Download presentation
Presentation is loading. Please wait.

1
Ramin Abrishami, Pharm D, BCPS

2
Infertility is defined as the inability to conceive after one year of unprotected intercourse 85% of couples with normal fertility will achieve pregnancy within one year The incidence of infertility in women: 15-29 yr: 11% 40-44 yr: 27%

3
Fecundity (probability of achieving a live birth in one menstrual cycle) is 20% for couples without infertility There is a downward trend after age 30, with fecundity rates <5% between 30-40 yr Chromosomal abnormalities and spontaneous abortion rates increases with age Male fertility is impacted by age as well, with a documented decline after age 35
 is 20% for couples without infertility There is a downward trend after age 30, with fecundity rates <5% between yr Chromosomal abnormalities and spontaneous abortion rates increases with age Male fertility is impacted by age as well, with a documented decline after age 35")
4
Tobacco: 13% of cases, worsen ovulatory function, induces chromosomal changes that alter sperm production and function Caffeine: ↓ fertility with higher levels of intake, moderate use of 1-2 cups (or equivalent) have minimal impact Alcohol: a link is not definitive→ women limit use to ≤ 1 drink/day
 have minimal impact Alcohol: a link is not definitive→ women limit use to ≤ 1 drink/day")
5
Illicit substances(ex. Marijuana): impairs fertility and ↓ success of treatments Occupational and environmental exposures: pesticides, heavy metals, and toxins (organic solvents used in dry cleaning & printing) impairs fertility
: impairs fertility and ↓ success of treatments Occupational and environmental exposures: pesticides, heavy metals, and toxins (organic solvents used in dry cleaning & printing) impairs fertility.")
6
to 40% of female infertility Thyroid dysfunction, hyperprolactinemia, PCOS can induce anovulation Signs: enlarged thyroid (thyroid dysfunction), abnormal discharge from the breast (hyperprolactinemia), or signs of hyperandrogenism or obesity (PCOS) Extremely low body weight and excessive exercise may negatively impact ovulatory function at the hypothalamic level
, abnormal discharge from the breast (hyperprolactinemia), or signs of hyperandrogenism or obesity (PCOS) Extremely low body weight and excessive exercise may negatively impact ovulatory function at the hypothalamic level")
7
Primary ovarian failure can result from exposure to chemotherapy, radiation, and ovarian surgery Aging process diminishes ovarian follicular reserve Ovarian reserve assessment is recommended >35 yr (measurement of serum FSH and/or estradiol on day 3, elevated levels suggest diminished ovarian function) Direct visualization of the ovaries through an ultrasound→ follicle count
 Direct visualization of the ovaries through an ultrasound→ follicle count")
8
Hyperprolactinemia is treated with dopamine agonists (bromocriptine) Prolactin levels should normalize after 4 wk in most patients PCOS should be treated (OCP, weight loss, metformin)
 Prolactin levels should normalize after 4 wk in most patients PCOS should be treated (OCP, weight loss, metformin)")
9
Structural abnormalities in the uterine cavity or fallopian tubes Primary or secondary (endometriosis, PID, and…) PID from STDs such as chlamydia or gonorrhea is a risk factor for tubal infertility, The risk increases with each subsequent infection and is more pronounced in older women
 PID from STDs such as chlamydia or gonorrhea is a risk factor for tubal infertility, The risk increases with each subsequent infection and is more pronounced in older women")
10
The incidence of infertility in a woman >25 yr with a history of ≥ 3 episodes of PID is 75%

11
Up to 40% of all infertilities Due to impaired sperm production or function Impaired sperm production: hypogonadism resulting from testicular trauma, radiation, cryptorchidism, or antiandrogen medications Varicoceles affect testicular function in 40% of male infertility

12
Azoospermia (Klinefelter syndrome, Pituitary tumors) Sperm transport defects result from ED, retrograde ejaculation, or obstruction of the vasdeferens or epididymis Antidepressants or antihypertensives can worsen libido and ejaculatory function Obesity → ↑ estrogen, ↓ testosterone
 Sperm transport defects result from ED, retrograde ejaculation, or obstruction of the vasdeferens or epididymis Antidepressants or antihypertensives can worsen libido and ejaculatory function Obesity → ↑ estrogen, ↓ testosterone")
13
Unexplained infertility, or no identifiable cause after evaluation, accounts for 30% of cases→ ovulation stimulation Female partner should take 400-800 mg folic acid to reduce the risk of neural tube defects

14
Ovulation Induction (OI): in patients who are not ovulating Controlled ovarian stimulation (COS): in women who have ovulatory cycles but are infertile & for procedures where the development of multiple ovarian follicles is desirable
: in patients who are not ovulating Controlled ovarian stimulation (COS): in women who have ovulatory cycles but are infertile & for procedures where the development of multiple ovarian follicles is desirable")
15
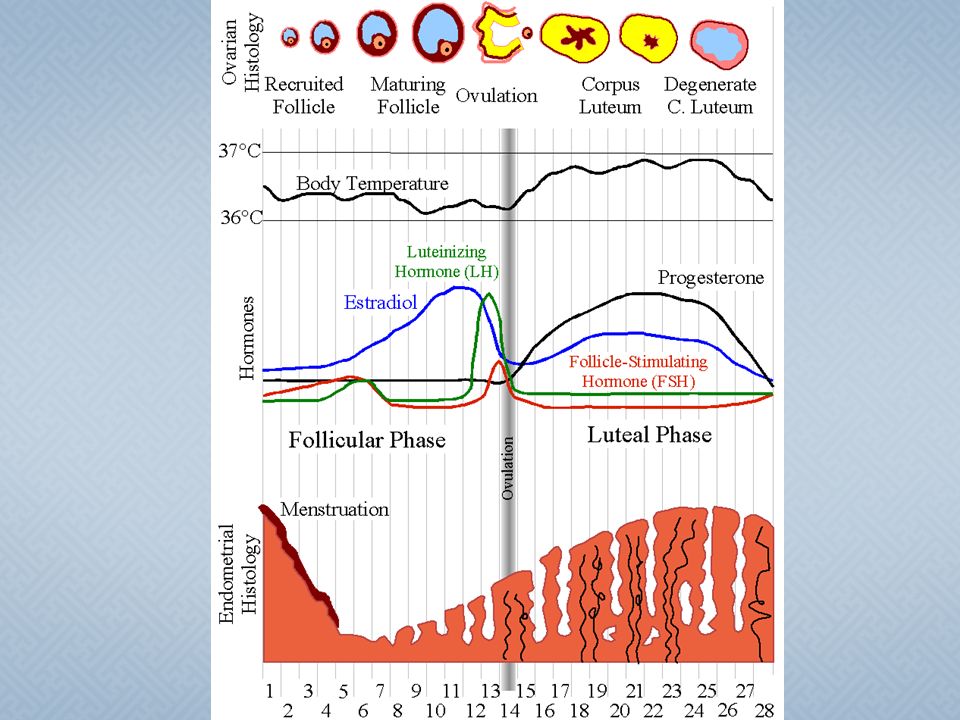
To mimic the hormonal patterns of the normal menstrual cycle FSH → initial recruitment and development of follicles early in the cycle → followed by development of a dominant follicle and increased estradiol levels → LH surge → release of the ovum

17
If adequate hypothalamic function→ oral CC, which is an estrogen agonist and antagonist Clomiphene inhibits estrogen binding in the hypothalamus to stimulate release of GnRH and pituitary gonadotropins and induce ovarian follicular development Ovulation is successful in 80% of patients using CC

18
Aromatase inhibitors are not FDA approved for OI, but increase release of GnRH & gonadotropins through an estrogen antagonist effect An alternative method of stimulating gonadotropin release is administration of gonadorelin, when administered in a pulsatile manner every 1-2 h, it induces pituitary release of FSH & LH → follicular development → inconvenient

19
If hypothalamic or pituitary dysfunction or if oral regimens are not successful→injectable gonadotropins Most common gonadotropin regimens: FSH± LH hCG is administered during the OI process to simulate the LH surge

20
"step-up" protocol: represents the natural progression of gonadotropin release during the cycle. Initial daily injections of 50 to 75 IU are increased in increments of 37.5 IU as necessary for a follicular response "step-down" protocol: higher initial daily doses of 150 IU until a dominant follicle is apparent on ultrasound. The dose is then decreased until ovulation is triggered

21
DrugBrand name hMG (menotropin) Menogon, Menopur (75 IU FSH + 75 IU LH) Urinary FSH (urofollitropin)Bravelle, Fostimon Recombinant FSH (follitropin alfa) Gonal-f Urinary hCGPregnyl
 Menogon, Menopur (75 IU FSH + 75 IU LH) Urinary FSH (urofollitropin)Bravelle, Fostimon Recombinant FSH (follitropin alfa) Gonal-f Urinary hCGPregnyl")
22
The medications are administered in doses intended to develop multiple ovarian follicles→ a greater number of oocytes available for fertilization Clomiphene citrate is the most common initial choice

23
Stimulates release of GnRH→ gonadotropin release → follicular development, increased estradiol production, and ovulation Initial dose is 50mg/d x5d starting on day 3 or 5 Ovulation occurs 5-12d after the 5 th dose If ovulation occurs but pregnancy does not occur → the same dose is used in future cycles If ovulation does not occur → the dose is increased by 50mg with each subsequent cycle, up to 250mg

24
ADR: Vasomotor symptoms (10-20%), nausea, headache, irritability, mood swings, visual disturbances, multiple gestation (8-10%) Ovarian cysts occur in 5-10% of users COS with CC: per-cycle pregnancy rate 3-8% lUI may not greatly improve pregnancy rate There is little evidence for effectiveness beyond six attempts with the combination of CC and lUI
, nausea, headache, irritability, mood swings, visual disturbances, multiple gestation (8-10%) Ovarian cysts occur in 5-10% of users COS with CC: per-cycle pregnancy rate 3-8% lUI may not greatly improve pregnancy rate There is little evidence for effectiveness beyond six attempts with the combination of CC and lUI")
25
Aromatase converts androstenedione to estrone and testosterone to estradiol Letrozole and Anastrazole They reduce estrogen levels→ ↑ gonadotropin secretion and follicular development They inhibit conversion of testosterone to estradiol → higher concentration of androgens in the ovary → increases follicular sensitivity to FSH

26
Letrozole 2.5 or 5 mg once daily x5d beginning on cycle days 3-5 Pregnancy rates are similar to that of CC ADR: vasomotor symptoms (11%), nausea and fatigue (10%), multiple gestation (less than CC),
, nausea and fatigue (10%), multiple gestation (less than CC),")
27
If oral agents are unsuccessful, COS can be attempted with injectable gonadotropins (FSH ±LH) Per-cycle conception rates are higher than that of CC or aromatase inhibitors: 21% If unsuccessful cycles of CC + lUI → switching to letrozole → pregnancy rates similar to gonadotropins without the inconvenience and cost
 Per-cycle conception rates are higher than that of CC or aromatase inhibitors: 21% If unsuccessful cycles of CC + lUI → switching to letrozole → pregnancy rates similar to gonadotropins without the inconvenience and cost")
28
ProcedureDescription IUI Delivery of a prepared semen sample into the uterus during ovulation Gamete intrafallopian transfer (GIFT) Laparoscopic transfer of the unfertilized oocytes and sperm to the fallopian tube for fertilization In vitro fertilization-embryo Transfer (IVF) Transfer of one or more embryos resulting from in vitro fertilization into the uterus through the cervix Zygote intrafallopian transfer (ZIFT) Laparoscopic transfer of the fertilized oocyte (zygote) into the fallopian tube
 Laparoscopic transfer of the unfertilized oocytes and sperm to the fallopian tube for fertilization In vitro fertilization-embryo Transfer (IVF) Transfer of one or more embryos resulting from in vitro fertilization into the uterus through the cervix Zygote intrafallopian transfer (ZIFT) Laparoscopic transfer of the fertilized oocyte (zygote) into the fallopian tube")
30
Represents an estimated 1% of live births For couples who are not candidates for OI/COS alone or lUI 37% results in a pregnancy and 30% to live birth

31
Tubal factor Severe male factor infertility Diminished ovarian reserve (time to conception is critical and success with other therapies is low) after failing treatment with less invasive therapies Ovarian failure (with donor eggs)
 after failing treatment with less invasive therapies Ovarian failure (with donor eggs)")
32
Infants born from multiple gestation pregnancies (30% of pregnancies from ART) may experience health complications as a result of pre term birth and low birth weight There is an associations between ART and septal heart defects, cleft lip, and certain GI malformations, predominantly in the singleton births
 may experience health complications as a result of pre term birth and low birth weight There is an associations between ART and septal heart defects, cleft lip, and certain GI malformations, predominantly in the singleton births")
33
ZIFT & GIFT are associated with slightly lower live birth rates than lVF (21% and 18% vs. 34%) IVF has a risk of transferring certain chromosomal abnormalities (Beckwith- Wiedemann syndrome, Angelman syndrome) in <1% of births
 IVF has a risk of transferring certain chromosomal abnormalities (Beckwith- Wiedemann syndrome, Angelman syndrome) in <1% of births.")
34
COSretrievalfertilizationembryo culturetransferprogesterone

35
OCP: to control the timing of the onset of the next menses in order to plan for initiating the COS regimen, particularly in women who have irregular or long menstrual cycles GnRH analogs: to limit the influence of any endogenous hormone levels as the cycle progresses and endogenous surge of LH

36
Agonists (Buserelin, triptorelin) initially increases gonadotropin release (flare)→daily administration → receptor down regulation → reduced pituitary secretion of LH and FSH Antagonist (Cetorelix) → immediate suppression of gonadotropin secretion 16% lower per-cycle pregnancy rates with antagonists Antagonists: shorter duration of administration and improved convenience
 initially increases gonadotropin release (flare)→daily administration → receptor down regulation → reduced pituitary secretion of LH and FSH Antagonist (Cetorelix) → immediate suppression of gonadotropin secretion 16% lower per-cycle pregnancy rates with antagonists Antagonists: shorter duration of administration and improved convenience")
38
Cetrorelix: daily SC injection of 0.25 mg or a single 3-mg dose Protocols that avoid OCP pretreatment appear to require a shorter duration and lower dose of gonadotropins

39
Administration of FSH ± LH is intended to mimic the natural process of follicular recruitment and maturation A relative increase in live birth rate of ≈ 20% with the urinary hMG (Vs. recombinant) A common starting dose is 150-225 IU/d, with dose adjustments based on the status of the developing follicles for 7-12 d
 A common starting dose is IU/d, with dose adjustments based on the status of the developing follicles for 7-12 d.")
40
To copy the effect of the physiologic LH surge on final oocyte maturation The oocyte retrieval must coincide with the completion of the oocyte maturation process, just prior to ovulation Single IM injection of 5,000-10,000 IU Doses of 5,000 IU may be administered in those who are high risk for OHSS

42
The number of embryos placed during this process must balance the risks of a multiple gestation Multiple gestation pregnancies → increased maternal and neonatal morbidity Mother complications: premature labor, pregnancy- induced HTN, and GDM Neonates complications: growth restriction and require ICU for pulmonary, GI, and neurologic complications Financial and psychosocial implications

43
Supplemental progesterone (immediately after retrieval) →prepares the endometrium for implantation of the fertilized ovum IM progesterone in oil 50 mg/d: effective but frequent reports of rash and discomfort at the injection site 17-α-hydroxyprogesterone caproate: less frequent administration (q3d), fewer injection site reactions Vaginal progesterone: ease of administration, no injection
 →prepares the endometrium for implantation of the fertilized ovum IM progesterone in oil 50 mg/d: effective but frequent reports of rash and discomfort at the injection site 17-α-hydroxyprogesterone caproate: less frequent administration (q3d), fewer injection site reactions Vaginal progesterone: ease of administration, no injection")
44
Progesterone is administered daily until a pregnancy test is performed and continued until at least 7-9 weeks gestation No significant risks to the mother or fetus from supplemental progesterone

45
45

48
A rare complication associated with COS Increased systemic vascular permeability due to high levels of vascular endothelial growth factor Risk factors: development of multiple follicles, younger age, low body weight, Hx of PCOS Monitoring: TVS and serum estradiol q1-3 d during COS If estradiol >3,500 pg/mL and/or >20 follicles at least 16mm→ cancellation or coasting (discontinuation of gonadotropins)
")
49
Typically within 1-2 weeks after oocyte retrieval Severity: mild, moderate, or severe Time: early (within 9 days after retrieval) or late (after 10 days) GI symptoms (abdominal pain, nausea, diarrhea, bloating) or weight gain, ovarian rupture, VTE, ARF, ARDS
 or late (after 10 days) GI symptoms (abdominal pain, nausea, diarrhea, bloating) or weight gain, ovarian rupture, VTE, ARF, ARDS")
Similar presentations










>")






 is a process by which egg cells are manually fertilized by sperm outside of the womb. IVF is a major treatment.>")







