Download presentation
Presentation is loading. Please wait.

1
Proximal Humerus Fractures
Gregory L. DeSilva, MD

2
History/Demographics
Bimodal: young-high energy, elderly-low energy (osteoporosis) 45% of all humerus fx. elderly females 4:1 over males 77% of all prox. hum. fractures female
 45% of all humerus fx. elderly females 4:1 over males. 77% of all prox. hum. fractures female.")
3
Consequences/Associated Injuries
Disabilities often underestimated Loss of motion Loss of reduction AVN heterotopic bone Associated Injuries rotator cuff nerve (axillary, brachial plexus) vascular scapula, clavicle
 vascular. scapula, clavicle.")
4
Anatomy

5
Proximal Humeral Retroversion
35-40 degrees relative to epicondylar axis

6
Blood Supply Axillary artery ant. humeral circumflex
*ascending branch (arcuate artery) is the major blood supply to the articular surface post. humeral circumflex Arcuate Arcua afeeffe
 is the major blood supply to the articular surface. post. humeral circumflex. Arcuate. Arcua. afeeffe.")
7
Nerves Brachial Plexus axillary suprascapular musculocutaneous

8
Classification Neer 2 part SN,AN,GT,LT 3 part SN+GT or LT AN+GT or LT
neck + both tuberosities +/- dislocation Neer’s definition of displacement: >1cm or >45 degrees

9
Classification AO/OTA type A-Unifocal type B-Bifocal type C-Articular
2 part extracapsular type B-Bifocal 3 part partially intracapsular type C-Articular vascular isolation of head 4 part intracapsular

10
Classification AO/OTA type A-Unifocal type B-Bifocal type C-Articular
2 part extracapsular type B-Bifocal 3 part partially intracapsular type C-Articular vascular isolation of head 4 part intracapsular

11
Radiographic Work Up Trauma Series Other CT Scan true scapular AP
axillary (head defects, displacement of tuberosities Y or transscapular Other modified axillary AP in int. and ext. rotation CT Scan articular fractures impression head split glenoid fractures assess tuberosity displacement for operative decision making

12
Radiographic Work Up Scapular AP, Axillary, Y view, CT Scan

13
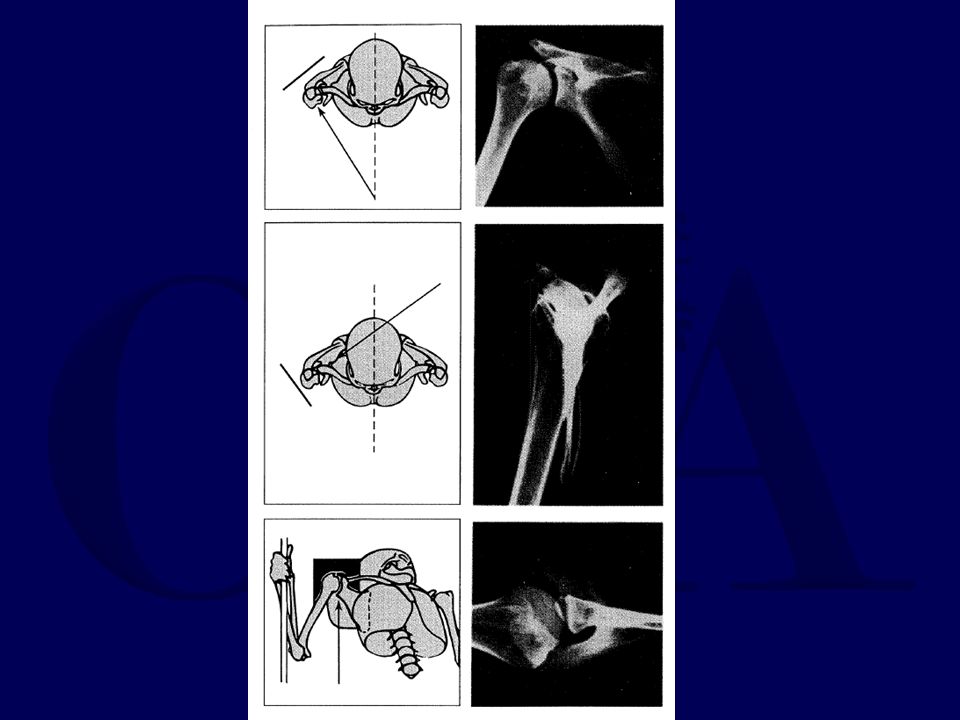
Shoulder Trauma -X-Rays

15
Avoid Missed Shoulder Dislocation
Clinical Suspicion Proper x-rays Axillary view is a must! Axillary view is mandatory! Don’t accept lack of axillary view!

16
Nothing is Dislocated until it is proven that it is dislocated!!!!!!!
Nothing is Reduced until it is proven that it is reduced!!!!!!!

17
Fractures to Consider for Closed Treatment
Minimally displaced 2 part fx’s (or positional reduction of significant displacement) GT fractures should be <5mm). Minimally displaced 3- and 4-part fractures
 GT fractures should be <5mm). Minimally displaced 3- and 4-part fractures.")
18
Fractures to Consider for ORIF
Displaced GT fx (> 5 mm) LT fx with involvement of articular surface Displaced or unstable surgical neck fx Displaced anatomic neck fx in young pt. Displaced, reconstructible 3- and 4-part fractures Polytrauma
 LT fx with involvement of articular surface. Displaced or unstable surgical neck fx. Displaced anatomic neck fx in young pt. Displaced, reconstructible 3- and 4-part fractures. Polytrauma.")
19
Fractures to Consider Hemiarthroplasty
Young/Middle age nonreconstructable articular surface (severe head split) or extruded anatomic neck Elderly many 4 parts some severe 3 parts most 3,4 part fracture dislocations most head splits
 or extruded anatomic neck. Elderly. many 4 parts. some severe 3 parts. most 3,4 part fracture dislocations. most head splits.")
20
Current Techniques of ORIF
Percutaneous Pins (Jaberg, H. 1992) Suture, K-wire, tension band technique (Cornell,C. H. 1994, Darder, A. 1993, Hawkins, J.R. 1987, Neer, C.S. 1970) Flexible IM nails (Lee, C. K. 1981, Robinson, C. M. 1993, Wesley, M. S. 1977) Buttress Plates (Esser, R. D. 1994, Kristiansen, B. 1986, Paavolainen, P. 1983, Savoie, F.H. 1989) Selected Locked Rigid IM nails Blade Plate Fixation (Weber 1984, Sehr, Szabo 1988, Jupiter, Scheid 1999) Proximal Humeral Locking Plates
 Suture, K-wire, tension band technique (Cornell,C. H. 1994, Darder, A. 1993, Hawkins, J.R. 1987, Neer, C.S. 1970) Flexible IM nails (Lee, C. K. 1981, Robinson, C. M. 1993, Wesley, M. S. 1977) Buttress Plates (Esser, R. D. 1994, Kristiansen, B. 1986, Paavolainen, P. 1983, Savoie, F.H. 1989) Selected Locked Rigid IM nails. Blade Plate Fixation (Weber 1984, Sehr, Szabo 1988, Jupiter, Scheid 1999) Proximal Humeral Locking Plates.")
21
Percutaneous Pinning Associated Problems: nerve injury (axillary), pin loosening, migration, no early motion Best Use: limited 2 or 3 part when other techniques not favorable Migration----

22
Suture or K-wire/Tension Band
Best Use: GT, LT, GT+LT, tuberosities with undispl. SN

23
Flexible Nails Best use: 2 part SN
Newer plates and nails more favorable

24
Locked Rigid Nails for Proximal Humerus
enhanced proximal fixation with twisted blades or multiple screws

25
PROXIMAL HUMERAL LOCKING PLATE

26
PROXIMAL HUMERAL PLATE

27
PROXIMAL HUMERAL

28
Hemiarthroplasty Associated Problems: unpredictable results from function standpoint, still requires bony healing (of tuberosities) Best use: elderly 3,4 part, head splits, dysvascular AN

29
Complications Misdiagnosis degree of GT displacement
missed post. Dislocation massive rot. cuff avulsion with high energy dislocation. Suspect when severe swelling head split (double shadow) best seen on axillary v. or CTS
 best seen on axillary v. or CTS.")
30
Complications Nonunion
In young, treat like an acute fracture if head viable. Consider hemiarthroplasty in elderly or osteoporotic.

31
Complications Adhesive Capsulitis AVN
Significant incidence in 3 and 4 part fractures. Higher when treated with ORIF. Unlike hip, incidence does not correlate directly with symptoms. Can be minimized with decreased soft tissue stripping and no encroachment of circumflex/arcuate art. Adhesive Capsulitis almost universal but minimized with early motion controlled P.T. manipulation under anesthesia occasional arthroscopic release

32
Summary Challenging fractures Get proper x-rays
Axillary view is a must Don’t miss a fracture-dislocation! Neer vs. AO/OTA classification AVN Osteoporosis/insufficiency fx Poor ROM

Similar presentations







, FRCS, D’ORTH, Dip ATLS FELLOWSHIP SHOULDER SURGERY(MANCHESTER) FELLOWSHIP HAND SURGERY(LIVERPOOL)>")







>")



