Download presentation
Presentation is loading. Please wait.

1
Innovative Interjurisdictional Practice Models Marlene M. Maheu, Ph.D. mmaheu@telehealth.org Executive Director TeleMental Health Institute Marlene M. Maheu, Ph.D. mmaheu@telehealth.org Executive Director TeleMental Health Institute

2
Disclaimer I am an MFT and clinical psychologist, not an attorney, physician or Information Technology specialist. My goal is educational only. The information I present is my best attempt to bring you timely and relevant information in a rapidly evolving area. I therefore make no warranty, guarantee, or representation as to the accuracy or sufficiency of the information contained in my training. My goal is to outline the issues and alert you to what's happening, including legal, ethical and other risk management issues. You are encouraged to seek specific advice related to your circumstance from your qualified authorities.

3
AASCB Slides & References http://telehealth.org/aascb

4
We are retooling 2014

5
Telehealth vs. Distance Counseling (working model not to scale) Behavioral Telehealth Disciplines, including Distance Counseling, Training & Supervision TelehealthTelehealth Health Professions Education Health Professions Education Administration Evaluation Research Evaluation Research Homeland Security Public Health Public Health Consumer Education (and Self- management) Consumer Education (and Self- management) Regional Health Information Sharing Regional Health Information Sharing
 Behavioral Telehealth Disciplines, including Distance Counseling, Training & Supervision TelehealthTelehealth Health Professions Education Health Professions Education Administration Evaluation Research Evaluation Research Homeland Security Public Health Public Health Consumer Education (and Self- management) Consumer Education (and Self- management) Regional Health Information Sharing Regional Health Information Sharing.")
6
What are the Current Models for Distance Services in Counseling and Other Disciplines?

8
Traditional Behavioral Telehealth Model

9
Hub-and-spoke model – Only work with previously identified clients/patients who have had an in-person assessment – Detailed and documented referral requests – Detailed health record at fingertips of clinician – Client/patient is at the “originating site” – Clinician is at the “distant” site – Community collaborator is available Client/patient is pre-trained by staff Technology is stable – IT staff is available during entire time of connection to client/patient

10
Online Norm vs. Traditional Behavioral Telehealth (or Telemental Health) Traditional Online Therapy Mostly Email & Chat Anonymity Accept self-referral online Disclaim Responsibility w/ Website Disclaimers No Clear Channels for Mandated Reporting No Patient Records Traditional Behavioral Telehealth Video Verify clients/patients Rely on referrals from clinical offices Use informed consent processes/documentation Engage in mandated reporting Document as required by law 2014
 Traditional Online Therapy Mostly & Chat Anonymity Accept self-referral online Disclaim Responsibility w/ Website Disclaimers No Clear Channels for Mandated Reporting No Patient Records Traditional Behavioral Telehealth Video Verify clients/patients Rely on referrals from clinical offices Use informed consent processes/documentation Engage in mandated reporting Document as required by law")
11
Online Norm vs. Traditional Behavioral Telehealth (or Telemental Health) Traditional Online Therapy No Contact with Other Treating Clinicians No Authentication of Consumer / Professional No Emergency Backup Procedures Misunderstanding of Clinical Processes (suicide) Scant Research for Unsupervised Settings Traditional Telemental Health Obtain signed releases and collaborate Verify identify of both Consumer and Professional Establish emergency backup plan and personnel prior to delivering care 2014
 Traditional Online Therapy No Contact with Other Treating Clinicians No Authentication of Consumer / Professional No Emergency Backup Procedures Misunderstanding of Clinical Processes (suicide) Scant Research for Unsupervised Settings Traditional Telemental Health Obtain signed releases and collaborate Verify identify of both Consumer and Professional Establish emergency backup plan and personnel prior to delivering care")
12
Levels of Security General Telepractice Licensure Issues 2014

13
Inter-jurisdictional Practice Licensing Boards that may assert jurisdiction: The one in the professional’s state(s) of licensure The one in the client/client’s state of location at time of call Both Safest Practice: Provide services only where licensed Require client to attest to his or her location on every call 2014
 of licensure The one in the client/client’s state of location at time of call Both Safest Practice: Provide services only where licensed Require client to attest to his or her location on every call 2014")
14
Inter-jurisdictional Practice (cont.) Special telehealth and in many cases, “telemedicine” laws have led the way Prescription-writing initiatives led to development of laws in the 90’s Reimbursement practices for Medicare 7 Medicaid 32 states now mandate in-person assessment prior to distance contact Special informed consent laws also rapidly evolving Regulatory Case Oklahoma case of Dr. Trow No in-person assessment No informed consent No HIPAA-compliant technology (he used Skype) 2014
")
15
Licensure Requirements for Professional Counselors – 2014 What’s New for 2014 (page 4)
")
16
Licensure Requirements for Professional Counselors – 2014 What’s New for 2014 (page 4)
")
17
Levels of Security Specific Telepractice Licensure Models 2014

18
Special Telehealth Licenses or Certificates Licenses could allow an out of state provider to render services via technology in a foreign state, or it allows a clinician to provide services via telehealth into a state if certain conditions are met (such as agreeing that they will not open an office in that state.) http://www.fsmb.org/pdf/grpol_telemedicine_licen sure.pdf
 sure.pdf")
19
States with Laws Mandating Private Insurance Coverage of Telemedicine

20
Special Telehealth Licenses or Certificates Alabama Louisiana Minnesota Montana Nevada http://www.fsmb.org/pdf/grpol_telemedicine _licensure.pdf New Mexico Ohio Oregon Tennessee Texas

21
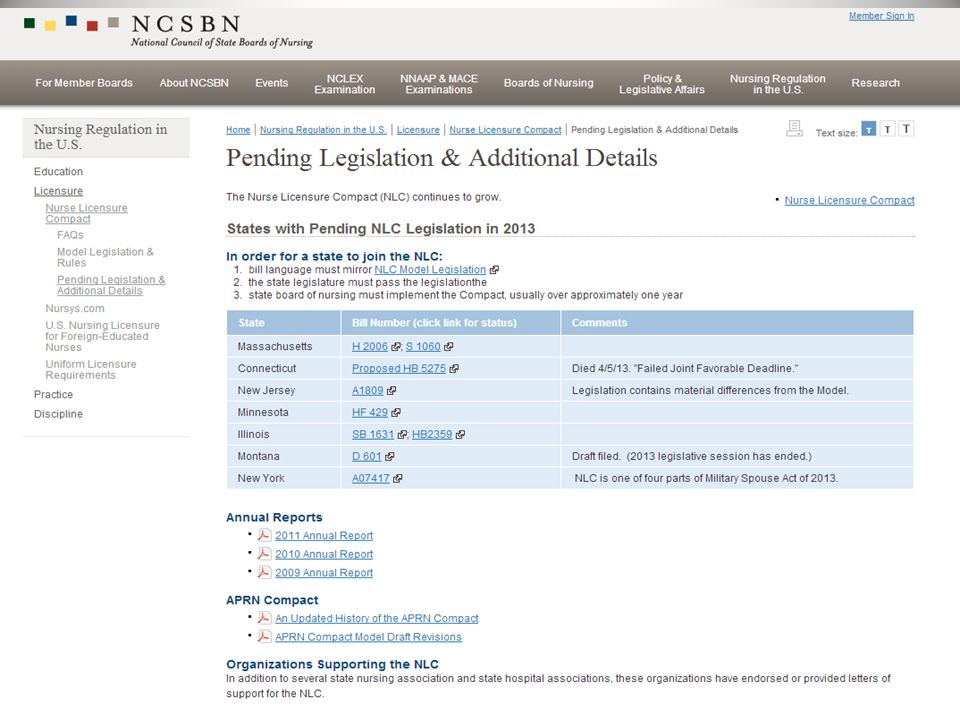
Innovative Models National Council of State Boards of Nursing (NCSB) National Council of State Boards of Nursing Federation of State Medical Boards (FSMB) Federation of State Medical Boards Association of State and Provincial Psychology Boards (ASPPB) Association of State and Provincial Psychology Boards
 National Council of State Boards of Nursing Federation of State Medical Boards (FSMB) Federation of State Medical Boards Association of State and Provincial Psychology Boards (ASPPB) Association of State and Provincial Psychology Boards")
22
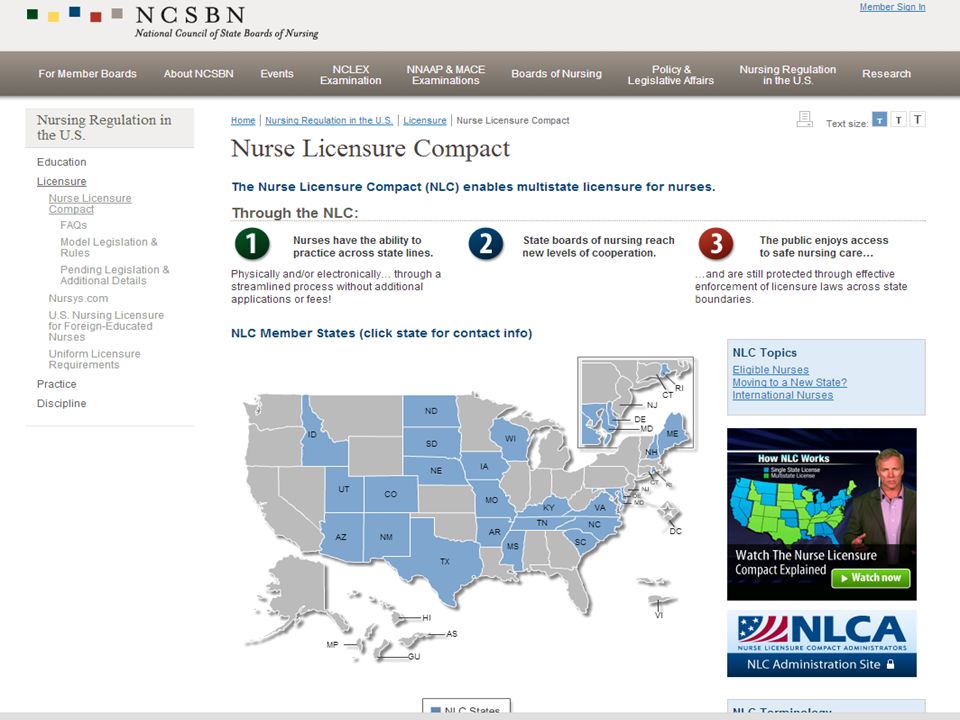
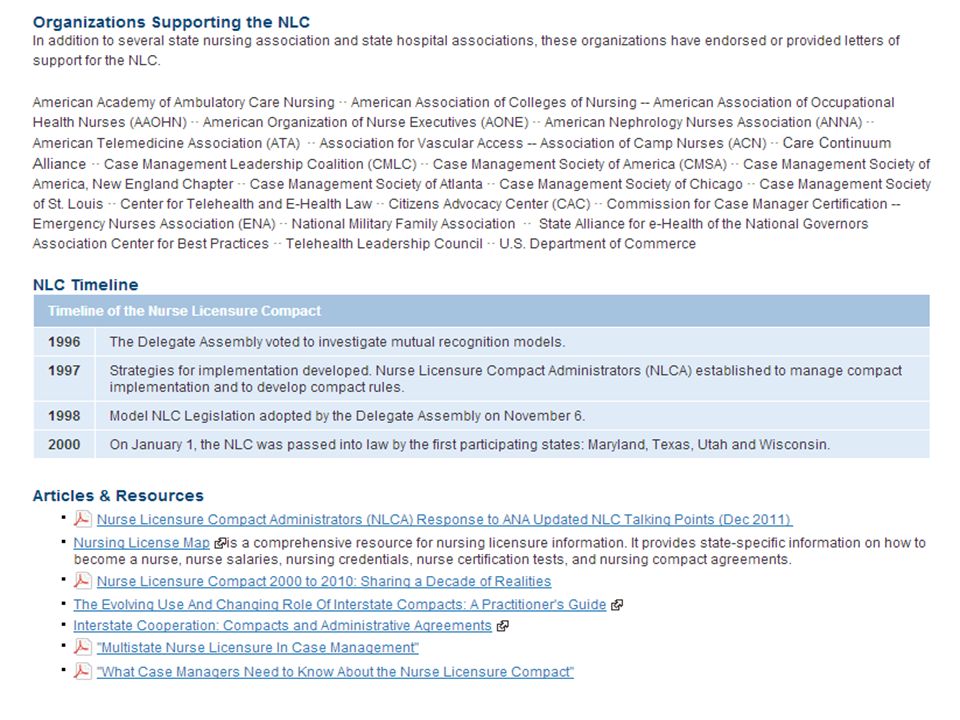
History of Licensure Portability 1996 – Telecommunications Act of 1996 - Congress urged the health care industry to develop multi-state licensure models – US Federal Communications Commission 2000 – National Council of State Boards of Nursing (NCSBN) instituted the Nurse License Compact (NLC)
 instituted the Nurse License Compact (NLC)")
23
Nurse Compact Developed upon the water rights precedent shared by states. Within states that have signed the compact, any licensed nurse can apply for a multistate license and practice nursing in all of the included states.

30
Association of State and Provincial Psychology Boards Association of State and Provincial Psychology Boards (ASPPB) (continued)
 (continued)")
31
Preferred Model Seem to be Compact - Association of State and Provincial Psychology Boards (ASPPB) – Received $350k grant for 3 years – Decided on “E.Passport” model – Running into difficulties – Now are working with other groups to develop a collaborative model across disciplines
 – Received $350k grant for 3 years – Decided on E.Passport model – Running into difficulties – Now are working with other groups to develop a collaborative model across disciplines")
32
Levels of Security Collaborative Model 2014

33
Collaborative Effort Movement toward collaboration was inspired and is being organized by Bill Hatherill, CEO of Federation of Boards of Physical Therapy Organizing CEOs of regulatory associations to approach states to help work with states Working with National Governors Association ASPPB is meeting in January with Federation of Association of Regulatory Boards (FARBS) and other groups Focus of ASPPB Meeting: – What does it take to establish a compact? – How to best move in conjunction with other disciplines to approach state boards?

34
Collaborative Effort Talking about compacts and endorsement programs – Endorsement--Where individual practitioner shows they have meet the standard and then convince states to accept credential – Compacts – reciprocal – Nursing – no real way to work around disciplining model – Follow rules in state of citizen, have to agree with comply with hearing and a both boards will impose fine, and practitioner would lose e.passport everywhere – Can’t take base license away – Up to home state to impose other sanctions on practitioner for base license

35
Levels of Security Licensure Portability Legislation 2014

36
Federal Proposals State Boards are Active Federal (proposals recognize that Congress has power to regulate interstate health commerce.) 1.STEP ACT (2011): allows DoD providers with a single state license to deliver services across state lines for the military
 1.STEP ACT (2011): allows DoD providers with a single state license to deliver services across state lines for the military")
37
STEP ACT STEP ACT is the Servicemembers’ Telemedicine & E-Health Portability Act, which expanded the already existing DOD state licensure exemption for health care professionals treating DOD clients.

38
TELEmedicine for MEDicare Act, 2013 HR 3077, the “TELE-MED Act” was introduced Sept. 10 in the House by Reps. Devin Nunes, R-Calif., and Frank Pallone, D-N.J. Nicknamed the TELE-MED Act, seeks to update current licensure laws for Medicare beneficiaries, the number of whom is expected to rise to 81 million by 2030

39
TELEmedicine for MEDicare Act, 2013 In the case of a Medicare participating physician or practitioner who is licensed or otherwise legally authorized to provide a health care service in a State, such physician or practitioner may provide such a service as a telemedicine service to a Medicare beneficiary who is in a different State, and any requirement that such physician or practitioner obtain a comparable license or other comparable legal authorization from such different State with respect to the provision of such health care service by such physician or practitioner to such beneficiary shall not apply. If passed, the bill will give licensing or authorizing states enforcement powers and require the Secretary of the Department of Health & Human Services to solicit input from “relevant stakeholders” in order to provide telemedicine guidance for states.

43
Levels of Security Resources 2014

47
TMHI News http://telehealth.org/newsletter-signup/ http://telehealth.org/newsletter-signup/

48
TeleMental Health Institute, Inc. Send email to: info@telehealth.org info@telehealth.org Visit website: www.telehealth.org

Similar presentations