Download presentation
Presentation is loading. Please wait.

1
World Federation of Public Health Associations Conference Istanbul, Turkey, April 28, 2009 J. Warren Salmon, Ph.D., Visiting Professor University of Sharjah College of Pharmacy; Professor of Health Policy & Administration University of Illinois at Chicago School of Public Health The Multinational Pharmaceutical Industry Drug Development in its Political Economic Context

3
Major U.S./E.U. Multinational Brand Firms Pfizer/Wyeth GlaxoSmithKline plc Eli Lilly & Co. Abbott Laboratories Boehringer Ingelheim GmbH Bristol-Myers Squibb Co. Novo Nordisk A/S Amgen Merck & Co/Schering-PloughMerck & CoSchering-Plough Organon Roche/GenentechRocheGenentech Sanofi-Aventis Novartis Japanese industry Israeli and Indian generic firm diversifications

4
U.S. General Situation Growing awareness of drugs and their costs, specific PHRMA firms and high profits, political influence, and world ’ s disease burden American citizens want relief from the burden of double-digit inflationary cost of medications Inability of a growing populace who cannot afford to buy their medications without other sacrifices Public knowledge of lots of specific drugs from DTC advertising and now pronounced concern over drug safety in post-Vioxx era New perspective from payers and patients with respect to the drug manufacturers—price, safety, efficacy, appropriateness, comparative effectiveness Medication errors and pharmacovigilance finally being acknowledged, though much more needs to be done

5
Drug development is not pure science What entities are developed recently? Name curative drugs? Chronic degenerative entities taken for a lifetime Mass market numbers R&D costs versus profits Blockbuster drugs versus budgetbusters RX firm Revenues -- R&D costs (25%) -- Promotion (25%) -- ???? ___________________ Profits (25%-40%)
 -- Promotion (25%) -- . ___________________ Profits (25%-40%).")
6
Manufacturing expenses Personnel, plant and equipment ??? Ingredient costs (10%-15%)
")
7
Pipelines of drug firms? USA, Europe, Japan firms differ historically CEO Salaries related to performance?

8
Global Pharmaceutical Industry Perhaps encountering its most profound period of change since the turn of last century when corporatized. Firms faced difficulties before the world economic collapse. Western multinational PHRMA firms confined to only seven Northern hemisphere nations: U.S., Great Britain, Switzerland, Japan, France, Germany, and Sweden

9
Global Drug Market 2008 figure estimated to be $640-$650 billion, growing at a flat rate in 2008 2008 United States drug expenditures of $286.5 billion was slowest growth since 1961. Total volume of scripts (4 billion) climbed only 2.8% (a declining rate). Further decline in 2009 with uninsurance and underinsurance $17 billion for U.S. generics (PBM push with MC Part D) New introductory medicines only $441 million Pharma firms looking elsewhere for emerging markets growth
 climbed only 2.8% (a declining rate). Further decline in 2009 with uninsurance and underinsurance $17 billion for U.S. generics (PBM push with MC Part D) New introductory medicines only $441 million Pharma firms looking elsewhere for emerging markets growth.")
12
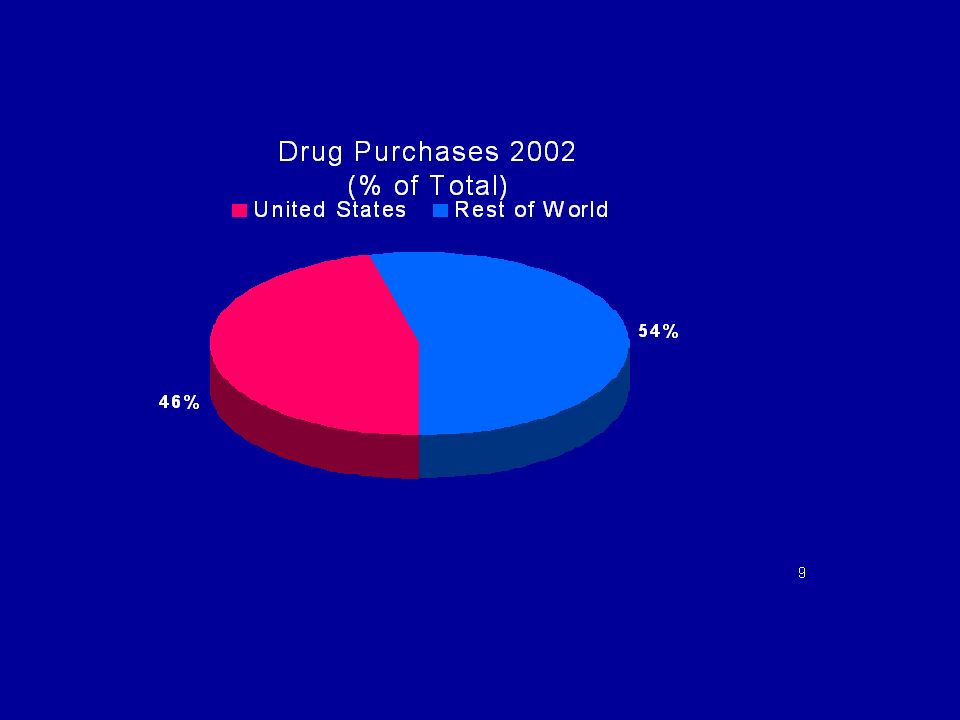
Global Drug Market Figure of $650 billion includes ethical branded drugs and biologicals (almost 80%), generic drug entities (6-9%), OTCs--NOT including natural medicines and folk remedies, which are majorly used across Asia, Africa, and Latin America U.S. consumption due to high utilization of costly branded entities unregulated as to price, unlike almost every other nation of the world where governments set the prices of drugs

13
Drug development is market- oriented Not pure science Not to serve public health needs in a country of origin nor worldwide, for sure

14
U.S. Drug consumption grew due to: More persons have a drug benefit--and use it Utilization of new and existing expensive brand drugs, even though top 3 Pharmacy Benefit Managers dispense over 50% of their prescriptions as generics (because pharmacies make higher margins on generics) New drug introductions have inflationary impact, and are always priced high. MDs are targeted with marketing Price increases annually on existing commonly used drugs (AARP study) Lack of governmental price controls (VA “best price” vs. Bush privatization for PBMs over Medicare) Obama Administration may change direction with fiscal crisis and health reforms???
 New drug introductions have inflationary impact, and are always priced high. MDs are targeted with marketing Price increases annually on existing commonly used drugs (AARP study) Lack of governmental price controls (VA best price vs. Bush privatization for PBMs over Medicare) Obama Administration may change direction with fiscal crisis and health reforms .")
15
PHARMACEUTICAL MANUFACTURERS On the Amerıcan domestic front, multinational drug manufacturers fear federal price controls, as well as further erosion of sales as large purchasers (e.g., HMOs, PBMs, hospital and nursing home chains, State Medicaid) force price reductions and substitute generics PHRMA lobbyists out number Congressmen 3 to 1 Substantial PAC contributions to both parties — $178 million lobbying in 2008, RX CEOs to Denver, Obama gets more Pharma $, PHMRA hires Democrats on staff Hard-ball restrictions on trade policies through WTO and Bilateral trade agreements (Bush administration) Will Obama administration change much???
 force price reductions and substitute generics PHRMA lobbyists out number Congressmen 3 to 1 Substantial PAC contributions to both parties — $178 million lobbying in 2008, RX CEOs to Denver, Obama gets more Pharma $, PHMRA hires Democrats on staff Hard-ball restrictions on trade policies through WTO and Bilateral trade agreements (Bush administration) Will Obama administration change much")
16
PBMs as a countervailing power? Pharmacy benefit managers profit as middlemen Marketplace “solutions” in health care rarely benefit consumers, especially the most vulnerable Nevertheless, PBM antagonisms with pharma firms have yielded socially beneficial outcomes to temper the relative power of pharma on climbing costs, marketing strategies, medication errors, drug benefit design, etc. PBMs support generic competition (patent expiries) Establish effective disease management programs Provide for head-to-head drug comparative advantage studies
 Establish effective disease management programs Provide for head-to-head drug comparative advantage studies.")
17
Bush signed Medicare Part D Drug Benefit for Seniors Projected $400 billion over ten years Or $800 billion How much for Pharma firms? PBMs favored generics

18
PHARMACEUTICAL MANUFACTURERS U.S. remains the only major nation of the world that does not regulate drug prices so U.S. has highest pharmaceutical costs Companies oppose parallel trade on the grounds that it circumvents patent laws and undermines market exclusivity for their patented drugs High profits are supposedly needed to fund Research and Development (R&D) costs in the U.S., but less expenditure than for sales promotion and sometimes profits Hard-ball restrictions on trade policies through WTO and unilateral trade agreements (Bush administration action against Thailand over compulsory licensing of Abbott Kaletra)
 costs in the U.S., but less expenditure than for sales promotion and sometimes profits Hard-ball restrictions on trade policies through WTO and unilateral trade agreements (Bush administration action against Thailand over compulsory licensing of Abbott Kaletra).")
19
Pharma dynamics What to do about patent expirations? Est. $100 billion Pipelines are scarce, failures at Phase 2, 3, and 4 Day of the blockbusters may be ending Generic competition over the world Niche markets are limited in numbers Promises of genomics, personalized medicine DTC going away??? $4 billion in spending Clinical trials costing more, multi-site Outsourcing manufacturing and clinical trials Mergers & acquisitions, alliances, co-marketing, joint ventures, and other collaborations with bio-techs

20
Prospects for Brand Drugs Drug spend across advanced economies outlandish and coming under greater control (post Vioxx safety issues) Sluggish growth due to pipelines, patents, and politics Era of the blockbuster ends with “new business models” New “high efficacy” treatments for smaller population cohorts on specific genotypes (higher per TX revenues) “Focused and virtual” R&D strategies since FDA approvals of NMEs not greatly increased lately (only a handful are truly innovative, even fewer first-in-class) R&D networks across companies, nations “Fundamental shift in industry’s operating environment”
 Sluggish growth due to pipelines, patents, and politics Era of the blockbuster ends with new business models New high efficacy treatments for smaller population cohorts on specific genotypes (higher per TX revenues) Focused and virtual R&D strategies since FDA approvals of NMEs not greatly increased lately (only a handful are truly innovative, even fewer first-in-class) R&D networks across companies, nations Fundamental shift in industry’s operating environment")
21
World pharma Market Southern hemisphere holds 80% of the world disease burden HIV/AIDS, TB, and malaria, and other neglected endemic diseases—where is pharma industry solution? Growing chronic disease patterns all over Middle class populations in emerging economies want modern medicines, but how much can afford to pay? Most multinational drug companies shifting to international markets Additionally, Avian flu, SARS, Swine flu, and new social epidemics pose major public health challenges

22
2012 Spending on Pharmaceuticals

23
Non-western Nations Resist Regulation horizons for access, cost, and safety Charitable industry (Gates, Clinton, U.N., pharma firms, Bono, Gere, Jolie and Pitt, Clooney, etc.) Trade policies are key for drugs as well as food, textiles and energy (Doha holdup with ongoing WTO negotiations) Pricing and reimbursement controls on drugs are getting tougher in several nations Bush unilateral trade pacts are an end-run against generics Brazil, India, China, South Africa, and ASEAN nations are generic strongholds and play a vital role in representing third world nations’ interests for drug access Additionally, China, Korea, Singapore, among others, are biomedical research centers (Bush stem cell policy) Generic competition and Compulsory licensing (Thailand and more)
 Trade policies are key for drugs as well as food, textiles and energy (Doha holdup with ongoing WTO negotiations) Pricing and reimbursement controls on drugs are getting tougher in several nations Bush unilateral trade pacts are an end-run against generics Brazil, India, China, South Africa, and ASEAN nations are generic strongholds and play a vital role in representing third world nations’ interests for drug access Additionally, China, Korea, Singapore, among others, are biomedical research centers (Bush stem cell policy) Generic competition and Compulsory licensing (Thailand and more)")
24
Multinational Drug firms face challenges on multiple fronts Weakening public image Drug access confrontations across the globe R&D costs, pipeline droughts High pricing and profit margins??? Drug safety and pharmacovigilance costs

25
CONCLUSION Widespread publicity on the industry has revealed the problematic of high costs and unregulated prices in the United States, thus leaving huge segments of Americans without proper pharmaceutical care Drug access is a necessary, but insufficient, answer to the health needs of those less fortunate. Infrastructure needed in delivery systems, with expanded pharmacist roles. Universal drug access, and proper and timely care, can save on significant downstream medical costs, which usually end up as public expenditure Pharma firms are under new scrutiny, and timely progressive public policy challenges must be mounted The pharmacy profession must be activist as patient and public health advocates

26
Thank you very much Professor Jack Salmon University of Sharjah COP and University of Illinois at Chicago SPH

Similar presentations



 in Transition Dr. Brian W Tempest www.briantempest.com The Global Generic Summit – Barcelona,>")












 (*)1990200020022003 Production63,127121,311158,647170,000 (e) Exports23,18089,443144,022170,000.>")


 Tighter Regulatory Controls on Clinical trials (1970s)>")