Download presentation
Presentation is loading. Please wait.

1
C. Bernie Good MD MPH Department of Veterans Affairs University of Pittsburgh CADTH 2016 April 12, 2016

2
Chair Medical Advisory Panel for Pharmacy Benefits Management, U.S. Department of Veterans Affairs Co-Director VA Center for Medication Safety FDA Drug Safety Oversight Board Member No COI with industry

3
Comprehensive health care system ◦ Direct provider of care ◦ Physicians are employees ◦ Prescription drug benefit is integrated 2014 Statistics ◦ 6.3 M veterans treated, 4.8M pharmacy users ◦ 271 million outpatient Rxes (30-day Eqv)
")
4
EMR ◦ Clinical data ◦ Pharmacy data ◦ Adverse drug events VA Center for Medication Safety ◦ Dedicated group of pharmacists, data analysts, programmers, and statisticians to support VA PBM Routinely do data monitoring, rapid cycle analyses, and full studies as indicated Work closely with FDA and other U.S. Federal Agencies

5
Drug/Drug Class IssuePotential Impact Real World VA Data Outcome or Action TZDsRosiglitazone CV Safety? 166,000 pts on TZD (2006) VA Data: Rosi > Pio for MI Rosi removed as preferred Zoster VaccineInc SAE’s in Clinical Trial ~ half VA patients >65 yo No inc in SAEs in VA patients Relaxed criteria VareniclineInc Neuropsych ADE, suicide comp NRT 24% VA smoke (17% U.S. > 18 yrs) No sig signalRelaxed criteria DOACsSafety, effectiveness v. warfarin in VA 307,000 VA pts with AF Safety, effectiveness ~ clinical trials 3 DOACs on VA formulary Hepatitis CComp. Eff; safety of meds 170,000 VA pts with HCV Real world < Clin Trials Use info for contracting EmpagliflozinComp Eff; Safety > 1M VA pts on DM Rx To Be Determined Reassess Recs
 VA Data: Rosi > Pio for MI Rosi removed as preferred Zoster VaccineInc SAE’s in Clinical Trial ~ half VA patients >65 yo No inc in SAEs in VA patients Relaxed criteria VareniclineInc Neuropsych ADE, suicide comp NRT 24% VA smoke (17% U.S. > 18 yrs) No sig signalRelaxed criteria DOACsSafety, effectiveness v. warfarin in VA 307,000 VA pts with AF Safety, effectiveness ~ clinical trials 3 DOACs on VA formulary Hepatitis CComp. Eff; safety of meds 170,000 VA pts with HCV Real world < Clin Trials Use info for contracting EmpagliflozinComp Eff; Safety > 1M VA pts on DM Rx To Be Determined Reassess Recs.")
6
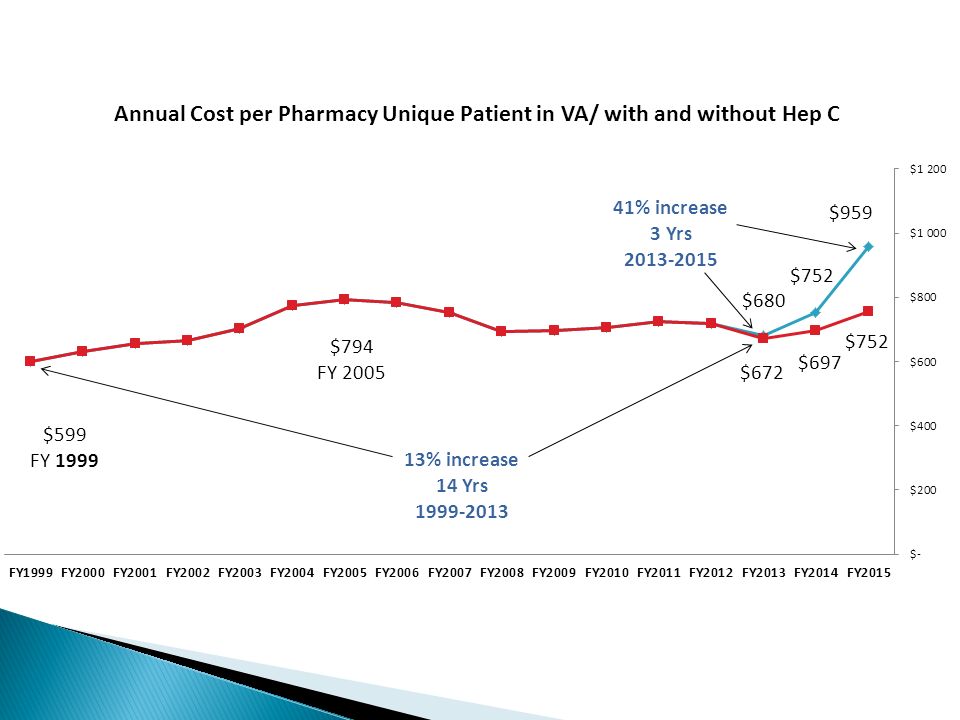
Hep C Registry: Every VA patient with HCV ◦ Genotype, viral load, prior treatment, advanced liver disease (ALD) ◦ Treatment response, adverse events, discontinuation, etc Weekly reports for new starts, by drug ◦ National, Regional, and site facility level ◦ Track new starts also by presence/absence of ALD ◦ Feedback to facilities for ALD starts, drug choice, with benchmarking Hep C data is used for contracting, CER among agents, and feedback to facilities to manage appropriateness
 ◦ Treatment response, adverse events, discontinuation, etc Weekly reports for new starts, by drug ◦ National, Regional, and site facility level ◦ Track new starts also by presence/absence of ALD ◦ Feedback to facilities for ALD starts, drug choice, with benchmarking Hep C data is used for contracting, CER among agents, and feedback to facilities to manage appropriateness")
7
> 50,000 VA Pts treated with DAA

9
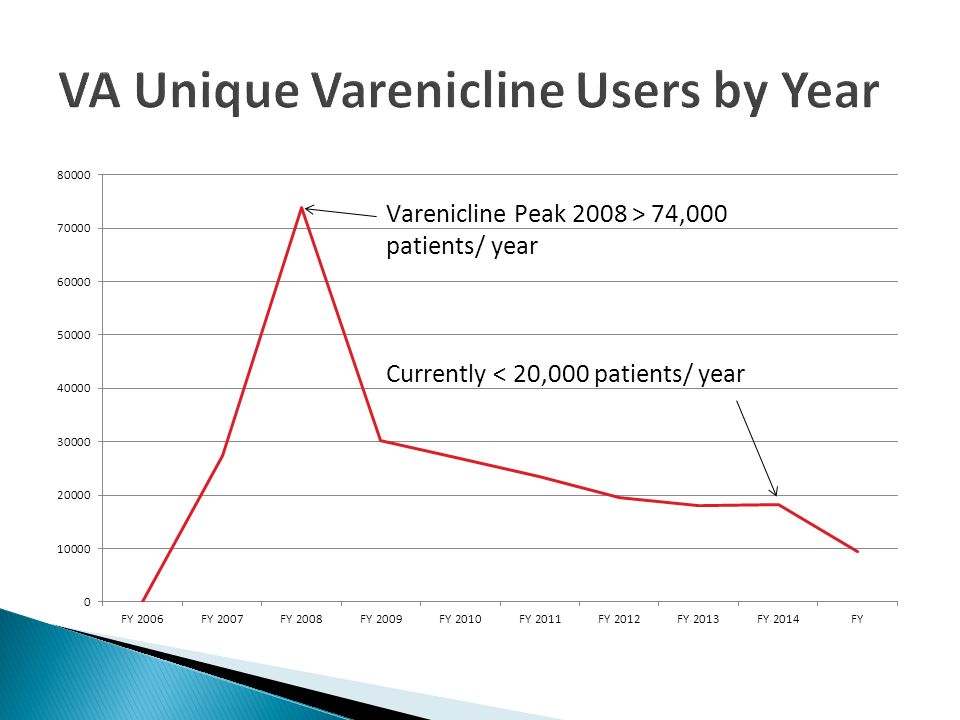
Post-marketing surveillance ◦ FDA warnings for neuropsychiatric adverse events, and suicide VA had reports of Varenicline related suicide As a result, VA developed criteria for use that restricted use of Varenicline as a third line treatment, with many safety measures Use of Varenicline dropped dramatically in VA Risk <<<< Benefit??

11
Propensity-matched study in the era *prior to FDA warnings* NRT vs. Varenicline ◦ Primary Outcome: Psychiatric adverse events Subgroups: Patients with and without psychiatric diagnoses ◦ Inpatient admissions, outpatient visits ◦ Suicide Results (pending publication) ◦ No significant increased adverse outcomes with Varenicline VA has changed criteria for use- significantly relaxed ◦ Education efforts to increase use in appropriate patients
 ◦ No significant increased adverse outcomes with Varenicline VA has changed criteria for use- significantly relaxed ◦ Education efforts to increase use in appropriate patients.")
12
DOACs- Clinical Trials: Better outcomes outcomes strongly associated with INR control in the warfarin comparison patients- for both safety and efficacy Greater patient convenience Far more expensive than warfarin VA Utilizes Pharmacy-based Anticoagulation Clinics TTR’s in VA excellent 3 DOACs on VA Formulary- does comparative effectiveness warrant significantly greater cost?

13
New user cohort, propensity matched cohort for non- valvular AF VA has done similar study, for dabigatran, rivaroxaban, and apixaban. Results show benefit >> warfarin * Graham et al, Circulation 2014 OutcomeHR (95% CI) Ischemic Stroke0.80 (0.67-0.96) Intracranial Hemorrhage0.34 (0.26-0.46) Gastrointestinal Bleed1.28 (1.14-1.44) Acute Myocardial Infarction0.92 (0.78-1.08) Death0.86 (0.77-0.96)
 Ischemic Stroke0.80 ( ) Intracranial Hemorrhage0.34 ( ) Gastrointestinal Bleed1.28 ( ) Acute Myocardial Infarction0.92 ( ) Death0.86 ( ).")
14
Real world data can inform clinical decisions ◦ Provide justification for increased expenditures based on improved clinically relevant outcomes ◦ Provide information that suggests utilization in VA should increase, based on safety and or effectiveness ◦ Provide information that drugs should be de-emphasized or removed from formulary status based on safety concerns

15
Clinical guidance Drug Monographs Criteria for use Clinical documents

18
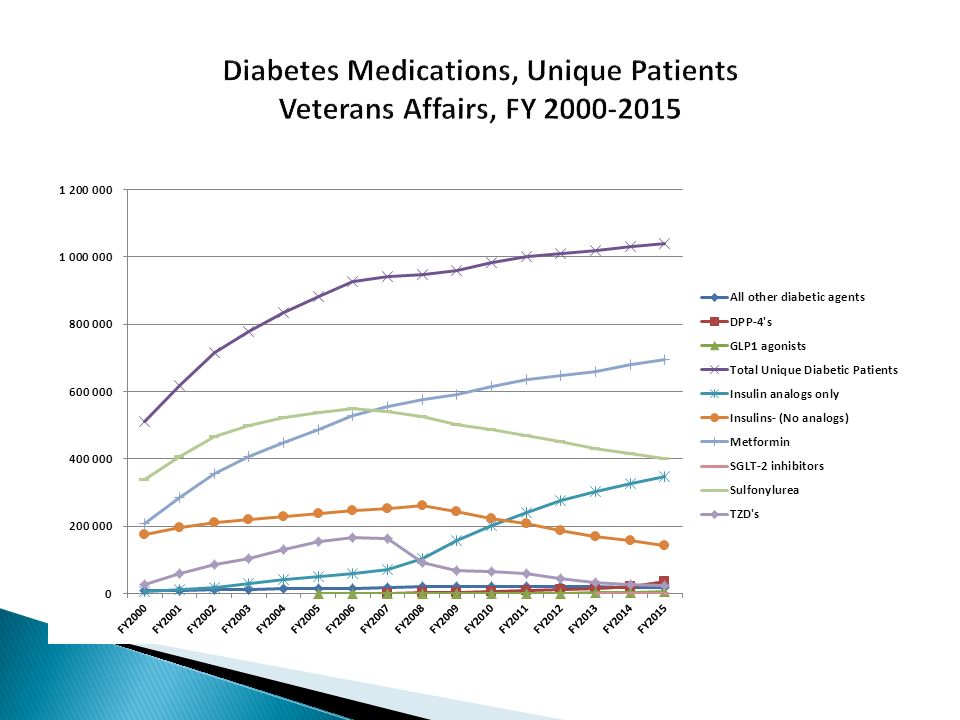
> 1 million pts with DM get medications from VA Have emphasized metformin, de-emphasized other newer oral agents without proven benefit Recent empagliflozin study indicates clinical benefit ◦ VA has added drug to our formulary with criteria for use ◦ Concerns regarding whether safety and effectiveness will be similar to clinical trial data ◦ Will monitor use of drug carefully, and track ADE, and later assess benefits

Similar presentations

















 study To reviewers and moderators: These.>")



