15 studies) –Nebulized magnesium sulfate (used in 9 studies) –Improved lung function but no significant effect on hospital adm. A large multicenter trial in the United Kingdom (Current Controlled Trials number, ISRCTN04417063) Magnesium sulfate
 Magnesium sulfate.")
22
A mixture of helium and oxygen, usually 79% and 21% –That reduces airflow resistance within regions of the bronchial tree where turbulent flow predominates –It is thought to reduce the work of breathing and to improve delivery of aerosolized medications –Its role in the management of acute severe asthma is unclear A Cochrane analysis of 544 patients in 10 trials –Heliox might be beneficial in patients with severe airflow obstruction who have not had a response to initial treatment Heliox

23
The administration of oral leukotriene inhibitors results in increases in the FEV1 within 1 to 2 hours Their usefulness in emergency department is unclear A randomized, placebo-controlled trial –583 adults whose FEV1 remained at 50% or less of the predicted value after 60 minutes of standard care Intravenous montelukast Significantly improved the FEV1 at 60 minutes But did not reduce the rate of hospitalization Leukotriene inhibitors

24
Risk for death related to asthma Chronic uncontrolled asthma necessitating daily rescue use of albuterol Not receiving daily controller therapy Treatment with oxygen, aerosolized albuterol and ipratropium, and systemic corticosteroids should be initiated Monitored closely and reassessed signs and symptoms Decision to admit or discharge within 4 hours

Similar presentations



>")


 Asthma GP monitoring Guideline 2) Asthma Diagnosis Guideline 3) Acute asthma.>")













 Professor Bill MacNee>")
 Diagnosis and management of chronic asthma in line with current BTS guidelines (Dr Lowery) 3 x Case.>")
