Download presentation
Presentation is loading. Please wait.

1
Comparison of Fondaparinux and Enoxaprin in Acute Coronary Syndrome OASIS-5 Presented by: Maram Mobara

2
Combined use of anticoagulant, antiplatlet and invasive strategy in high risk patient with ACS reduce the ischemic event but also increase the risk of bleeding The search to look for future therapies that preserve or enhance the benefits without increase bleeding

3
Drug information Fondaprinux (Arixtra) First Pentasaccharide Anticoagulant prophylaxis of DVT that could lead to PE in patients undergoing hip fracture surgery, hip replacement surgery, and knee replacement surgery. Fondaparinux exerts its anticoagulant effect solely via antithrombin-III mediated neutralization of factor Xa and is devoid of IIa inhibition.

4
Enoxaprin(LMWH) Fibrinolytic Agents Anticoagulants antithrombin-dependent Both are eliminated by kidney
 Fibrinolytic Agents Anticoagulants antithrombin-dependent Both are eliminated by kidney")
5
Demonstrate the noninferiority of fondaparinux as compared with enoxaparine at 9 days To determine weather the fondaparinux was superior to enoxaparin in prevention major bleeding Follow up : 90 – 180 days Objectives

6
Study design

7
OASIS-5 Randomized study,, double blinded,, double dummy 20078 patients from 576 center in 41 countries included

8
Designed by the steering committee Data coordinated and managed by Population Health Research Institute, McMaster University and Hamilton Health Sciences, Hamilton, Ontario, Canada. Conducted independently by both of them. protocol was approved by respective ethics committees and regulatory bodies. F/O mini 80 days, maxi 180 Sponsored by Sanofi-Aventis, Organon and GlaxoSmithKline.

9
Sample size 20078 Enoxaprin 10021 Fondaparinux 10057

10
If < 60y both should be + ve

11
Exclusion criteria: Contraindication to LMW heparin Recent hemorrhagic stroke Indication of anticoagulants other than ACS Serum creatinine of at least 265

12
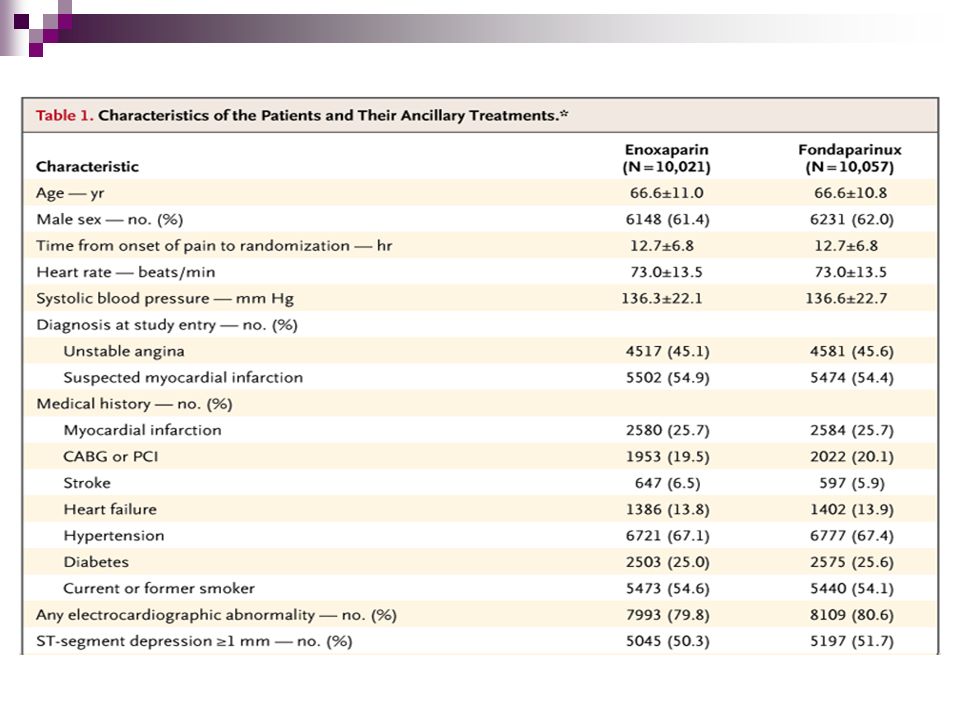
Baseline characteristics

13
Enoxaparin (n=10,002) Fondaparinux (n = 10,057) Male (%)6162 Troponin T positive or CK-MB > ULN (%) 7170 Heart failure (%)14 S/P MI (%)26 Hypertension (%)67 Diabetes (%)2526 Smoker (%)22
 Fondaparinux (n = 10,057) Male (%)6162 Troponin T positive or CK-MB > ULN (%) 7170 Heart failure (%)14 S/P MI (%)26 Hypertension (%)67 Diabetes (%)2526 Smoker (%)22")
16
Written consent Randomly assigned by central telephone system Received either : Fondaparinuxs at 2.5 mg OD + placebo of enoxaparin SC until discharge or 8 days Enoxaparin 1 mg/kg TID + placebo of fondaparinux OD for 2-8 days or clinically stable Plus standard treatment Cardiac cath could be done anytime Administration

17
Outcome Outcome

18
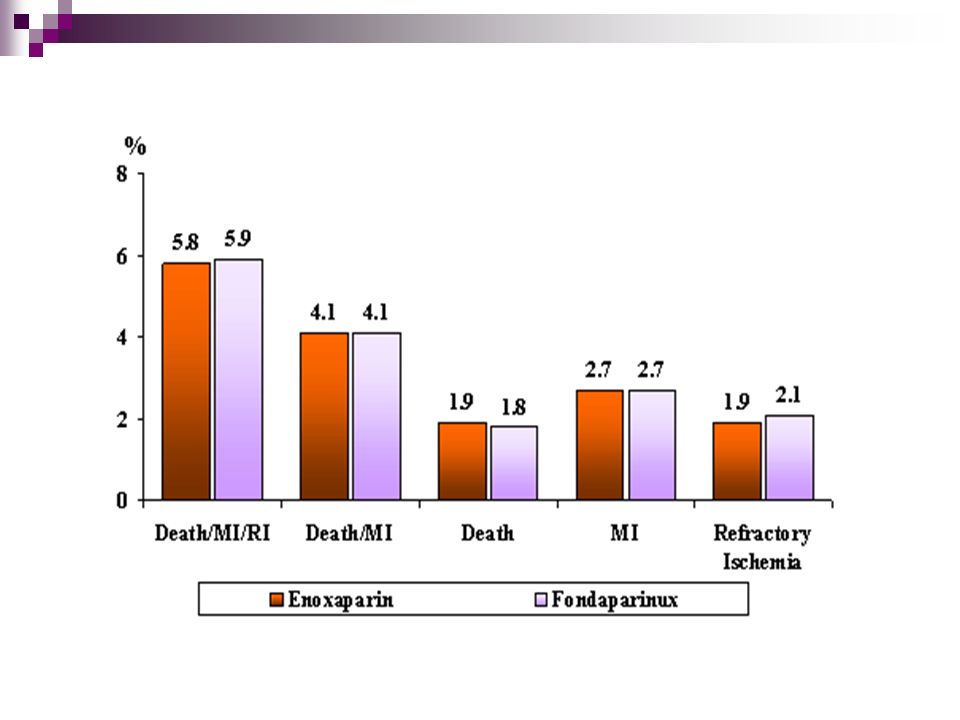
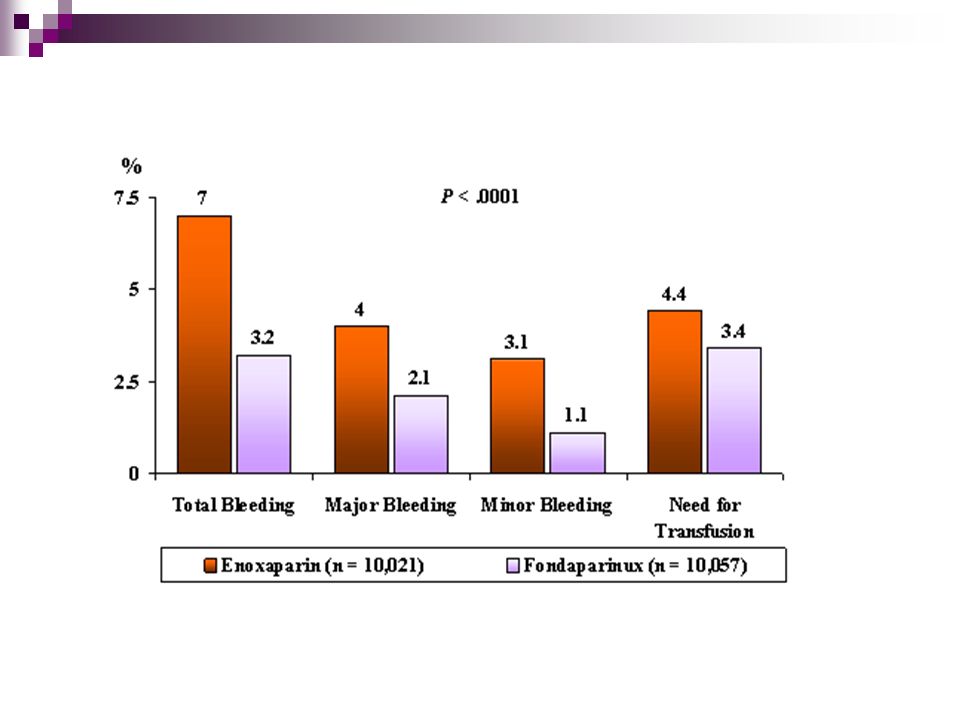
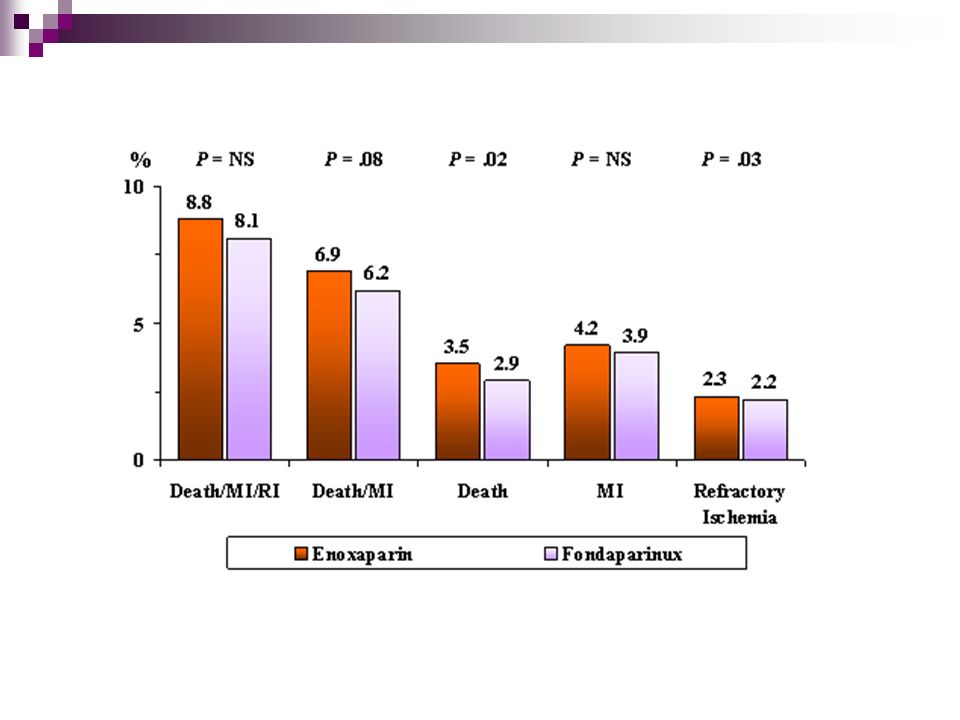
Efficacy outcome : Death, MI, Refractory ischemia Safety outcome : major bleeding at nine days. Risk benefit: Death, MI, refractory ischemia, major bleeds at 9 days Secondary: Above and each component separately at Day 30 and at 6 months The balance of benefit and risk was assessed on the basis of the combination of the primary efficacy and safety outcomes

19
OASIS- 5 definition of major bleeding clinically overt bleeding that is either fatal, symptomatic intracranial, retroperitoneal, intraocular leading to vision loss, decrease of Hb of at least 3 g/dl or bleed that requiring of > 2 U

20
This result confirms the noninferiority of fondaparinux as compared with enoxaparin because the upper confidence limit is well below the prespecified boundary of 1.185 (P=0.007 for noninferiority).
.")
27
Conclusion noninferiority of fondaparinux as compared with enoxaparine at 9 days (similar efficacy ) compared with enoxaparin, fondaparinux substantially reduces bleeding reduced bleeding that accompanies the use of fondaparinux is associated with lower long-term mortality and morbidity.
 compared with enoxaparin, fondaparinux substantially reduces bleeding reduced bleeding that accompanies the use of fondaparinux is associated with lower long-term mortality and morbidity.")
28
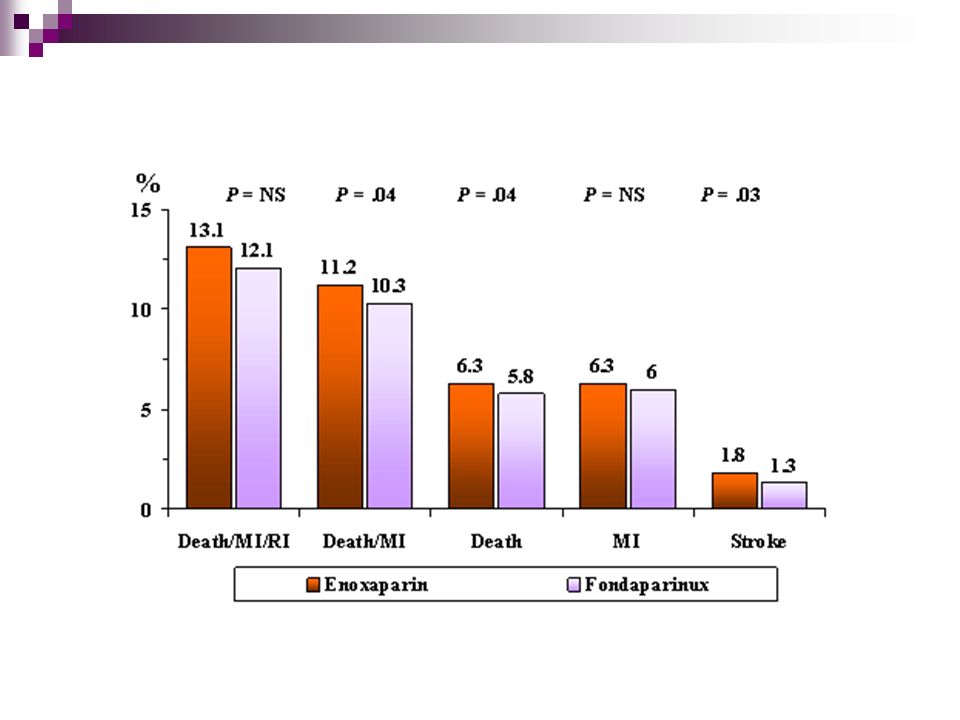
Strokes were also significantly reduced by fondaparinux. according to the results of the OASIS-5 trial, fondaparinux is the preferred anticoagulant for the treatment of acute coronary syndromes.

29
Critical appraisal

30
Validity of study 1.Randomized,, 2.double blinded,, double dummy 3. follow up 80 to 180 days 7 patients in the fondaparinux and 5 of enoxaprin were lost in the follow up by 9 days

31
4.The groups were similar at the start of study, and 5. aside from experimental intervention groups were treated equally Adherence : 99.2% in fondaparinux gp 99.4% in enoxaparin gp mean duration of tx about 5 days

32
What were the results ? Primary outcome : at 9 days ARR = 0.1 NNT = 10 95% CI ( 0.90 to 1.13 ) So, we need to treat 10 patients to prevent 1 occurrence of primary outcome over an average of 9 days
 So, we need to treat 10 patients to prevent 1 occurrence of primary outcome over an average of 9 days.")
33
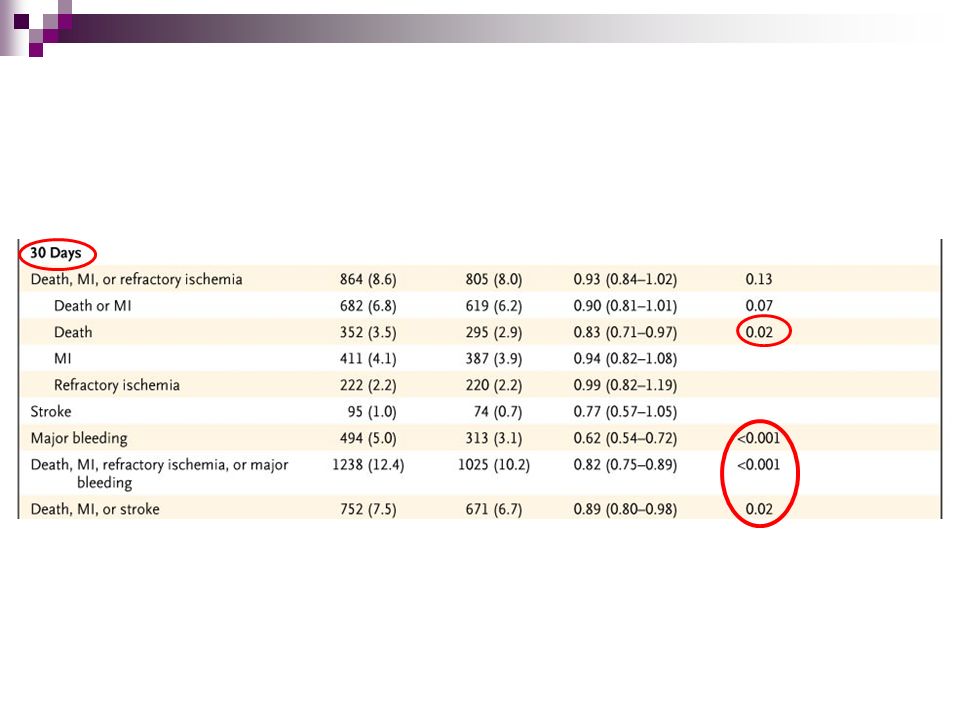
Primary outcome : at 30 days ARR = 0.6 NNT = 1.66 95% CI ( 0.84 to 1.02) So, we need to treat ~ 2 patients to prevent 1 occurrence of primary outcome over an average of 30 days
 So, we need to treat ~ 2 patients to prevent 1 occurrence of primary outcome over an average of 30 days")
34
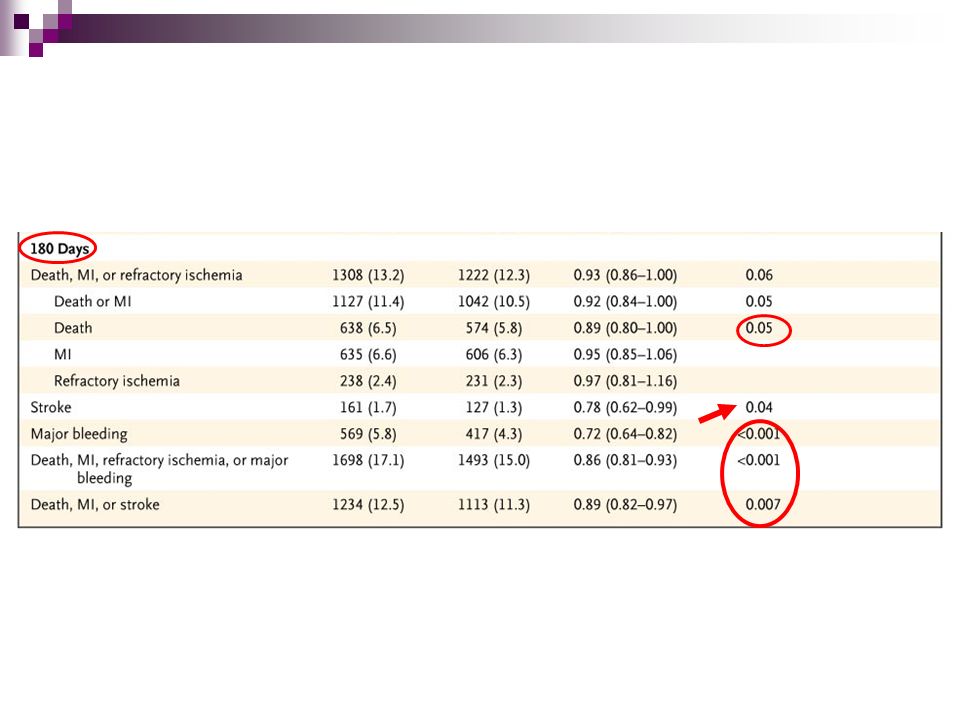
Primary outcome : at 180 days ARR = 0.9 NNT = 1.1 95% CI ( 0.84 to 1.02) So, we need to treat ~ 1 patients to prevent 1 occurrence of primary outcome over an average of 180 days
 So, we need to treat ~ 1 patients to prevent 1 occurrence of primary outcome over an average of 180 days")
35
Composite outcome :at 9 days ARR =1.7 NNT = 0.58 95% CI ( 0.73 to 0.89 ) So, we need to treat ~ 1 patients to prevent 1 occurrence of composite outcomes over an average of 30 days same figure for 30 & 180 days
 So, we need to treat ~ 1 patients to prevent 1 occurrence of composite outcomes over an average of 30 days same figure for 30 & 180 days")
36
Major bleeding : at 9 days ARR = 1.9 NNT = 0.52 95% CI ( 0.44 to 0.61; P<0.001) So, we need to treat ~ 1 patients to prevent 1 occurrence of major bleeding over an average of 9 days This difference persisted during long-term follow-up
 So, we need to treat ~ 1 patients to prevent 1 occurrence of major bleeding over an average of 9 days This difference persisted during long-term follow-up")
37
How would the result help us in caring of our patients could the results be applied to our patients ? co-morbidity, severity, prognostic factors. So, Yes I can apply it to my patients

38
Enoxaparin (n= 10,02) Fondaparinux (n = 10,057) Male (%)6162 Troponin T positive or CK-MB > ULN (%) 7170 Heart failure (%)14 S/P MI (%)26 Hypertension (%)67 Diabetes (%)2526 Smoker (%)22
 Fondaparinux (n = 10,057) Male (%)6162 Troponin T positive or CK-MB > ULN (%) 7170 Heart failure (%)14 S/P MI (%)26 Hypertension (%)67 Diabetes (%)2526 Smoker (%)22")
39
Were all clinically important outcomes considered ? death death MI refractory ischemia stroke bleeding

40
Are the likely treatment benefits worth the potential harms and costs ?

41
AE: bleeding, local irritation and asymptomatic increases in AST and ALT. ADEs occurring in greater than 5% of patients studied include:anemia, fever, nausea, edema, constipation, rash, vomiting,and insomnia. Fondaparinux is more costly than existing LMWHs; however,formal pharmacoeconomic analyses are not available. The Price of fondaparinux 2.5 mg daily is $43.50, enoxaparin 30 mg every 12 hours or 40 mg daily is $36.70 and $24.46, respectively.

42
In OASIS-5 study showed similar efficacy in primary outcome But marked benefit in decreasing risk of major bleeding Which is uncommon in the treatment of ACS, But if happened is associated with high mortality and morbidity Need of establishment of pharmacoeconomic analysis

43
Thank you

Similar presentations


 Trial>")




. Formulate Clinical Question Patient/ population Intervention Comparison Outcome (s) Women with IBS Alosetron.>")





>")


 in the prevention of venous thromboembolism after hip-fracture surgery BI Eriksson, KA Bauer, MR Lassen, and AGG Turpie.>")



