Download presentation
Presentation is loading. Please wait.

2
Cardiovascular Risk Factors Non-modifiable – Age – Gender – Family History Modifiable – Hypertension – Smoking – Diabetes – Hyperlipedemia – Other: Homocystine levels CRP levels Sedentary life style obesity

3
Cardiovascular Evaluation History Blood Pressure Pulse Auscultation CXR EKG Stress EKG Scintigraphy – Thallium Echocardiograms Angiography

4
Exercise Stress Testing Pathophysiology: – At rest, there may be adequate coronary blood flow, with exercise, supply may not keep up with demand leading to characteristic ST segment changes and other end points due to obstruction. – At least a 70-80%occlucions is needed before coronary stenosis (obstruction) is reliably detected by this test. – Significant coronary artery disease can exist with a negative Exercise Stress Test.
 is reliably detected by this test. – Significant coronary artery disease can exist with a negative Exercise Stress Test..")
5
Indications for Stress Testing Evaluation of patients with suspected coronary artery disease (CAD). – Typical Angina Pectoris – Atypical Angina Pectoris Evaluation of patients with known coronary artery disease (CAD). – After myocardial infarction – After intervention Evaluation of exercise capacity Evaluation of cardiac rhythm disorders
. – After myocardial infarction – After intervention Evaluation of exercise capacity Evaluation of cardiac rhythm disorders.")
6
Preparation for Stress Testing History – Type, character, durations, radiation, position of chest pain – Factors that increase or decrease chest pain – Associated symptoms i.e. SOB, Diaphoresis, leg pain, etc – Other illnesses: - HTN, DM, COPD, >lipids, CNS disease, Physical Limitations – Medications – General Activity level

7
Preparation for Stress Testing Physical Examination – General appearance, gait and mobility – Cardiac auscultation and palpation – Pulmonary Exam – Vascular- bruits, pulses – Musculoskeletal – limb strength and mobility Laboratory Studies – Screening chemistry and hematologic profiles – Resting ECG

8
Contraindications to Stress Testing Acute myocardial infarction or unstable angina Acute cardiac inflammation, pericarditis, endocarditis, or myocarditis Severe congestive heart failure Uncontrolled sustained ventricular arrhythmias, symptomatic supraventricular arrhythmias or high-grade block Hemodynamically significant aortic stenosis

9
Contraindications to Stress Testing Severe hypertension (>200/>100) Active thromboembolic processes within past 3 months – Pulmonary embolism – Deep vein thrombosis Poor candidate for exercise Extreme obesity, i.e. Exceeds equipment capacity, usually can’t do over 350 lb. Severe mental or physical disabilities

10
Possible Contraindications to Stress Testing based on Resting ECG ST-segment changes 1 mm or greater, either depression or elevation Ventricular strain patterns or hypertrophy T-wave inversions Left bundle branch block Right bundle branch block, if significant Prolonged QT interval

11
Equipment for Stress Testing Treadmill or bicycle or steps ECG machine Blood Pressure Cuff Computer is a ‘nice to have’ ACLS Certification Exit Strategy Good Help* (it takes two to test)
")
13
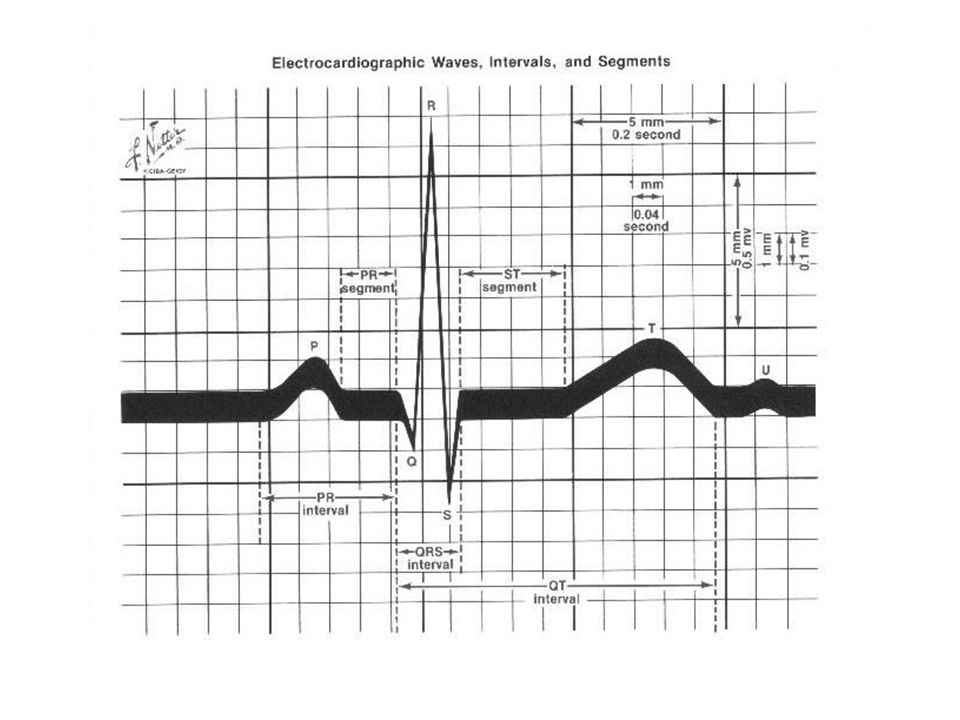
Normal ECG

14
Normal Response to Stress Testing 1)Heart rate increases 2)Blood pressure increases 3)Cardiac output increases 4)Total peripheral resistance decreases 5)Dysrhythmias – isolated unifocal PVC’s and PAC’s not of concern, usually suppressed at increased heart rate 6)Oxygen consumption increases (1MET = 3.5 ml O2/Kg./min = 1 metabolic equivalent)
Heart rate increases 2)Blood pressure increases 3)Cardiac output increases 4)Total peripheral resistance decreases 5)Dysrhythmias – isolated unifocal PVC’s and PAC’s not of concern, usually suppressed at increased heart rate 6)Oxygen consumption increases (1MET = 3.5 ml O2/Kg./min = 1 metabolic equivalent)")
15
Abnormal Response to Stress Testing 1)Heart rate fails to rise above 120 or unable to attain target heart rate of 85% of max 2)Blood pressure shows a drop in systolic 3)Patient physically unable to complete test 4)Marked hypertension, >260/115 5)Chest Pain and/or unusual shortness of breath
Heart rate fails to rise above 120 or unable to attain target heart rate of 85% of max 2)Blood pressure shows a drop in systolic 3)Patient physically unable to complete test 4)Marked hypertension, >260/115 5)Chest Pain and/or unusual shortness of breath")
16
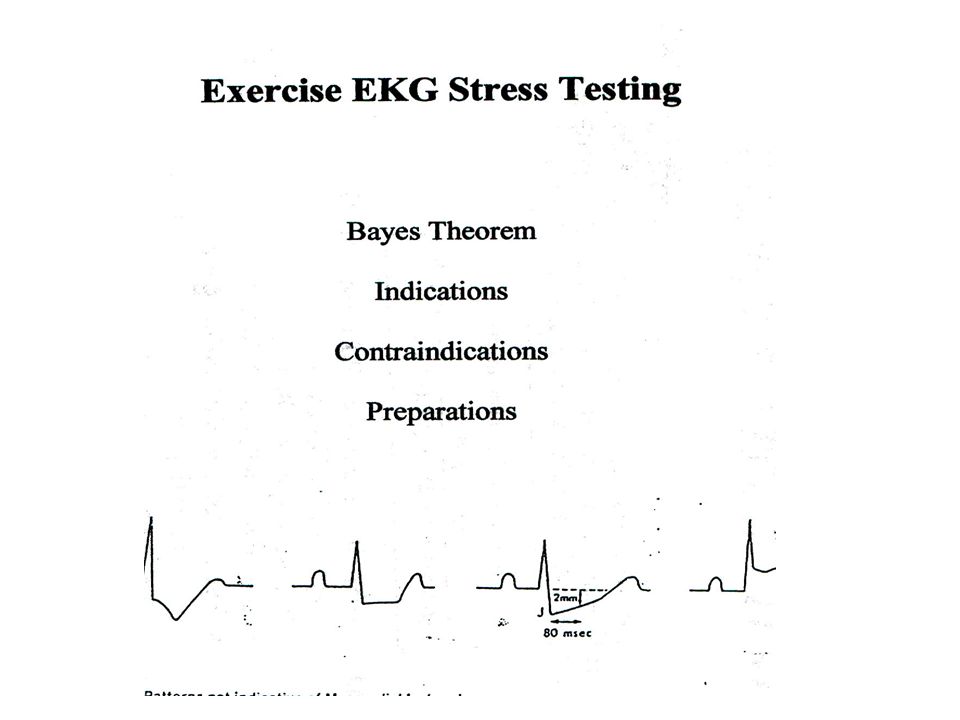
Normal ECG Response to Stress Testing 1)ECG Changes 1)QRS complex decreases in size 2)J point depresses, resulting in up sloping of ST segment 3)ST segment returns to baseline by 80 milliseconds 4)PR segment may down slope – thus baseline is defined as PQ junction 5)R amplitude may decrease at rates that go above 130 6)T wave decreases
ECG Changes 1)QRS complex decreases in size 2)J point depresses, resulting in up sloping of ST segment 3)ST segment returns to baseline by 80 milliseconds 4)PR segment may down slope – thus baseline is defined as PQ junction 5)R amplitude may decrease at rates that go above 130 6)T wave decreases")
18
Abnormal ECG Response to Stress Testing ECG Changes Horizontal or down sloping ST segments ST segment depressed or elevated ST segment does not return to baseline by 80 milliseconds U or T wave inversion Dysrhythmias – rate dependent blocks above first degree, WPW appears, Atrial fib/flutter, multiform and/or increasing PVC’s, V-tach occurs

19
Protocols EST’s utilize standard protocols to progressively increase cardiovascular work load in a uniform and reproducible manner. Work load is expressed in METS (1 MET = 3.5ml O2 /Kg/min). – 1 MET (3.5 ml) = basal O2 requirement – 5 METS (17.5 ml) = activities of daily life – 13 METS (45.5 ml) = good work out and excellent prognosis Myocardial O2 consumption is estimated by multiplying HR by BP to obtain the ‘double product’. – Double product < 20,000 is low heart work load – Double product > 29,000 indicates high heart work load
. – 1 MET (3.5 ml) = basal O2 requirement – 5 METS (17.5 ml) = activities of daily life – 13 METS (45.5 ml) = good work out and excellent prognosis Myocardial O2 consumption is estimated by multiplying HR by BP to obtain the ‘double product’. – Double product < 20,000 is low heart work load – Double product > 29,000 indicates high heart work load.")
20
Reasons to Terminate Test Absolute – Patient requests to stop – Technical/mechanical difficulties – Suspected MI – CNS symptoms – Serious dysrhythmias – Drop in systolic BP – Severe Angina – ST elevation > 1mm – Poor perfusion Relative – > 2mm of ST depression – Increasing chest pain – Tired or SOB – Wheezing – Claudication – SVT – SBP>260, DBP>115 – Exercise induced BBB – 85% of max predicted HR – > 15 METS – > 30,000 double product

Similar presentations



















 stress testing Standard Echocardiographic (echo) stress testing Pharmacologic.>")
