Download presentation
Presentation is loading. Please wait.

1
Rahul Batra,1 Ben S. Cooper,5,6 Craig Whiteley,2 Amita K. Patel,1 Duncan Wyncoll,2 and Jonathan D. Edgeworth1,3 1Directorate of Infection and 2Intensive Care Unit, Guy’s and St Thomas’ National Health Service Foundation Trust, and 3Department of Infectious Diseases, King’s College London School of Medicine at Guy’s, King’s College, and St Thomas’ Hospitals, London, and 4Center for Clinical Vaccinology and Tropical Medicine, Nuffield Department of Clinical Medicine, University of Oxford, Churchill Hospital, Oxford, United Kingdom; and 5Mahidol-Oxford Tropical Medicine Research Unit, Faculty of Tropical Medicine, Mahidol University, Bangkok, Thailand Clinical Infectious Diseases 2010; 50:210–7 Efficacy and Limitation of a Chlorhexidine-Based Decolonization Strategy in Preventing Transmission of MRSA in an Intensive Care Unit R2 조 욱 / Prof. 손준성

2
Introduction The mainstay of infection control –prompt identification of MRSA-colonized patients –institution of contact precautions + enforcing hand hygiene practice Guidelines recommendation –active surveillance cultures from high-risk patients :debateful –Isolation or cohorting : unclear benefit in ICU –surface antiseptics (chlorhexidine…) : benefit reported for high-risk groups ? routine cleansing of all patients ?

3
surface antiseptics as decolonization agents –Emerging resistance is a particular concern –MRSA resistant to mupirocin –Genes increasing MBCs to antiseptics plasmid-borne qacA/B genes code for multidrug efflux pumpsplasmid-borne qacA/B genes code for multidrug efflux pumps –2~4 X increase in MBCs for antiseptics –10%~20% of UK, 63% of European, 80% of Brazilian and 55% of Taiwanese MRSA strains Measures to control MRSA transmission in ICU –Educational campaign –Cohorting –surface antiseptic protocol

4
purpose To assess the effect of chlorhexidine-based antiseptic protocol during TW MRSA outbreak

5
Methods Clinical setting and infection control practice –two 15-bed ICUs in The St Thomas’ Hospital site –All admitted Pts 2002.1.1~2006.4.20 –contact precautions –MRSA screening swab samples nose, perineum, axilla, throat, rectal swab, other samplesnose, perineum, axilla, throat, rectal swab, other samples –intervention A : Educational campaign (2003.7.15~) –intervention B : Cohorting (2003.10.15~) –intervention C : surface antiseptic protocol (2004.4.26~) chlorhexidine gluconate nostrils, around the mouth, tracheostomy sites, groin, axillae, and skinfoldschlorhexidine gluconate nostrils, around the mouth, tracheostomy sites, groin, axillae, and skinfolds
 –intervention B : Cohorting ( ~) –intervention C : surface antiseptic protocol ( ~) chlorhexidine gluconate nostrils, around the mouth, tracheostomy sites, groin, axillae, and skinfoldschlorhexidine gluconate nostrils, around the mouth, tracheostomy sites, groin, axillae, and skinfolds")
6
Data collection and definitions –age, sex, specialty, APACHE II score, length of ICU stay, ICU mortality rate, dates of isolation of MRSA and its antibiotic resistance profile, dates of ventilation and renal replacement, and staffing levels. –Importing MRSA : MRSA cultured within 48 h after ICU admission –Acquiring MRSA : MRSA isolated for the first time after 48hrs in ICU Statistical analysis –TW and non-TW MRSA acquisition data separate segmented regression models. –weekly number of acquisitions Poisson models

7
Results

8
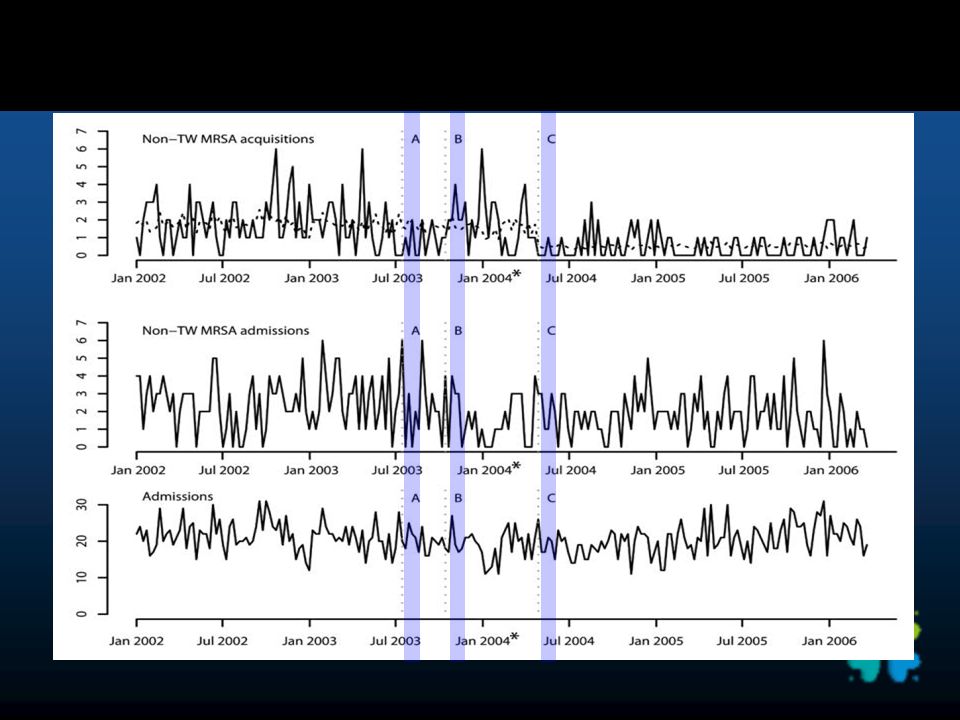
Clinical and epidemiologic characteristics Total 4570 pts admitted to ICU (for a total of 44,505 days) 517 (11%) admitted with MRSA infection, 347 of 3073 susceptible pts staying >48 h acquired MRSA antiseptic protocol appeared to be associated with an immediate reduction in acquisition of non-TW, but not TW strains no apparent effect after the educational campaign or cohorting
 517 (11%) admitted with MRSA infection, 347 of 3073 susceptible pts staying >48 h acquired MRSA antiseptic protocol appeared to be associated with an immediate reduction in acquisition of non-TW, but not TW strains no apparent effect after the educational campaign or cohorting")
9
Weekly No. of ICU admissions and acquisitions of TW and non-TW strains

11
Table 1. Clinical and Microbiological Characteristics of Pts Admitted to ICU before and after Antiseptic Protocol

12
Estimating the impact of interventions on transmission of MRSA. Table 2. Estimated Parameters from the Poisson Segmented Regression Applied to the Non-TW and TW MRSA Data

13
Table 4.Chlorhexidine and Triclosan Minimum Bactericidal Concentrations (MBCs) for Selected TW and Non-TW MRSA Acquisition Isolates Table 3. Estimated Bayesian Model-Averaged Incidence Rate Ratios (IRRs) for TW and Non-TW MRSA Acquisitions
 for TW and Non-TW MRSA Acquisitions.")
14
Table 4.Chlorhexidine and Triclosan Minimum Bactericidal Concentrations (MBCs) for Selected TW and Non-TW MRSA Acquisition Isolates Anatomical sites of MRSA isolation.
 for Selected TW and Non-TW MRSA Acquisition Isolates Anatomical sites of MRSA isolation.")
15
Discussion Chlorhexidine surface antiseptic protocol into an ICU where MRSA prevalence is stable at ∼ 20% can lead to an immediate and sustained reduction in transmission of susceptible MRSA stains. Although basic infection control interventions were already in place and actively reenforced, this does not mean that a more sustained and effective campaign would not have had an effect comparable to that of the antiseptic protocol. However, the data contribute to a body of evidence indicating that use of antiseptics, either as part of a decolonization strategy for known MRSA- colonized patients or administered to all ICU patients can be useful in controlling MRSA surface antiseptics have only limited efficacy at eradicating MRSA in multisite-colonized patients prompting systematic reviews suppression of colonization can reduce MRSA transmission

16
One concern about the use of antiseptics is the lack of effect on and, therefore, selection of resistant strains The TW strains – –carried qacA/B genes, demonstrated 3-fold increased chlorhexidine MBCs in vitro – –not affected in anatomical site colonization or transmissibility after introduction of the antiseptic protocol – –all models provided evidence that the antiseptic protocol increased transmission of TW MRSA – –MBC of TW MRSA, still well below the chlorhexidine concentrations used, greater activity and/or expression of qacA/B on body surface localized TW MRSA and, therefore, a higher MBC in vivo than in vitro. ineffective application or inactivation on skin, less likely

17
When prevalence of qacA/B is high – – cautions against widespread use of chlorhexidine Hand hygiene or cohorting may have reduced TW MRSA acquisitions – –may be an artefact because the exponential increase in TW MRSA is clearly not sustainable in a small ICU. A better assessment of the effect of interventions on transmission of MRSA in small units – –individual-level data within a mechanistic transmission model to account for the fact that, as the numbers colonized increase fewer patients remain at risk. hospital MRSA strains can differ in their virulence and response to infection control interventions storage and analysis of MRSA strains identified in intervention studies may help to develop a more targeted approach to enhanced infection control measures.

18
Conclusion antiseptic protocol caused an immediate reduction in transmission of non-TW MRSA and moderate evidence of an immediate increase in transmission of TW MRSA.

Similar presentations



















>")