Download presentation
Presentation is loading. Please wait.

1
Antidepressants NS204

2
Antidepressant Drug Types
Tricyclic & related drugs Monoamine oxidase inhibitors Selective serotonin reuptake inhibitors Other drugs

3
Depression Somatic Features Psychological Features Anxiety Features
Concentration & attention Self esteem Unworthiness Pessimism Death wish Suicidality Anxiety Features Anhedonia Emotional reactivity Sleep & EMW (~ 2 hrs) DMV (mornings worse) Collaterally reported psychomotor retardation Appetite Weight Libido Self confidence Guilt Tension Worry Distress
 DMV (mornings worse) Collaterally reported psychomotor retardation. Appetite. Weight. Libido. Self confidence. Guilt. Tension. Worry. Distress.")
4
What can antidepressants do...?
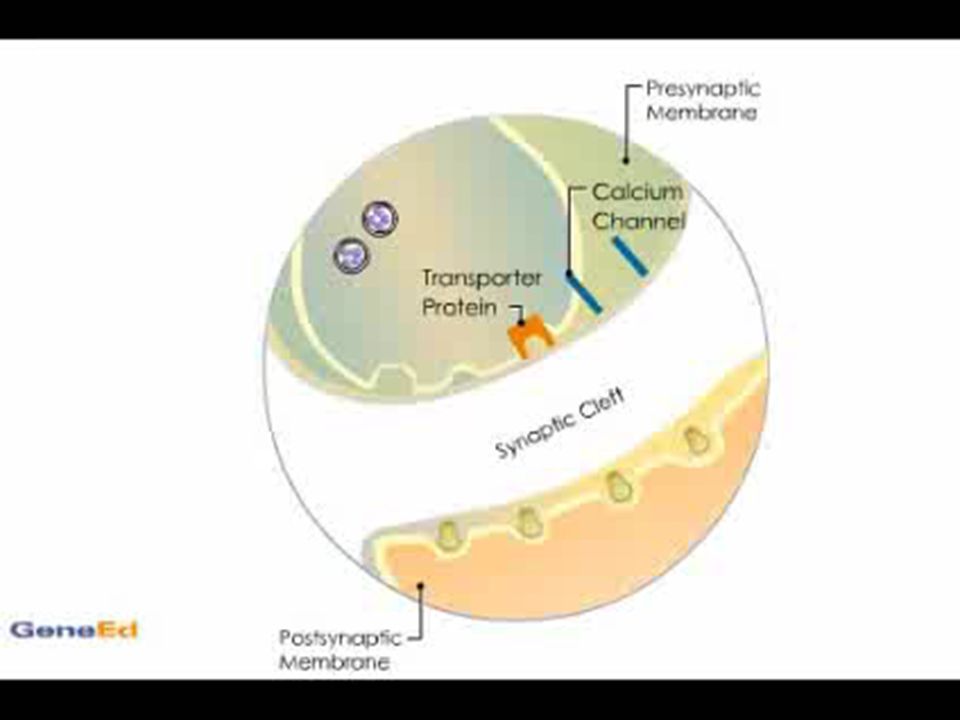
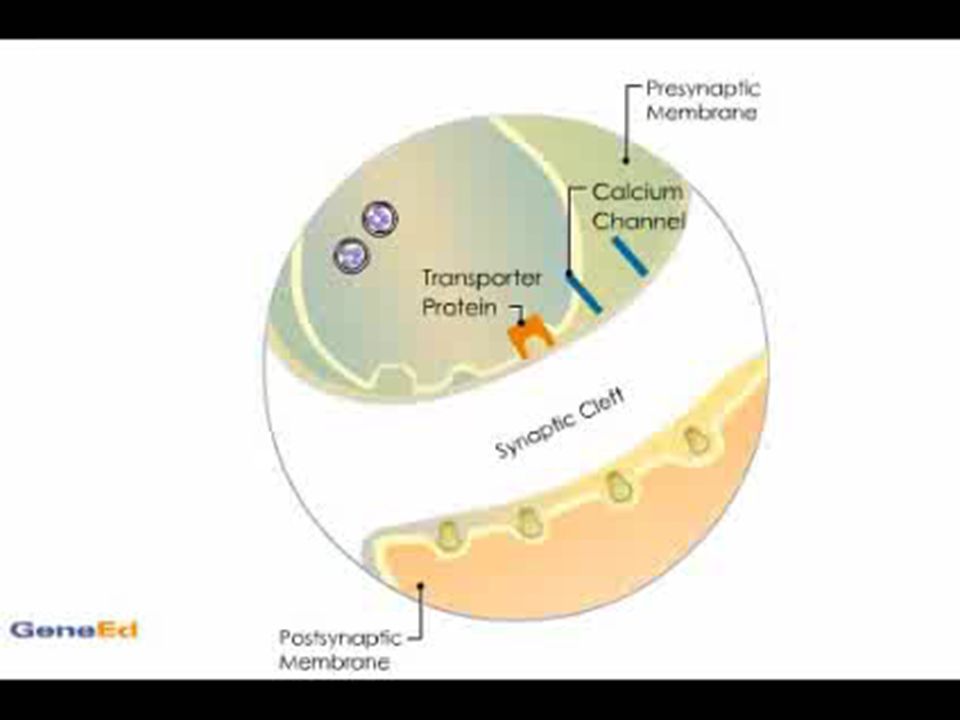
The older drugs; the tricyclics & related compounds and the MAOIs work best on the somatic or “vital” features of depression SSRIs and other drugs whose main therapeutic mode of action is on the serotonergic system work best on the anxiety-related elements There is no compelling evidence that any antidepressant impacts directly on the psychological features of depression Most antidepressants, including the tricyclics & SSRIs, work by blocking reuptake of neurotransmitters. Others, including the MAOIs, work by inhibiting the action of enzymes that deactivate neurotransmitters

6
Tricyclic & related drugs
Therapeutic effect has been linked inhibiting the reuptake of NE (primarily) & to a lesser extent, of 5HT Due to their action on the NE system, their effect is often referred to as ‘energy enhancing’ Therefore they are most effective for moderate to severe depressive episodes where there are pronounced somatic features Tricyclics & related drugs are also sedative, depending on the degree to which they block H1 receptors – this helps with sleep The less sedative drugs tend to suit people who are experiencing anhedonia and general social withdrawal The more sedative drugs, in partciular trazodone (Molipaxin®), tend to suit people who have anxiety features
 & to a lesser extent, of 5HT. Due to their action on the NE system, their effect is often referred to as ‘energy enhancing’ Therefore they are most effective for moderate to severe depressive episodes where there are pronounced somatic features. Tricyclics & related drugs are also sedative, depending on the degree to which they block H1 receptors – this helps with sleep. The less sedative drugs tend to suit people who are experiencing anhedonia and general social withdrawal. The more sedative drugs, in partciular trazodone (Molipaxin®), tend to suit people who have anxiety features.")
7
What features does Geraldine have?
“Vital” features Psychological Features Concentration & attention Self esteem Unworthiness Pessimism Death wish Suicidality Anxiety Features Anhedonia Emotional reactivity Sleep & EMW (~ 2 hrs) DMV (mornings worse) Collaterally reported psychomotor retardation Appetite Weight Libido Self confidence Guilt Tension Worry Distress
 DMV (mornings worse) Collaterally reported psychomotor retardation. Appetite. Weight. Libido. Self confidence. Guilt. Tension. Worry. Distress.")
8
Tricyclic & related antidepressants
Why do about 10 to 20% of patients fail to respond to tricyclic and related antidepressant drugs? Tricyclic antidepressants don’t really have a direct impact on the psychological features of depression Inadequate dosage may account for some instances It could be a question of the wrong drug for the wrong person, and sometimes another tricyclic might work

9
Tricyclic & related antidepressants
Lethal in overdose, especially amitryptiline & dosulepin (Prothiaden®) Require gradual withdrawal – if stopped suddenly after regular administration for 8 weeks or more, the following may occur: Gastro-intestinal symptoms (nausea, vomiting, anorexia) Headache Giddiness ‘Chills’ Insomnia Less often, hypomania, panic-anxiety or extreme motor restlessness may occur
 Require gradual withdrawal – if stopped suddenly after regular administration for 8 weeks or more, the following may occur: Gastro-intestinal symptoms (nausea, vomiting, anorexia) Headache. Giddiness. ‘Chills’ Insomnia. Less often, hypomania, panic-anxiety or extreme motor restlessness may occur.")
10
Main Adverse Effects Tricyclics are related to the phenothiazines and have similar adverse effects to them, for the most part anticholinergic, but also: Seizures Hepatic reactions Haematological reactions Cardiotoxicity Drowsiness (H1) Urinary retention Hypotensive effects Hyponatraemia Neuroleptic Malignant Syndrome (rarely, highest risk with mainserin, where 1/12 blood count is advised during first 3/12)
 Urinary retention. Hypotensive effects. Hyponatraemia. Neuroleptic Malignant Syndrome (rarely, highest risk with mainserin, where 1/12 blood count is advised during first 3/12)")
11
Tricyclic Adverse Effect Profiles
Amitriptyline Clomipramine (Anafranil®) Dosulepin (Prothiaden®) Doxepin (Sinequan®) Trimipramine (Surmontil®) Imipramine (Tofranil®) Lofepramine (Gamanil®) Nortriptyline (Allegron®) Trazodone (Molipaxin®)* Mianserin* Sedative (H1) ++ + Anticholinergic (M) ++ +++ + * - tricyclic-related compounds
 Dosulepin (Prothiaden®) Doxepin (Sinequan®) Trimipramine (Surmontil®) Imipramine (Tofranil®) Lofepramine (Gamanil®) Nortriptyline (Allegron®) Trazodone (Molipaxin®)* Mianserin* Sedative (H1) ++ + Anticholinergic (M) * - tricyclic-related compounds.")
12
Imipramine (Tofranil®) & Amitryptiline
In the liver, imipramine is broken down into desipramine & amitryptiline to nortriptyline Both of these compounds inhibit NE reuptake Neither inhibits 5HT reuptake

13
Monoamine Oxidase Inhibitors
Phenelzine (Nardil®) Tranylcypromine Isocarboxazid Moclobemide (Manerix®)
 Tranylcypromine. Isocarboxazid. Moclobemide (Manerix®)")
14
Monoamine Oxidase Inhibitors
Have a similar impact on “vital”, somatic features as tricyclics & related compounds Rather than inhibiting reuptake, they inhibit the enzymes that break down 5HT & NE They do not have the same histaminergic effects as the tricyclics, and so have a pronounced stimulant effect and are best taken in the morning (particularly tranylcypromine) Phenelzine & isocarboxazid are the least stimualting & most popular MAOIs
 Phenelzine & isocarboxazid are the least stimualting & most popular MAOIs.")
16
Monoamine Oxidase Inhibitors
Usually used as a drug of last resort due to dangers of dietary and drug interactions Like tricyclics, gradual withdrawal is necessary Most effective for depression with atypical, hypochondriacal or hysterical features as well as phobic anxiety disorders

17
MAOI dietary & drug interactions
MAOIs potentiate the pressor effects of indirect acting sympathomimetics (found mainly in decongestant preparations) and both should not be used together MAOIs also potentiate the pressor effect of tyramine, a compound found in certain foods, which should be avoided by people on MAOIs Avoid: mature cheese pickled herring broad bean pods meat/yeast extract (Bovril®, Oxo®, Marmite®) fermented soya bean extract shrimp paste caviar
 and both should not be used together. MAOIs also potentiate the pressor effect of tyramine, a compound found in certain foods, which should be avoided by people on MAOIs. Avoid: mature cheese. pickled herring. broad bean pods. meat/yeast extract (Bovril®, Oxo®, Marmite®) fermented soya bean extract. shrimp paste. caviar.")
18
MAOI dietary precautions
The person should be advised to eat fresh foods only and to avoid game Alcohol should also be avoided The dangers of drug & dietary interaction persist for up to 2 weeks after discontinuation of MAOIs Throbbing headache may be indicative of tyramine interaction and the person should receive emergency medical attention

19
Other Antidepressants
Triptafen® is a compound preparation of amitriptyline hydrochloride and perphenazine Motival® is a compound preparation of nortriptyline hydrochloride and fluphenazine Mirtazapine (Zispin®) Reboxotine (Edronax®) Tryptophan (Optimax®) Duloxetine (Cymbalta®, Yentreve®) Flupentixol (Fluanxol®)
 Reboxotine (Edronax®) Tryptophan (Optimax®) Duloxetine (Cymbalta®, Yentreve®) Flupentixol (Fluanxol®)")
20
Mirtazapine (Zispin®)
Presynaptic antagonist of alpha2-adrenoceptors Increases central NE and 5HT transmission through a nonspecific alpha-blockade that causes presynaptic alpha2-receptors to increase NE release Also a 5HTR-2a antagonist LSD & other hallucinogenic drugs act at this site 5HTR-2a antagonism has not got a very good antidepressant or anxiolytic effect Benefits may be linked to fact that 5HTR-2a antagonists can be beneficial for derealisation & dissociative symptoms, part of the effects of LSD & some depression/anxiety presentations Has sedative effect Adverse effects include increased appetite & weight gain Increased risk of orthostatic hypotension & NMS

21
Reboxetine (Edronax®)
SNRI - inhibits NE reuptake (does not affect 5HT reuptake) Has stimulant effect – best taken am No anticholinergic effects Can cause impotence
 Has stimulant effect – best taken am. No anticholinergic effects. Can cause impotence.")
22
Selective serotonin reuptake inhibitors (SSRIs)
Citalopram (Cipramil®) Escitalopram (Cipralex®) Fluoxetine (Prozac®) Fluvoxamine (Faverin®) Paroxetine (Seroxat®) Sertraline (Lustral®) Duloxetine (Cymbalta®, Yentreve®)* Venlafaxine (Efexor®)* * - Also have SNRI effect
 Escitalopram (Cipralex®) Fluoxetine (Prozac®) Fluvoxamine (Faverin®) Paroxetine (Seroxat®) Sertraline (Lustral®) Duloxetine (Cymbalta®, Yentreve®)* Venlafaxine (Efexor®)* * - Also have SNRI effect.")
23
Selective serotonin reuptake inhibitors (SSRIs)
Inhibit reuptake of 5HT No more effective in the long term than tricyclics Fewer antimuscarinic and cardiotoxic effects than tricyclics

24
Discontinuing SSRIs Adverse effects that can occur if treatment with an SSRI is abruptly withdrawn: - Gastro-intestinal disturbances - Headache - Anxiety - Dizziness - Paraesthesia - Sleep disturbances - Fatigue - Flu-like symptoms - Sweating

25
SSRIs – Facts and Fallacies
Blocking serotonin reuptake is not necessary for antidepressant action Studies have found that effective blockage of serotonin reuptake by SSRIs and the speed with which they treat depression are not correlated SSRIs tend not to be effective for severe depression There is no evidence that depressed people have disordered serotonin systems (Healy 2009)
")
26
So how do SSRIs work? SSRIs have an anxiolytic effect, and are prescribed for some anxiety disorders Therefore, it has been suggested that this anxiolytic effect plays a key part in their therapeutic usefulness (Healy 2005)
")
27
Venlafaxine It is advisable that people commencing treatment with venlafaxine have an ECG, and also have their blood pressure measured before and periodically during treatment.

28
Venlafaxine Adverse effects that can occur if treatment with venlafaxine is abruptly withdrawn: - Gastro-intestinal disturbances - Headache - Anxiety - Dizziness - Paraesthesia - Tremor - Sleep disturbances - Sweating

29
5HT Syndrome Similar to NMS, which can also occur
Not just a risk on SSRIs, but on any antidepressants affecting serotonergic system, person experiences: Muscular jerks & twitches Tremor Confusion, agitation, restlessness Excessive shivering & sweating Hyperreflexia Diarrhoea Not as dangerous as NMS, but fatalities have occurred Usually resolves with discontinuation of drug

Similar presentations




 are a class of powerful antidepressant drugs. They are particularly effective in treating.>")








 Depression>")



 ~>")

