Download presentation
Presentation is loading. Please wait.

1
Spondeloarthropathy

2
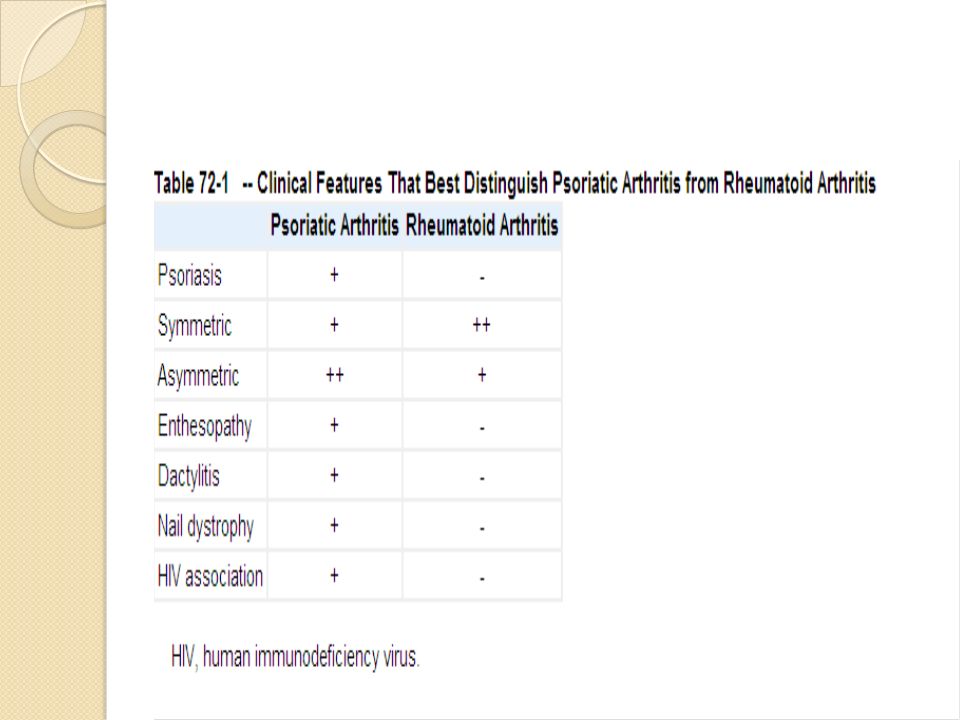
Psoriatic Arthritis

3
Psoriatic arthritis should be suspected in a patient with an asymmetric joint distribution pattern who may have additional clinical features, such as dactylitis, enthesitis, or inflammatory-type back pain, and who is negative for rheumatoid factor. In such patients, a careful search for psoriasis is warranted.

4
dactylitis

5
dactylitis

6
CLINICAL FEATURES Plaque psoriasis or psoriasis vulgaris is the most common skin phenotype in patients with psoriatic arthritis. Other patterns of skin involvement may be seen Although the arthritis usually develops in a setting of an established diagnosis of psoriasis,(80%) some patients may be unaware that they have psoriasis, or psoriasis may develop after the onset of arthritis in approximately 15% of cases. If a patient presents with the classic articular manifestations of psoriatic arthritis,
 some patients may be unaware that they have psoriasis, or psoriasis may develop after the onset of arthritis in approximately 15% of cases. If a patient presents with the classic articular manifestations of psoriatic arthritis,")
7
but does not volunteer psoriasis or the presence of a rash, it is incumbent on the physician to examine the patient’s skin carefully, including the scalp and nails because psoriasis frequently lurks in such areas. in clinical practice, there seems to be little relationship between severity of skin involvement and severity of arthritis. Patients with psoriatic arthritis present with symptoms and signs of joint, entheseal, or spinal inflammation.

8
Clinical patterns of P.A
five clinical patterns of psoriatic arthritis 1. Asymmetric oligoarthritis 2. Symmetric polyarthritis 3. Predominant distal interphalangeal (DIP) joint involvement 4. Predominant spondyloarthritis 5. Destructive (mutilans) arthritis(5%).
 joint involvement 4. Predominant spondyloarthritis 5. Destructive (mutilans) arthritis(5%).")
9
Psoriatic arthritis of the hands with phalangeal joint and nail involvement.

10
Features that are typical of psoriatic arthritis are helpful in diagnosis, including dactylitis and enthesitis. Dactylitis, in which there is a sausage-shaped swelling of the fingers or toes (may be found at first presentation, or during follow-up). Ultrasound and magnetic resonance imaging (MRI) studies have shown that joint and tenosynovial inflammation are prominent in involved digits. Enthesitis, inflammation at tendon or ligament insertion into bone, is a feature of all of the spondyloarthropathies and may be a presenting feature in psoriatic arthritis.
 studies have shown that joint and tenosynovial inflammation are prominent in involved digits. Enthesitis, inflammation at tendon or ligament insertion into bone, is a feature of all of the spondyloarthropathies and may be a presenting feature in psoriatic arthritis.")
11
Patients with enthesitis complain of pain at these sites with tenderness and sometimes swelling found on examination. Entheseal involvement may be asymptomatic, with ultrasound being more sensitive than clinical palpation. Often spurs are detected on x-ray, although spurs are not always associated with symptoms.

12
Iritis or uveitis occurs more bilateral than in ankylosing spondylitis, but usually found in patients with spinal involvement. Numerous studies have suggested that psoriatic arthritis patients have a higher prevalence of inflammatory bowel disease, sometimes asymptomatic and detected only on biopsy specimen. Whether this inflammatory bowel disease is coincidental or possibly related to medication effects remains to be clarified. Distal limb edema or lymphedema may occur more commonly in psoriatic arthritis Finally, amyloid is rare, but is described in psoriatic arthritis.

14
LABORATORY FEATURES There is no diagnostic laboratory test for psoriatic arthritis. Although the absence of rheumatoid factor is considered an important distinguishing feature from RA Until there is a more definitive diagnostic test, it is difficult to be categorical about diagnosis in these patients. Cyclic citrullinated peptide antibodies were initially thought to be specific to RA, but it is now recognized that cyclic citrullinated peptide antibodies are found in approximately 5% of psoriatic arthritis patients as well.

15
Acute-phase markers, such as ESR, C-reactive protein, or serum amyloid A, all may be elevated in psoriatic arthritis patients, but less commonly and to a lesser degree than in RA patients. These markers are elevated in particular in patients with polyarticular disease and act as a marker of poor prognosis . Finally, as mentioned previously, hyperuricemia may be found in association with metabolic abnormalities in psoriatic arthritis patients and not reflecting the extent of skin involvement.

16
TREATMENT nonsteroidal anti-inflammatory drugs are most often the agents first used in psoriatic arthritis although occasional exacerbations of psoriasis have been reported. The use of systemic corticosteroids is no evidence-based ,although 24% of patients in one study were taking prednisolone .There are concerns that exacerbations of psoriasis may follow corticosteroid withdrawal. intra-articular steroids in psoriatic arthritis or of local entheseal or dactylitis injections. intra-articular steroids is effective, especially in oligoarticular disease or where there is localized entheseal involvement, such as in plantar fasciitis .

17
sulfasalazine is used in psoriatic arthritis
sulfasalazine is used in psoriatic arthritis . Methotrexate remains for many rheumatologists the DMARD of first choice for patients with psoriatic arthritis, but evidence for its use is limited . A small, prospective randomized controlled trial concluded that methotrexate was as effective as cyclosporine, gold salts and antimalarials, there is no evidence of treatment benefit; exacerbation of psoriasis is reported, Biological agent also used in the treatment as TNF-alfa

18
Enteropthic Arthritis

19
Pathogenesis The interplay between the intestinal microflora and genetic host factors is disturbed in IBD. The microbial contribution is still largely unclear, and animal work indicates that parts of the normal gut flora may be involved. In addition, pathogenic organisms, such as Clostridium difficile, have been linked to exacerbations of IBD. genetic factors related to innate immunity are involved in susceptibility to IBD HLA-B27 is clearly one predisposing factor, but only in the minority of cases with spinal joint involvement.

20
Jejunal fluid from patients with ankylosing spondylitis (AS) and rheumatoid arthritis collected with the closed-segment endoscopic technique contained antibodies against Klebsiella pneumoniae, Escherichia coli, and Proteus mirabilis. Increased gut permeability has already been alluded to as an important factor in pathogenesis. Bacteria recovered from the gut lumen in IBD are covered by immunoglobulin, part of which is circulatory IgG.

21
CLINICAL FEATURES Spinal involvement occurs in 10% to 20% of cases. The back symptoms are often silent, so their prevalence is underestimated; they may precede the onset of IBD or appear later. In contrast to AS, there is an equal sex distribution. In general, the involvement is similar to or identical with that in classic AS, although small differences have been found. Changes in enteropathic disease tended to be milder than AS, squaring was more prevalent, . The majority of radiographic features were similar.

22
As noted, spinal involvement is often asymptomatic, but when symptoms are present, they do not correlate with intestinal symptoms as that of peripheral arthritis. The issue is complicated by the association of AS with silent Crohn's disease, as diagnosed by biopsy. Isolated sacroiliitis is not strongly associated with HLA-B27. In full-blown IBD- related AS, the prevalence of B27 is between 50% and 70%.

23
Peripheral joint disease in IBD

24
Extraintestinal manifestationof IBD

25
Pyoderma gangernosum

26
DIAGNOSIS A careful history and clinical examination, supplemented by imaging, are the principal diagnostic tools. As mentioned, genetic mapping has shown interesting clinical correlates, but genotyping is not part of the routine clinical workup at present, except perhaps for HLA-B27. Stool cultures should be performed when infection with special pathogens is suspected.

27
TREATMENT Sulfasalazine and its derivative 5-ASA which have efficacy of compared with placebo in ulcerative colitis but not in Crohn's disease. Glucocorticoids are effective in both forms of IBD, although the response of uveitis to topical therapy with glucocorticoids may be less prompt than in uveitis of other causes . Azathioprine has been widely used to maintain remission in IBD. It has proven long-term efficacy in both ulcerative colitis and Crohn's disease, according to a large European study .It should not be combined with 5-ASA owing to a pharmacokinetic interaction.

28
TNF inhibition with infliximab (but not with etanercept) results in remission of gastrointestinal manifestations in close to 60% of patients with Crohn's disease, as confirmed in several placebo- controlled studies. More recently, infliximab was found to be superior to placebo in ulcerative colitis patients resistant to conventional drug therapy, efficacy of infliximab in the treatment of pyoderma gangrenosum Pain control with nonsteroidal anti-inflammatory drugs is a potential problem owing to their potential induction of flares. However, they are widely used and often well tolerated.

29
Reactive arthritis The occurrence of enteric reactive arthritis is determined by the prevalence of exposure to triggering agents and the susceptibility of infected individuals. Therefore, incidence and prevalence figures vary among populations and over time. The risk of developing enteric reactive arthritis in exposed individuals varies from very low to 20% in different outbreaks ; it may be lower in children .The prevalence of Yersinia infections has diminished in recent years, probably as a consequence of improved slaughterhouse hygiene. Salmonella and Campylobacter are presently the two dominant causes of enteric reactive arthritis in most countries.

30
A history of urethritis (dysuria or discharge) or diarrhoea must be specifically sought for several reasons. The interval between these symptoms and the development of arthritis means that patients may not connect these apparently unrelated events. Secondly, preceding infection may be virtually asymptomatic. Chlamydia infection in women is notoriously silent, and in men these symptoms or a sexual history are often not volunteered spontaneously. Of gastrointestinal infections, salmonella is likely to produce symptoms in those who go on to reactive arthritis , whereas in yersinia-related arthritis many patients have sub-clinical or mild gastrointestinal symptoms .

31
CAUSE The triggering agents are usually gram- negative obligate or facultative intracellular organisms In most series, no organism can be identified in one quarter of patients. clearly only a small number of microorganisms have the potency to trigger reactive arthritis.

32
causes of gastroenteritis lead to reactive arthritis

33
PATHOGENESIS In enteric reactive arthritis, a triggering gut pathogen starts an inflammatory reaction in the gut; immune cells and antigenic material then disseminate into the joint. By definition, no living organisms are present in the joint after the outbreak of arthritis. Several steps in the pathogenesis remain elusive. The humoral immune response to the trigger involves secretory IgA and IgM and also IgG, and it is prolonged in comparison to patients who do not develop enteric reactive arthritis.

34
The role of HLA-B27 has been studied intensely for decades
The role of HLA-B27 has been studied intensely for decades. Some evidence indicates that it enhances the expression of proinflammatory signals, resulting in a glutamic acid located in the B pocket. In vitro experiments have shown normal cellular uptake of bacteria but delayed elimination. Ex vivo studies have identified antigenic material, in part in the form of processed lipopolysaccharid, and DNA in the joints. It is not known how this material gets into the joints.

35
Bacterial lipopolysaccharide and heat shock protein can be found in joint tissue up to 4 years after the acute episode. Carriage of HLA-B27 does not influence the duration of bacterial presence in feces in salmonellosis, and joint involvement does not correlate with carriage.

36
CLINICAL FEATURES Reactive arthritis is characterized by the acute onset of asymmetric oligoarthritis, with dominant localization to the lower extremities and often affecting the large joints Aseptic urethritis is a common feature, and the presence of circinate balanitis &Keratoderma bllenorhagica is almost pathognomonic. Enthesopathy, manifested by heel pain, is very common. Erythema nodosum is rather unusual. Unequivocal signs of synovitis are often accompanied by less distinct arthralgias, which may outlast synovitis by several months.

37
The enteritis is typically mild and may escape recognition, suggesting that a vigorous inflammatory response in the gut may provide protection against arthritis. Fever and acute-phase reactants may be low grade or intense. Self-limited glomerulonephritis, myocarditis, and conjunctivitis are other clinical features.

38
DIAGNOSIS Asymmetric, nondestructive oligoarthritis starting some weeks after mild gastroenteritis in a previously healthy individual should raise the suspicion of enteric reactive arthritis. The presence of balanitis in males is almost pathognomonic& Keratoderma blennorrhagica. Rheumatoid factor and anticyclic citrullinated peptide antibody (anti-CCP) should be negative. A triggering agent may be cultured from the stools or traced serologically in the blood. However, even a systematic search reveals a trigger in only 60% of cases. Conversely, it is not unusual to find triggers in patients without previous symptomatic disease.
 should be negative. A triggering agent may be cultured from the stools or traced serologically in the blood. However, even a systematic search reveals a trigger in only 60% of cases. Conversely, it is not unusual to find triggers in patients without previous symptomatic disease.")
39
TREATMENT Importantly, reactive arthritis cannot be prevented with aggressive antibiotic therapy, even when started early. Symptomatic analgesic treatment is usually sufficient but may be supplemented by short periods of systemic glucocorticoids or antimalarials. Short-term antibiotic therapy is usually administered if a triggering agent can be identified. The rationale for the use of antibiotics is to eradicate remaining microorganisms (e.g., Salmonella) in carriers and to prevent recurrence. However, there is no evidence that antibiotics influence the outcome.
 in carriers and to prevent recurrence. However, there is no evidence that antibiotics influence the outcome.")
Similar presentations















 is the name for a family of inflammatory rheumatic diseases that cause.>")
 Ulcerative colitis is an inflammatory bowel disease (IBD) that causes chronic inflammation of the digestive tract It is.>")


