Download presentation
Presentation is loading. Please wait.

1
Osteoporosis Dr Janet Horner Leeds Teaching Hospitals NHS Trust

2
Overview What is osteoporosis? Fracture risk? Who should we target for DXA? –Secondary prevention –Primary prevention What treatments are available and who do we treat?

3
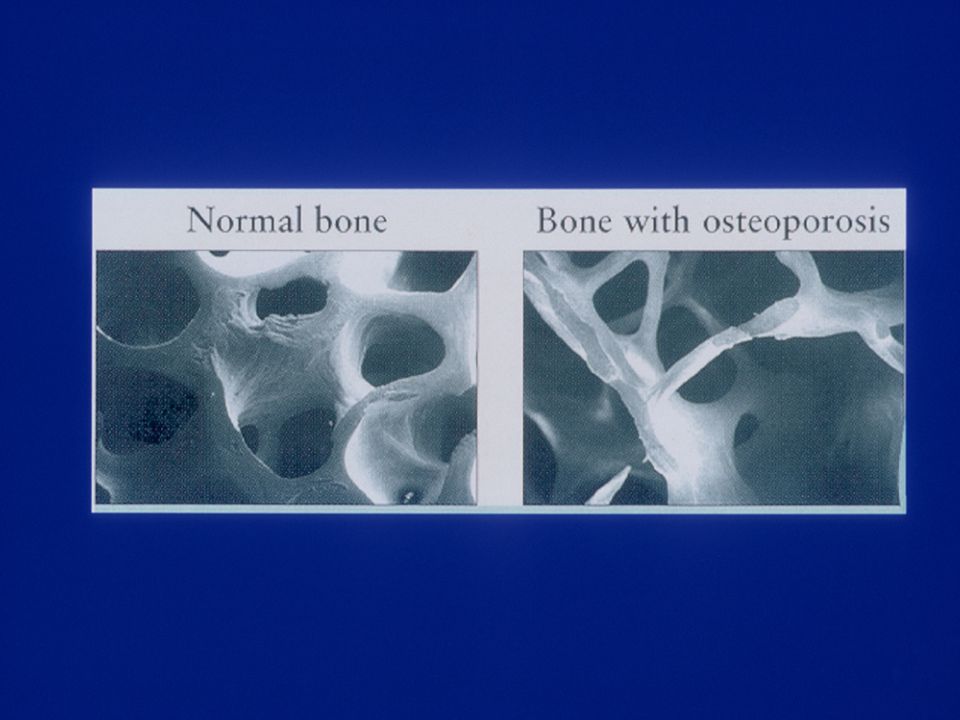
WHAT IS OSTEOPOROSIS?

4
Healthy vertebrae Osteoporotic vertebrae Rizzoli R, ed. In: Atlas of Postmenopausal Osteoporosis (First Edition). Science Press, 2004.
. Science Press,")
6
Osteoporosis ‘…a systemic skeletal disease characterised by low bone mass and microarchitectural deterioration of bone tissue, with consequent increase in bone fragility and susceptibility to fracture’ Common sites of fracture Spine Neck of femur Wrist Qualitative Definition

7
WHO definition of osteoporosis Based on the measurement of BMD The number of SDs from the average BMD in a group of 25-year-old women (T-score) Normal: T-score of -1 SD or more Osteopenia: T-score between -1 and -2.5 SD Osteoporosis: T-score below -2.5 SD Established osteoporosis: T-score below -2.5 SD, with one or more associated fragility fractures.
 Normal: T-score of -1 SD or more Osteopenia: T-score between -1 and -2.5 SD Osteoporosis: T-score below -2.5 SD Established osteoporosis: T-score below -2.5 SD, with one or more associated fragility fractures.")
8
Z scores The number of SDs from the average BMD in an group of age-matched women Gives indication of severity – ie much worse than would be expected from age related bone loss Z score < -2.0, consider secondary causes

9
0 10 20 30 40 50 60 Bone mass Age (years) Attainment of peak bone massConsolidation Age-related bone loss Men Women Menopause Age-related changes in BMD Compston JE. Clin Endocrinol 1990; 33 : 653– 682.

10
Consequences of osteoporosis Asymptomatic in absence of # Substantial pain, disability and reduced quality of life. Women >50y –1 in 3 risk of vertebral # –1 in 6 risk of hip #. After a hip fracture - some patients die within a year; 50% of survivors are incapacitated and 20% require long-term residential care Lifetime risk for woman of dying from hip # same as risk of dying from breast cancer

11
Scale of the problem Prevalence –~1.2M women in England and Wales Osteoporosis causes over 180,000 fractures per year in men and women in the UK. Cost £1.8B/y in UK. Total number of fractures is increasing 10-20% of women with osteoporosis receive Rx

12
FRACTURE RISK? Age and BMD are key risk factors and currently the only quantifiable risk factors for fragility fracture

13
BMD – estimating # risk

14
Age - estimating # risk Hip Vertebrae Wrist Adapted from Rosen at al JBMR 2004

15
# risk and BMD and age 80 70 60 50 Age, yrs Kanis, Osteoporosis International 2001

16
Fracture History Women with vertebral # have –3-5 times greater risk of further # in next 12 months –increased risk of hip # Women with wrist # >45y after fall from standing ht or less associated with doubling of risk of further osteoporotic fracture 30% of women >50y with wrist # have osteoporosis

17
% absolute annual risk of osteoporotic fracture Age T-score Fragility # >50y Number of additional risk factors FH hip # Current smoker Steroid use ever Alcohol >2u/day RA

18
WHO SHOULD WE TARGET FOR DXA?

19
NICE Technology Appraisal TA087 Osteoporosis Jan 2005 Secondary prevention of osteoporotic fragility fracture (# after fall from standing height) Postmenopausal women –not men, not CSO Recommendations based on cost and clinical effectiveness
 Postmenopausal women –not men, not CSO Recommendations based on cost and clinical effectiveness")
20
WHO SHOULD WE TARGET FOR DXA? Postmenopausal women who sustain a fragility fracture and who are < 75years

21
WHO SHOULD WE TARGET FOR DXA?– primary prevention Currently RCP case finding strategy Untreated hypogonadism (ie HRT refused or inappropriate) perimenopausal with other risk factors premature natural/surgical menopause (<45y) 2 y amenorrhoea >6m and not pregnancy related Glucocorticoid use : >3months, patient <65y (M or F) Risk of secondary osteoporosis (M or F) Malabsorption, Inflammatory bowel disease, Chronic liver disease, Hyperparathyroidism, Thyrotoxicosis
 perimenopausal with other risk factors premature natural/surgical menopause (<45y) 2 y amenorrhoea >6m and not pregnancy related Glucocorticoid use : >3months, patient <65y (M or F) Risk of secondary osteoporosis (M or F) Malabsorption, Inflammatory bowel disease, Chronic liver disease, Hyperparathyroidism, Thyrotoxicosis")
22
WHO SHOULD WE TARGET FOR DXA?– primary prevention Radiological osteopenia or vertebral deformity (M or F) Other risk factors Family history of osteoporosis / maternal hip fracture<80y Smoker Alcohol intake >35u/w (F), >50u/w (M) Low BMI <19 Height loss >2cm in 1 y
 Other risk factors Family history of osteoporosis / maternal hip fracture<80y Smoker Alcohol intake >35u/w (F), >50u/w (M) Low BMI <19 Height loss >2cm in 1 y")
23
NICE: Osteoporosis - primary prevention Cost effectiveness No opportunistic screening <70y

24
WHAT TREATMENTS ARE AVAILABLE AND WHO DO WE TREAT?

25
NICE guidelines – secondary prevention Selection of patients for Rx based on –inter-related factors, age and BMD –other age-independent risk factors Adequate calcium and vitamin D provided

26
NICE guidelines – secondary prevention: Bisphosphonate >75years, without need for DEXA scanning 65-75years, if osteoporosis confirmed by DEXA (T score < -2.5) <65years –T score - 3.0 –T score -2.5 to -3.0 and age-independent risk factor FH hip # medical conditions associated with bone loss - IBD, RA, coeliac disease, hyperthyroidism
 <65years –T score –T score -2.5 to -3.0 and age-independent risk factor FH hip # medical conditions associated with bone loss - IBD, RA, coeliac disease, hyperthyroidism")
27
NICE guidelines – secondary prevention: Strontium ranelate Bisphosphonates contraindicated renal impairment, oesophageal stricture Unable to comply with dosing instructions for bisphosphonates Unsatisfactory response to bisphosphonates 1year of Rx and further fragility fracture or loss in BMD Intolerant of bisphosphonates

28
NICE guidelines – secondary prevention: Raloxifene Strontium ranelate contraindicated OR Unsatisfactory response to strontium ranelate OR Intolerant of strontium ranelate –Nausea and diarrhoea

29
NICE guidelines – secondary prevention: Teriparatide Women >65y –unsatisfactory response to bisphosphonates 1year of Rx and further fragility fracture or loss in BMD AND –T score -4.0 OR –T score -3.0 and >2 fractures and additional age-independent risk factor

30
NICE guidelines – secondary prevention: summary Secondary prevention of osteoporotic fractures in postmenopausal women –Bisphosphonate first line Rx –Strontium ranelate as second line Rx –Raloxifene as third line Rx –Teriparatide in very severe osteoporosis

31
NICE: Osteoporosis - primary prevention Number of additional risk factors and T- score determine Rx decisions in women >70years

32
Vertebral # Endo Rev 2002: Meta - analysis of therapies for postmenopausal osteoporosis AGENTNo of trials RR (patients) (95%CI) Vitamin D8 (1130) 0.63 (0.45, 0.88) Alendronate8 (9360) 0.52 (0.43, 0.65) Risedronate5 (2604) 0.64 (0.54, 0.77) Raloxifene1(6828) 0.60 (0.5, 0.7)
 (95%CI) Vitamin D8 (1130) 0.63 (0.45, 0.88) Alendronate8 (9360) 0.52 (0.43, 0.65) Risedronate5 (2604) 0.64 (0.54, 0.77) Raloxifene1(6828) 0.60 (0.5, 0.7)")
33
Non-vertebral # Endo Rev 2002: Meta - analysis of therapies for postmenopausal osteoporosis AGENTNo of Trials RR (95%CI) (Patients) Alendronate6 (3723) 0.51(0.38,0.69) Risedronate7 (12,958) 0.73(0.61,0.87)
 (Patients) Alendronate6 (3723) 0.51(0.38,0.69) Risedronate7 (12,958) 0.73(0.61,0.87)")
34
Teriparatide (NEJM 2001 ) n=1637 Daily injections Median Rx period 21 months Raised spinal BMD by 9 and 13% (dose dependent) Reduced new vertebral fractures by 65% Reduced non-vertebral fracture risk by 35- 40%
 n=1637 Daily injections Median Rx period 21 months Raised spinal BMD by 9 and 13% (dose dependent) Reduced new vertebral fractures by 65% Reduced non-vertebral fracture risk by %")
35
Strontium Ranelate (NEJM 2004) RCT 1649 PMF with osteoporosis and at least 1 vertebral # 2g oral strontium ranelate or placebo for 3y Reduced vertebral # by 49% at 1yr and 41% over 3y
 RCT 1649 PMF with osteoporosis and at least 1 vertebral # 2g oral strontium ranelate or placebo for 3y Reduced vertebral # by 49% at 1yr and 41% over 3y")
36
Strontium Ranelate (JCEM 2005) RCT 5091 PMF with osteoporosis >74y 2g oral strontium ranelate or placebo for 3y Reduced non-vertebral # by 16% at 3y Inadequately powered to look at hip # alone Post hoc subgroup analysis of elderly high risk group did show reduction
 RCT 5091 PMF with osteoporosis >74y 2g oral strontium ranelate or placebo for 3y Reduced non-vertebral # by 16% at 3y Inadequately powered to look at hip # alone Post hoc subgroup analysis of elderly high risk group did show reduction")
37
Ibandronate BONE study (Chesnut CH, et al. J Bone Miner Res 2004;19:1241–9) After 3 years treatment with daily ibandronate - 62% reduction in new vertebral fractures MOBILE study(Miller PD, et al. J Bone Miner Res 2005;20, 8: 1315-1322) Once-monthly oral ibandronate (150mg) is at least as effective as daily ibandronate at 1 and 2 years with comparable safety to daily ibandronate
 After 3 years treatment with daily ibandronate - 62% reduction in new vertebral fractures MOBILE study(Miller PD, et al. J Bone Miner Res 2005;20, 8: ) Once-monthly oral ibandronate (150mg) is at least as effective as daily ibandronate at 1 and 2 years with comparable safety to daily ibandronate.")
38
Ca/vitamin D No indication for using Ca and vitD ALONE for prevention of further # in previously mobile elderly Record study (Lancet 2005) 5292 people >70y (85% F) who were mobile prior to sustaining low trauma # 800iu vitD or 1000mg Ca or 800iu vitD and 1000mg Ca or placebo End point – fragility # - 13% of 5292 had new fragility # No difference in incidence between groups
 5292 people >70y (85% F) who were mobile prior to sustaining low trauma # 800iu vitD or 1000mg Ca or 800iu vitD and 1000mg Ca or placebo End point – fragility # - 13% of 5292 had new fragility # No difference in incidence between groups")
39
Other Ca/vitamin D studies BMJ 2005 –3314 PMF >70y with 1 risk factor for hip# –1000mg Ca and 800iu D3 –No effect on hip # NEJM 2006 –WHI – 36, 292 PMF 50-79y –1000mg Ca and 400iu D3 –Small significant BMD –No effect on hip #

40
Calcium and vitamin D Requirements – calcium: –Postmenopausal women 1000mg/day –Dietary or supplements Requirements – vitamin D: –Postmenopausal women 800iu or 20ug/day Vitamin D concentrations –Population reference range vs. target range

41
Conclusions Osteoporosis still unrecognised and under-treated Treatment target – fracture risk Guidance on secondary prevention available Guidance on primary prevention awaited New agents – ibandronate, strontium ranelate, teriparatide Recent trials of calcium/vitamin D – not effective Rx Risk factor algorithm - aggregating other risk factors - predict individual fragility fracture risk - awaited Optimum age to start Rx ?? Optimum duration of Rx ??

42
10year probability of fracture: age and BMD Age (yrs) T-score 502.4 3.8 5.9 9.214.1 21.3 603.2 5.18.2 13.0 20.2 30.6 704.3 7.111.5 18.3 28.4 42.3 804.6 7.712.7 20.5 31.8 46.4 Kanis et al. Osteoporosis Int 2001; 12 : 989-95. +1 0 -1 -2 -3 -4

Similar presentations




, Fellowship Diabetes/Endocrinology (AKUH), PG Dip Diab (UK) Consultant Endocrinologist.>")


>")





>")





