Download presentation
Presentation is loading. Please wait.

1
Immune Disorders Kimiko Suzue, MD PhD October 4, 2011

2
Question 101 A 20 year old medical student develops a skin rash on her arms and hands 2 days after hiking in the Adirondack mountains. A skin biopsy of her blisters would be expected to have the histologic appearance below, with a dense lymphocytic infiltrate. This is characteristic of which type of hypersensitivity reaction? Type I Type II Type III Type IV Answer: D

3
Question 101 Answer: D

4
Question 101 A 20 year old medical student develops a skin rash on her arms and hands 2 days after hiking in the Adirondack mountains. A skin biopsy of her blisters would be expected to have the following histologic appearance with a dense lymphocytic infiltrate. This is characteristic of which type of hypersensitivity reaction? Type I Type II Type III Type IV Answer: D

5
Question 102 A 55 year old woman undergoes a lip biopsy (minor salivary gland biopsy). Shown is the histology which shows a dense periductal and perivascular lymphocytic infiltrate. This biopsy most strongly supports the diagnosis of: Amyloidosis DiGeorge syndrome Sjogren syndrome Systemic sclerosis Systemic lupus erythematosus Answer: C Langerman et al., The Laryngoscope 2007
. Shown is the histology which shows a dense periductal and perivascular lymphocytic infiltrate. This biopsy most strongly supports the diagnosis of: Amyloidosis. DiGeorge syndrome. Sjogren syndrome. Systemic sclerosis. Systemic lupus erythematosus. Answer: C. Langerman et al., The Laryngoscope")
6
Question 102 Answer: C Langerman et al., The Laryngoscope 2007

7
Question 102 A 55 year old woman undergoes a lip biopsy (minor salivary gland biopsy). Shown is the histology which shows a dense periductal and perivascular lymphocytic infiltrate. This biopsy most strongly supports the diagnosis of: Amyloidosis DiGeorge syndrome Sjogren syndrome Systemic sclerosis Systemic lupus erythematosus Answer: C Langerman et al., The Laryngoscope 2007
. Shown is the histology which shows a dense periductal and perivascular lymphocytic infiltrate. This biopsy most strongly supports the diagnosis of: Amyloidosis. DiGeorge syndrome. Sjogren syndrome. Systemic sclerosis. Systemic lupus erythematosus. Answer: C. Langerman et al., The Laryngoscope")
8
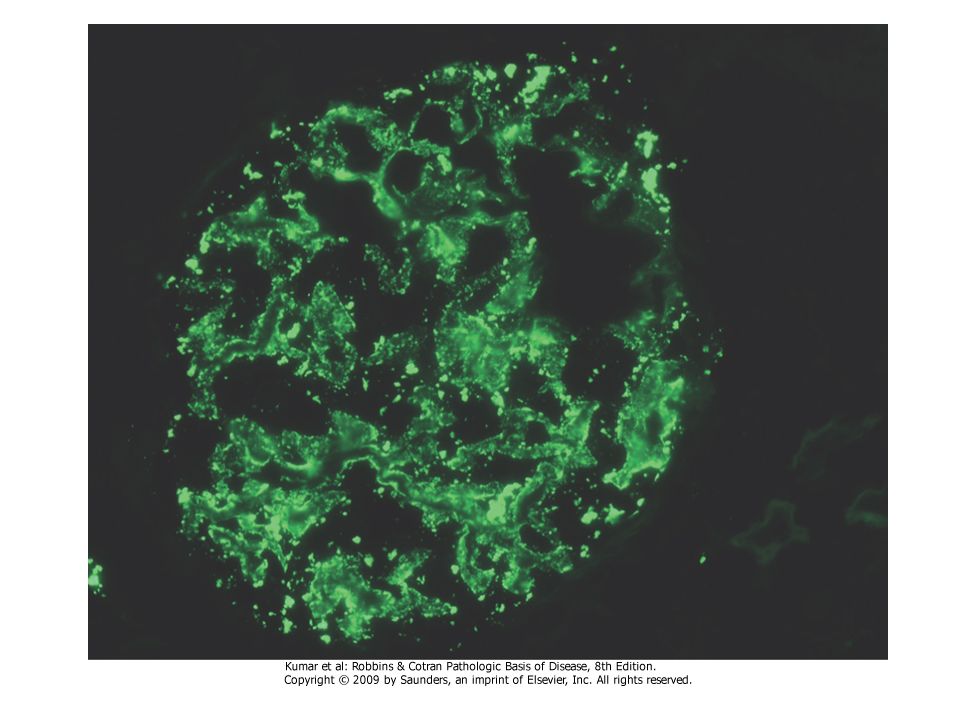
This renal biopsy illustrates:
Question 103 This renal biopsy illustrates: Amyloid deposition and a Congo red stain will confirm the diagnosis Glomerular morphology in a patient with chronic discoid lupus erythematosus IgG deposition secondary to excessive immunoglobulin production in a patient with XLA, Bruton’s Disease. Necrotic glomeruli caused by immune complex deposition commonly seen in type I hypersensitivity reactions Normal histology without diagnostic abnormality Answer: A

10
This renal biopsy illustrates:
Question 103 This renal biopsy illustrates: Amyloid deposition and a Congo red stain will confirm the diagnosis Glomerular morphology in a patient with chronic discoid lupus erythematosus IgG deposition secondary to excessive immunoglobulin production in a patient with XLA, Bruton’s Disease. Necrotic glomeruli caused by immune complex deposition commonly seen in type I hypersensitivity reactions Normal histology without diagnostic abnormality Answer: A

11
Question 104 A 25 year old woman presents to you with this facial rash and a 3-month history of joint pain and sporadic fevers. Her lab studies show an elevated creatinine and blood urea nitrogen level. Which of the following is FALSE? Antibodies to double-stranded DNA and Smith antigens are virtually diagnostic for this entity. A skin biopsy evaluated by immunofluorescence may show IgG deposition at the dermoepidermal junction. Progressive interstitial and perivascular fibrosis in the skin and multiple organs are characteristic of this systemic disorder. She may have a false positive test for syphilis. She may have antibodies to SS-A ribonucleoprotein Answer: C and E

12
Question 105 A 32-year old woman is found to have a congenital immunodeficiency that has remained largely asymptomatic throughout her life. What is her most likely diagnosis? Adenosine deaminase deficiency Bruton’s aggamaglobulinemia Hyper-IgM syndrome Isolated IgA deficiency Wiskott-Aldrich syndrome Answer: D

13
Question 106 A 55 year old woman has subcutaneous fibrosis in her fingers, dysphagia from esophageal fibrosis and episodic vasoconstriction of the arteries and arterioles of her extremities. What is the most likely diagnosis? Amyloidosis CREST syndrome Sjogren syndrome Systemic lupus erythematosus Wiskott-Aldrich syndrome Answer: B

14
Primary amyloidosis refers to:
Question 107 Primary amyloidosis refers to: Autosomal dominant familial disorders with deposition of amyloid in peripheral and autonomic nervous system Localized deposition of AL type amyloid associated with chronic inflammatory conditions Microscopic amyloid deposits found in endocrine tumors such as medullary carcinoma of the thyroid gland Systemic deposition of AA type amyloid generally seen in patients with renal failure undergoing dialysis Systemic deposition of AL type amyloid associated to multiple myeloma and other monoclonal plasma cell dyscrasias Answer: E

15
Question 108 Deposition of antigen-antibody complexes with activation of complement, recruitment of leukocytes by complement products and Fc receptors with release of enzymes and other toxic molecules are characteristic of all of the following, EXCEPT: Arthus reaction Myasthenia gravis Polyarteritis nodosa Serum sickness Systemic lupus erythematosus Answer: B

16
Question 109 The following immunodeficiencies occur due to mutations on the X-chromosome except: Bruton’s agammaglobulinemia DiGeorge’s syndrome Hyper-IgM syndrome Severe combined immunodeficiency Wiskott-Aldrich syndrome Answer: B

17
Question 110 Which of the following statements regarding the human leukocyte antigen system is FALSE? Autoimmune diseases such as rheumatoid arthritis, primary Sjogren syndrome and Type 1 diabetes are associated with alleles at the HLA-DR locus. The HLA-A, HLA-B and HLA-C antigens are the principal antigens involved in tissue graft rejection. The HLA-B27 allele is associated with ankylosing spondylitis. The MHC class I molecules present foreign peptides to CD8 positive T-cells. The MCH molecules HLA-DP, DQ and DR are present on virtually all nucleated cells and platelets. Answer: E

18
End of Quiz

19
Question 101 A 20 year old medical student develops a skin rash on her arms and hands 2 days after hiking in the Adirondack mountains. A skin biopsy of her blisters would be expected to have the following histologic appearance with a dense lymphocytic infiltrate. This is characteristic of which type of hypersensitivity reaction? Type I Type II Type III Type IV Answer: D

20
Hypersensitivity reactions
Type I (immediate or anaphylactic) IgE Type II (antibody-mediated) IgG IgM Type III (immune complex-mediated) Ag-Ab complex Type IV (cell-mediated) T-cells delayed hypersensitivity cytotoxic T lymphocyte (CTL)-mediated cytotoxicity 20
 IgE. Type II (antibody-mediated) IgG IgM. Type III (immune complex-mediated) Ag-Ab complex. Type IV (cell-mediated) T-cells. delayed hypersensitivity. cytotoxic T lymphocyte (CTL)-mediated cytotoxicity. 20.")
21
Type IV T-cell-mediated hypersensitivity
21

22
Type IV Hypersensitivity
antigen (presented by HLA class II macrophages) interacts with T-cell receptor of CD4+ lymphocytes stimulation of antigen-specific CD4+ memory T cells subsequent contact with antigen proliferation of CD4+ memory T cells secretion of IL-2 and other cytokines recruiting of macrophages and stimulation of phagocytic activity of macrophages 22
 interacts with T-cell receptor of CD4+ lymphocytes stimulation of antigen-specific CD4+ memory T cells. subsequent contact with antigen proliferation of CD4+ memory T cells secretion of IL-2 and other cytokines recruiting of macrophages and stimulation of phagocytic activity of macrophages. 22.")
23
Delayed hypersensitivity
antigen (presented by HLA class II macrophages) interacts with T-cell receptor of CD4+ lymphocytes stimulation of antigen-specific CD4+ memory T cells subsequent contact with antigen proliferation of CD4+ memory T cells secretion of IL-2 and other cytokines recruiting of macrophages and stimulation of phagocytic activity of macrophages 23
 interacts with T-cell receptor of CD4+ lymphocytes stimulation of antigen-specific CD4+ memory T cells. subsequent contact with antigen proliferation of CD4+ memory T cells secretion of IL-2 and other cytokines recruiting of macrophages and stimulation of phagocytic activity of macrophages. 23.")
24
CD4 positive lymphocytes in dermis in contact dermatitis
24

25
Cytotoxic T lymphocyte (CTL)-mediated cytotoxicity
Direct CD8+ T cell-mediated killing of target cells (typically tumor cells or virus-infected cells) Specific target cell antigen recognized by T-cell receptor of CD8+ lymphocytes 25
 Specific target cell antigen recognized by T-cell receptor of CD8+ lymphocytes. 25.")
26
Question 108 Deposition of antigen-antibody complexes with activation of complement, recruitment of leukocytes by complement products and Fc receptors with release of enzymes and other toxic molecules are characteristic of all of the following, EXCEPT: Arthus reaction Myasthenia gravis Polyarteritis nodosa Serum sickness Systemic lupus erythematosus Answer: B

27
Question 108 Deposition of antigen-antibody complexes with activation of complement, recruitment of leukocytes by complement products and Fc receptors with release of enzymes and other toxic molecules are characteristic of all of the following, EXCEPT: Arthus reaction Myasthenia gravis anti-AchR ab Polyarteritis nodosa Serum sickness Systemic lupus erythematosus Answer: B

28
Graves’ disease Example of antibody-medated cellular dysfunction, a subtype of Type II hypersensitivity Anti-TSH Receptor Antibody similar mechanism in myasthenia gravis: antibodies react with acetylcholine receptors in motor end plates of skeletal muscles 28

29
Exophthalmos in Graves’ disease
29

30
Graves’ disease. Note epithelial hyperplasia and scalloped colloid
30

31
Goodpasture syndrome an example of Type II hypersensitivity
antiglomerular basement membrane antibodies directed against antigens in glomerular as well as in pulmonary alveolar basement membranes clinical manifestations include glomerulonephritis and pneumonitis with hemoptysis linear immunofluorescence 31

32
Linear immunofluorescence in Goodpasture syndrome
32

33
Question 102 A 55 year old woman undergoes a lip biopsy (minor salivary gland biopsy). Shown is the histology which shows a dense periductal and perivascular lymphocytic infiltrate. This biopsy most strongly supports the diagnosis of: Amyloidosis DiGeorge syndrome Sjogren syndrome Systemic sclerosis Systemic lupus erythematosus Answer: C Langerman et al., The Laryngoscope 2007
. Shown is the histology which shows a dense periductal and perivascular lymphocytic infiltrate. This biopsy most strongly supports the diagnosis of: Amyloidosis. DiGeorge syndrome. Sjogren syndrome. Systemic sclerosis. Systemic lupus erythematosus. Answer: C. Langerman et al., The Laryngoscope")
34
Sjögren syndrome Autoimmune diseases in association with:
keratoconjunctivitis sicca (dry eyes) xerostomia (dry mouth) lymphocytic infiltrates with destruction of acini in lacrimal and salivary glands ANAs anti-SS-B (relatively specific) anti‑SS-A (somewhat less specific) 34
 xerostomia (dry mouth) lymphocytic infiltrates with destruction of acini in lacrimal and salivary glands. ANAs. anti-SS-B (relatively specific) anti‑SS-A (somewhat less specific) 34.")
37
Sjögren syndrome Lymphocytic infiltrate Residual ducts Fat replacing
Glandular elements

38
This renal biopsy illustrates:
Question 103 This renal biopsy illustrates: Amyloid deposition and a Congo red stain will confirm the diagnosis Glomerular morphology in a patient with chronic discoid lupus erythematosus IgG deposition secondary to excessive immunoglobulin production in a patient with XLA, Bruton’s Disease. Necrotic glomeruli caused by immune complex deposition commonly seen in type I hypersensitivity reactions Normal histology without diagnostic abnormality Answer: A

39
Congo Red Stain

40
Polarized congo red stain of renal amyloid

41
Pathogenesis of Amyloidosis
© 2005 Elsevier 41

42
Primary amyloidosis refers to:
Question 107 Primary amyloidosis refers to: Autosomal dominant familial disorders with deposition of amyloid in peripheral and autonomic nervous system Localized deposition of AL type amyloid associated with chronic inflammatory conditions Microscopic amyloid deposits found in endocrine tumors such as medullary carcinoma of the thyroid gland Systemic deposition of AA type amyloid generally seen in patients with renal failure undergoing dialysis Systemic deposition of AL type amyloid associated to multiple myeloma and other monoclonal plasma cell dyscrasias Answer: E

43
Primary amyloidosis refers to:
Question 107 Primary amyloidosis refers to: Autosomal dominant familial disorders with deposition of amyloid in peripheral and autonomic nervous system Localized deposition of AL type amyloid associated with chronic inflammatory conditions Microscopic amyloid deposits found in endocrine tumors such as medullary carcinoma of the thyroid gland Systemic deposition of AA type amyloid generally seen in patients with renal failure undergoing dialysis Systemic deposition of AL type amyloid associated to multiple myeloma and other monoclonal plasma cell dyscrasias Answer: E

44
Question 107 Autosomal dominant familial disorders with deposition of amyloid in peripheral and autonomic nervous system Transthyretin Localized deposition of AL type amyloid associated with chronic inflammatory conditions Secondary amyloidosis-Serum associated amyloid-AA Microscopic amyloid deposits found in endocrine tumors such as medullary carcinoma of the thyroid gland calcitonin Systemic deposition of AA type amyloid generally seen in patients with renal failure undergoing dialysis Beta-microglobulin Systemic deposition of AL type amyloid associated to multiple myeloma and other monoclonal plasma cell dyscrasias Answer: E

45
Question 110 Which of the following statements regarding the human leukocyte antigen system is FALSE? Autoimmune diseases such as rheumatoid arthritis, primary Sjogren syndrome and Type 1 diabetes are associated with alleles at the HLA-DR locus. The HLA-A, HLA-B and HLA-C antigens are the principal antigens involved in tissue graft rejection. The HLA-B27 allele is associated with ankylosing spondylitis. The MHC class I molecules present foreign peptides to CD8 positive T-cells. The MCH molecules HLA-DP, DQ and DR are present on virtually all nucleated cells and platelets.

46
Question 104 A 25 year old woman presents to you with this facial rash and a 3-month history of joint pain and sporadic fevers. Her lab studies show an elevated creatinine and blood urea nitrogen level. Which of the following is FALSE? Antibodies to double-stranded DNA and Smith antigens are virtually diagnostic for this entity. A skin biopsy evaluated by immunofluorescence may show IgG deposition at the dermoepidermal junction. Progressive interstitial and perivascular fibrosis in the skin and multiple organs are characteristic of this systemic disorder. She may have a false positive test for syphilis. She may have antibodies to SS-A ribonucleoprotein Answer: C

47
Systemic Lupus Erythematosus
Head and Neck Manifestations Malar rash (Butterfly Rash) often first sign Erythematous maculopapular eruption after sun exposure Oral ulceration 47
 often first sign. Erythematous maculopapular eruption after sun exposure. Oral ulceration. 47.")
48
Butterfly Rash in Systemic Lupus Erythematosus
48

49
Renal Manifestations of SLE World Health Organization (WHO) classification
I. Normal glomeruli by light microscopy (LM), IF, and EM II. Pure mesangial alterations III. Focal segmental (proliferative) glomerulonephritis IV. Diffuse (proliferative) glomerulonephritis V. Diffuse membranous glomerulonephritis VI. Advanced sclerosing glomerulonephritis 49
, IF, and EM. II. Pure mesangial alterations. III. Focal segmental (proliferative) glomerulonephritis. IV. Diffuse (proliferative) glomerulonephritis. V. Diffuse membranous glomerulonephritis. VI. Advanced sclerosing glomerulonephritis. 49.")
50
SLE – “wire-loop” changes in glomerulus
50

53
Red blood cell cast 53

54
White blood cell cast 54

55
Libman-Sacks Endocarditis in SLE Notice flat, reddish-tan vegetations
Libman-Sacks endocarditis is the most characteristic cardiac manifestation of systemic lupus erythematosus. These lesions most commonly involves mitral and aortic valves although the other valves may be involved. Because of their tiny size and because they seldom embolize these vegetations only rarely cause problems. Libman-Sacks Endocarditis in SLE Notice flat, reddish-tan vegetations 55

56
Question 106 A 55 year old woman has subcutaneous fibrosis in her fingers, dysphagia from esophageal fibrosis and episodic vasoconstriction of the arteries and arterioles of her extremities. What is the most likely diagnosis? Amyloidosis CREST syndrome Sjogren syndrome Systemic lupus erythematosus Wiskott-Aldrich syndrome Answer: B

57
Systemic sclerosis (Scleroderma)
The term scleroderma comes from the Greek words “slerosis” meaning hard and “derma” meaning skin. Scleroderma is a disease of connective tissues, which results from an overproduction of collagen. There is thickening of skin on the arms, legs, face, etc and internal organs (such as the esophagus, gastrointestinal tract, lungs, heart, and kidneys are affected. 57

58
Dysphagia due to esophageal fibrosis
Systemic sclerosis is primarily (by 3:1) a disease of women. Distinctive features include: Cutaneous changes. Raynaud phenomenon, Dysphagia due to esophageal fibrosis Respiratory difficulties due to pulmonary fibrosis Malignant hypertension, which may lead to the development of fatal renal failure 58
 a disease of women. Distinctive features include: Cutaneous changes. Raynaud phenomenon, Dysphagia due to esophageal fibrosis. Respiratory difficulties due to pulmonary fibrosis. Malignant hypertension, which may lead to the development of fatal renal failure. 58.")
59
The CREST syndrome is a milder form of systemic sclerosis characterized by:
Calcinosis: painful calcium deposits in the skin. Raynaud's phenomenon: spasm of tiny arteries in response to cold or stress. Esophageal dysfunction: difficulty swallowing because of scarring in the esophagus. Sclerodactyly: thickening and tightening of skin on the fingers and toes which limits motion. Telangiectasis: tiny redspots on the hands, palms, forearems, face and lips which are caused by dilated capillaries. Calcinosis 59

60
Antinuclear antibody tests in Systemic Sclerosis (Scleroderma)
About 75% of patients with the diffuse form of scleroderma and about 10% of patients with the localized CREST version have antinuclear antibodies directed against DNA topoisomerase (anti-Scl-70). The CREST syndrome most commonly demonstrates anti-centromere antinuclear antibodies. 60
. The CREST syndrome most commonly demonstrates anti-centromere antinuclear antibodies. 60.")
61
Sclerodactyly 61

70
Question 105 A 32-year old woman is found to have a congenital immunodeficiency that has remained largely asymptomatic throughout her life. What is her most likely diagnosis? Adenosine deaminase deficiency Bruton’s aggamaglobulinemia Hyper-IgM syndrome Isolated IgA deficiency Wiskott-Aldrich syndrome Answer: D

71
Question 109 The following immunodeficiencies occur due to mutations on the X-chromosome except: Bruton’s agammaglobulinemia DiGeorge’s syndrome Hyper-IgM syndrome Severe combined immunodeficiency Wiskott-Aldrich syndrome Answer: B

79
Transplant rejection 79

80
Transplant rejection Hyperacute Acute Chronic (note kidney model) 80
 80")
81
Renal transplant rejection
hyperacute rejection primarily antibody-mediated preexisting antibody to donor antigens occurs within minutes of transplantation acute rejection primarily cell-mediated occurs days to months after transplantation characterized by infiltration of lymphocytes and macrophages 81

82
Renal transplant rejection
chronic rejection primarily antibody-mediated vascular damage months to years after transplantation 82

83
Histologic manifestations of cellular vs. humoral rejection
cellular rejection interstitial infiltrate of T-lymphocytes and macrophages humoral rejection endothelial injury with thrombosis and resultant coagulation necrosis 83

84
Graft versus host (GVH) disease
84

85
Graft versus host (GVH) disease
significant problem in bone marrow transplantation immunocompetent cells are transplanted can also be caused by whole blood transfusion in patients with severe combined immunodeficiency disease (SCID) 85
 85.")
86
Graft versus host (GVH) disease
rejection of ``foreign'' host cells by engrafted T and B cells CD8+ T cells from graft directly damage host cells cytokines from graft CD4+ T cells recruit macrophages which damage host cells 86

87
Graft versus host (GVH) disease
liver, skin, and gastrointestinal mucosa are principal target organs clinical features fever, rash, hepatosplenomegaly, jaundice, bloody diarrhea 87

88
Graft versus host (GVH) disease
apoptotic changes in target organs bile ducts jaundice basal layer of squamous epithelium of skin rash intestinal epithelium (distal ileum most prominent site) bloody diarrhea lymphoid tissue 88
 bloody diarrhea. lymphoid tissue. 88.")
89
Apoptotic cells in basal layer of epidermis in GVHD
89

90
Apoptotic cells in basal layer of crypts in GVHD
90

Similar presentations




















>")





 I) Anaphalactic II) Cytotoxic III) Immune Complex IV) Cell-mediated (Delayed) Autoimmune Diseases.>")

 Immunity and inflammation. the capability of the body to resist harmful microbes from entering to the body.>")









