Download presentation
Presentation is loading. Please wait.

1
Monday, July 25 th, 2011

2
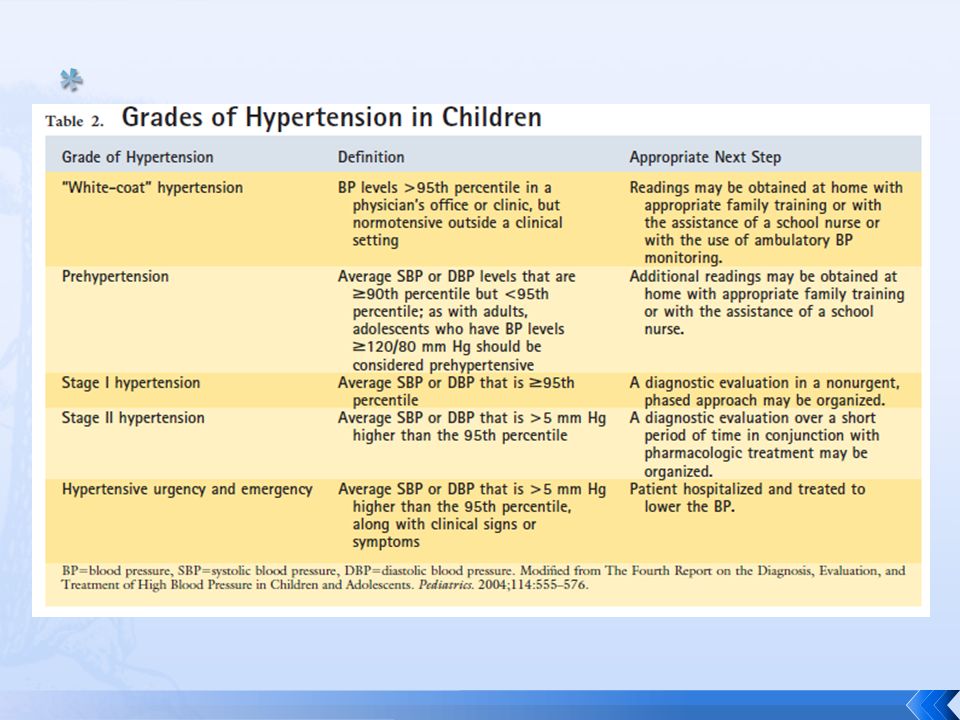
Diagnostic Evaluation COST Confirm the diagnosis Organize a diagnostic approach Determine the Severity of the HTN Treat the HTN effectively

3
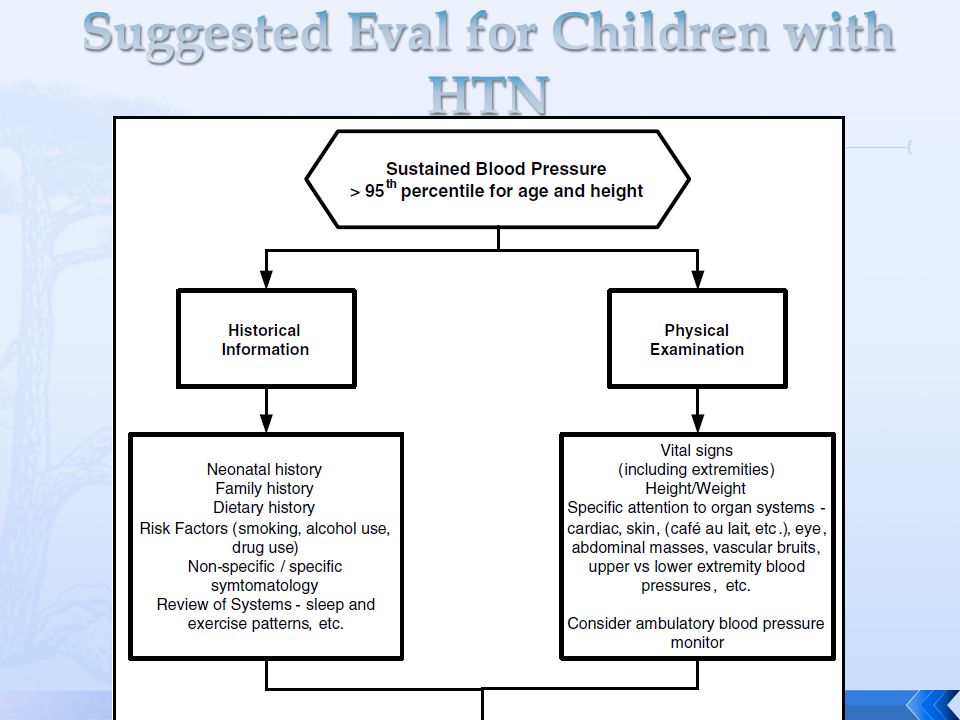
Suspect when the BP reading is high for the height, age, and sex of the child Confirmed when a high reading is obtained at three or more separate office visits about 1 week apart

4
Ensure proper BP cuff size Bladder should encircle the arm by at least 80%

6
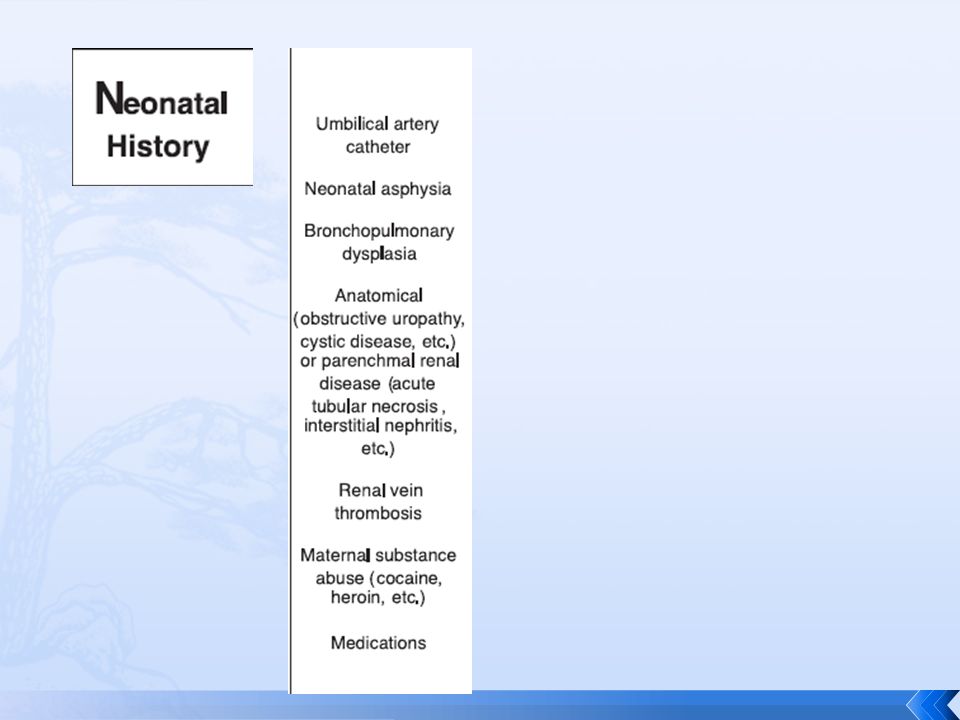
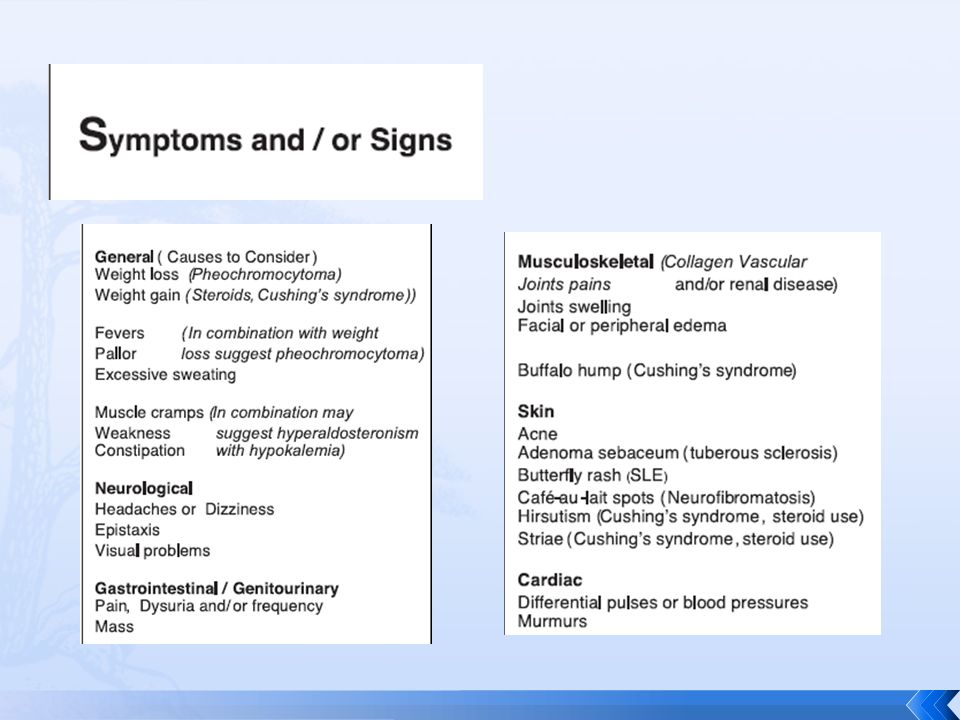
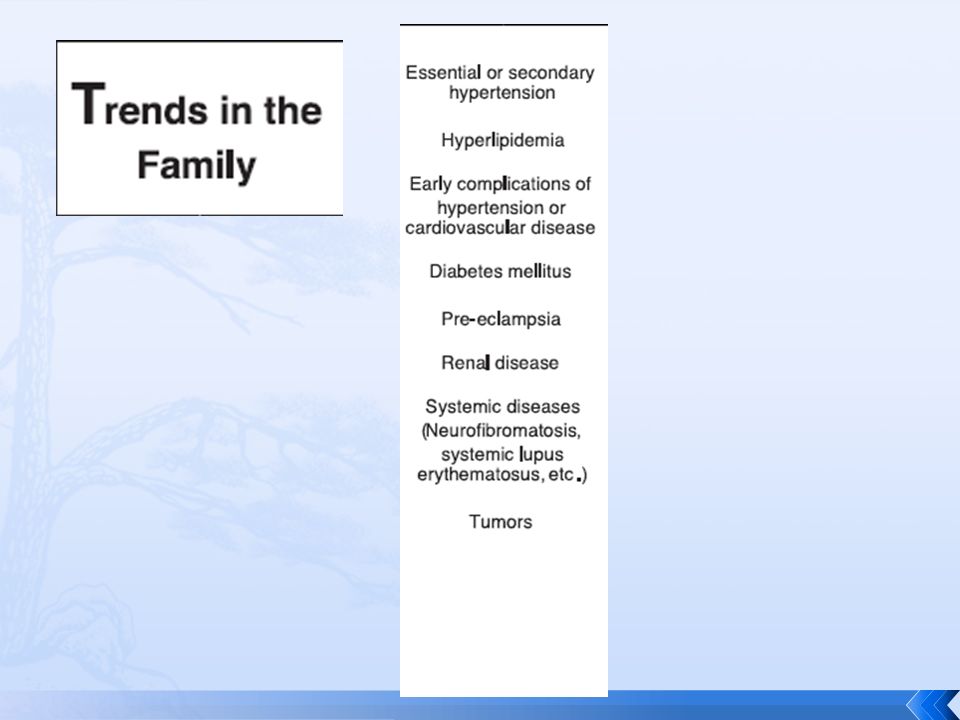
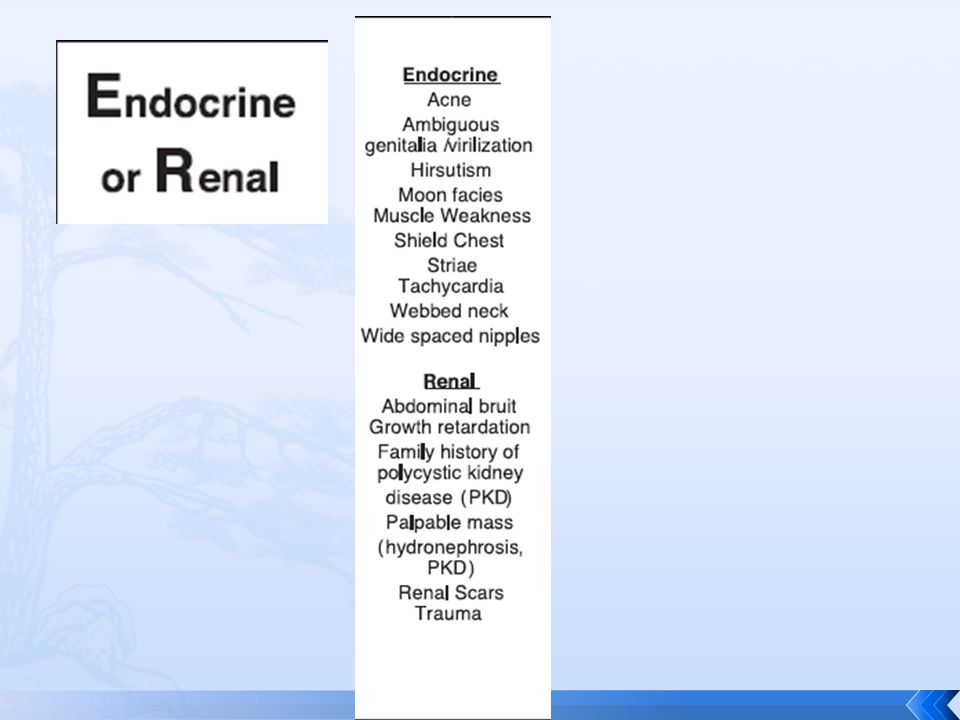
MONSTER Medications Obesity Neonatal history Symptoms or signs Trends in the family Endocrine or renal

7
**Remember, amphetamines, corticosteroids, contraceptives, cyclosporine, OTC allergy and cold medicine and licorice can cause HTN

8
BMI > 95% 3 to 5 times more likely to have hypertension Can have obstructive sleep apnea syndrome (OSAS) Causes significantly higher diastolic BPs
 Causes significantly higher diastolic BPs")
13
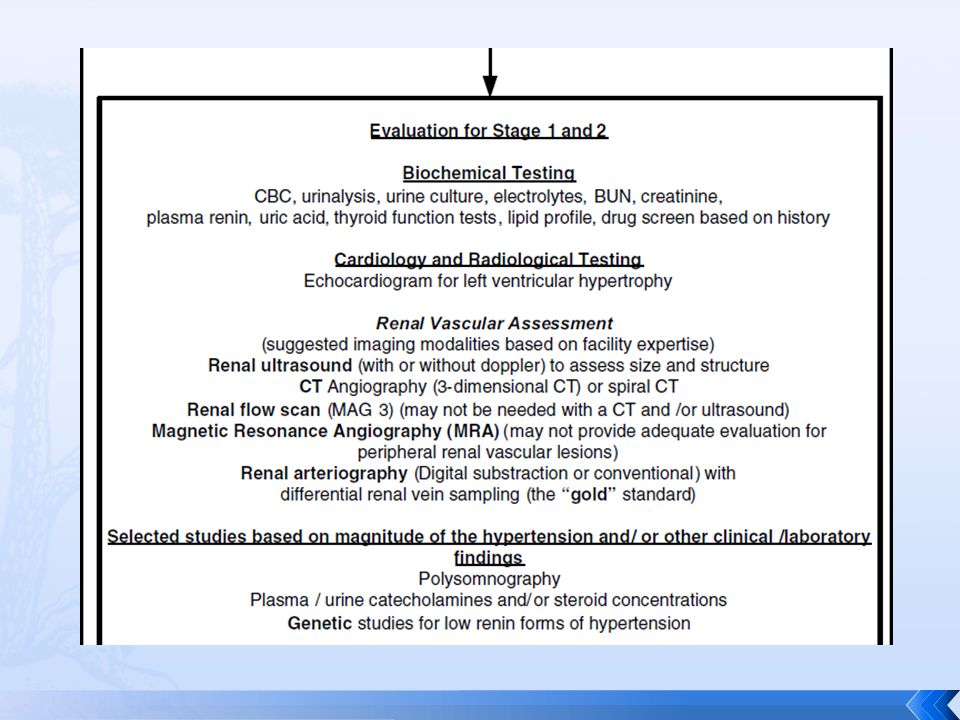
Evaluation is guided by history and physical Biochemical and imaging studies are used to address three primary organ systems: endocrine, renal, and cardiovascular

16
High uric acid is associated with high BP readings in childhood that may persist into adulthood (Bogalusa Heart Study) Strong relationship between uric acid and essential HTN (found in 89%, but only 30% with secondary HTN, none with white-coat HTN)
 Strong relationship between uric acid and essential HTN (found in 89%, but only 30% with secondary HTN, none with white-coat HTN)")
17
Combo of magnitude of BP elevation and presence of LVH on echo are proof of sustained HTN Cardiac hypertrophy is major indication for therapy Finding of LVH suggests risk for future CV disease

18
Nonpharmacologic treatment Lifestyle modifications or environmental changes must be implemented or at least attempted! Reducing sodium intake Physical activity If significant essential or severe HTN, avoid weight lifting, body building, and strength training Restriction based on the possibility of catastrophic event

19
Goal is normalization or near-normalization of BP based on age, sex, and height using a drug regimen that causes minimal adverse effects Consider starting with one drug and maximizing dose before adding a second agent

20
First-line ACE inhibitors (ex: Captopril, Enalpril) SE = renal impairment, hyperkalemia, neutropenia, anemia, dry cough, angioedema Angiotensin receptor blockers SE = renal impairment, hyperkalemia, neutropenia, anemia Calcium channel blockers (ex: Nifedipine, Isradipine) SE = peripheral edema, dizziness, nausea, headache, flushing, weakness
 SE = renal impairment, hyperkalemia, neutropenia, anemia, dry cough, angioedema Angiotensin receptor blockers SE = renal impairment, hyperkalemia, neutropenia, anemia Calcium channel blockers (ex: Nifedipine, Isradipine) SE = peripheral edema, dizziness, nausea, headache, flushing, weakness")
21
Second-line therapy Beta-blockers Central alpha agonists (Clonidine) Vasodilators (Hydralazine, Minoxidil) Diuretics
 Vasodilators (Hydralazine, Minoxidil) Diuretics")
22
1. E. Schedule 2 subsequent visits to measure BP 2. A. Echocardiography 3. B. Hyperkalemia 4. D. Perform renal ultrasonography

23
Noon conference is Inpatient ID with Dr. Begue

Similar presentations






 Drug Therapy (Antihypertensives) ACEi B.B CCB D iuretics. Centrally acting agents: alphametyldopa, HTN + pregnancy.>")

 Prevention and Control SASH – September 25, 2012 Suzanne Lapointe, RN, BA, CNN Fletcher Allen Health Care, Nephrology.>")










