Download presentation
Presentation is loading. Please wait.

1
ATHEROSCLEROSIS

2
22. [Path] Pathology of atherosclerosis:
Objectives This lecture provides an understanding of atherosclerosis in terms of definition, epidemiology, risk factors, pathogenesis, and clinical significance of atherosclerosis Learning outcomes At the end of the lecture, student will be able to Explain the terms atherosclerosis, arteriosclerosis and Monckeberg medial calcific sclerosis Discuss the epidemiology, risk factors, pathogenesis, and clinical consequences of atherosclerosis Describe the gross and microscopic morphology of the atherosclerosis
![22. [Path] Pathology of atherosclerosis:](http://slideplayer.com/slide/10596017/36/images/2/22.+%5BPath%5D+Pathology+of+atherosclerosis%3A.jpg "Objectives. This lecture provides an understanding of atherosclerosis in terms of definition, epidemiology, risk factors, pathogenesis, and clinical significance of atherosclerosis Learning outcomes. At the end of the lecture, student will be able to. Explain the terms atherosclerosis, arteriosclerosis and Monckeberg medial calcific sclerosis. Discuss the epidemiology, risk factors, pathogenesis, and clinical consequences of atherosclerosis. Describe the gross and microscopic morphology of the atherosclerosis.")
3
COMPONENTS Intima, Media, Adventitia, M>A or A>M ENDOTHELIUM
INTERNAL ELASTIC LAMINA ECM: Elastin ,collagen, mucopolysaccharides Smooth Muscle Connective Tissue Fat

5
Aorta (elastic artery), artery, vein, capillary: Know all the differentiating histologic features
, artery, vein, capillary: Know all the differentiating histologic features")
6
ARTERIO-SCLEROSIS GENERIC term for ANYTHING which HARDENS arteries
Three general patterns Atherosclerosis (99%) Mönckeberg medial calcific sclerosis (1%) Arteriolosclerosis - involving small arteries and arterioles, related to hypertension and/or diabetes Atherosclerosis and arteriosclerosis are often used so interchangeably, it is hardly worth differentiating them anymore, other than to know they are different!
 Mönckeberg medial calcific sclerosis (1%) Arteriolosclerosis. - involving small arteries and arterioles, related to hypertension and/or diabetes. Atherosclerosis and arteriosclerosis are often used so interchangeably, it is hardly worth differentiating them anymore, other than to know they are different!")
7
Arteriosclerosis Arteriosclerosis literally means “hardening of the arteries” it is a generic term reflecting arterial wall thickening and loss of elasticity Atherosclerosis (Greek )words for “gruel” and “hardening,” is the most frequent and clinically important pattern
words for gruel and hardening, is the most frequent and clinically important pattern")
8
Arteriosclerosis Mönckeberg medial sclerosis is characterized by
calcific deposits in muscular arteries in persons typically older than age 50 deposits may undergo metaplastic change into bone lesions do not encroach on the vessel lumen and are usually not clinically significant

9
ATHEROSCLEROSIS (classical)
Etiology/Risk Factors Pathogenesis Morphology Clinical Expression

10
ATHEROSCLEROSIS *Natural History *Epidemiology *Risk Factors
*Pathogenesis *Other Factors *Effects *Prevention

11
ATHEROSCLEROSIS Atherosclerosis
is characterized by intimal lesions called atheromas that protrude into vessel lumens (Atheroma = Atheromatous plaques = Atherosclerotic plaques)
")
12
ATHEROSCLEROSIS An atheromatous plaque consists of a raised lesion with a soft, yellow, grumous core of lipid (mainly cholesterol and cholesterol esters) covered by a firm, white fibrous cap
 covered by a firm, white fibrous cap")
14
ATHEROMATOUS PLAQUE

15
Effects of ATHEROSCLEROSIS
Mechanically obstructing blood flow Rupture, leading to thrombosis Weaken the underlying media leading to aneurysm formation

17
EPIDEMIOLOGY & RISK FACTORS

18
Epidemiology most developed nations
much less prevalent in Central and South America, Africa, and Asia mortality rate for IHD in the United States is among the highest in the world

19
Epidemiology prevalence and severity of atherosclerosis and IHD among individuals and groups are related to several risk factors Major Risks factors - Non modifiable -Potentially Controllable Lesser or Nonquantitated Risks factors

20
Risk Factors for Atherosclerosis
Major Minor NON-modifiable Modifiable Increasing age Obesity Male gender Physical inactivity Family history Stress ("type A" personality) Genetic abnormalities Postmenopausal estrogen deficiency High carbohydrate intake Modifiable Hyperlipidemia Alcohol Hypertension Lipoprotein Lp(a) Cigarette smoking Hardened (trans)unsaturated fat intake Diabetes Chlamydia pneumoniae
 Genetic abnormalities. Postmenopausal estrogen deficiency. High carbohydrate intake. Modifiable. Hyperlipidemia. Alcohol. Hypertension. Lipoprotein Lp(a) Cigarette smoking. Hardened (trans)unsaturated fat intake. Diabetes. Chlamydia pneumoniae.")
21
Major Risks factors Hyperlipidemia Hypertension Cigarette Smoking
Diabetes Mellitus

22
Additional risk factors
Inflammation (C-reactive protein) Hyperhomocystinemia Metabolic syndrome Lipoprotein (a) Other factors
 Hyperhomocystinemia. Metabolic syndrome. Lipoprotein (a) Other factors.")
23
HYPERLIPIDEMIA Hypercholesterolemia-is a major risk factor for atherosclerosis even in the absence of other risk factors, hyercholesterolemia is sufficient to stimulate lesion development

24
HYPERLIPIDEMIA The major component of serum cholesterol associated with increased risk is low-density lipoprotein (LDL) cholesterol ("bad cholesterol") LDL cholesterol has an essential physiologic role delivering cholesterol to peripheral tissues
 cholesterol ( bad cholesterol ) LDL cholesterol has an essential physiologic role delivering cholesterol to peripheral tissues")
25
HYPERLIPIDEMIA high-density lipoprotein (HDL, "good cholesterol") mobilizes cholesterol from developing and existing atheromas and transports it to the liver for excretion in the bile higher levels of HDL correlate with reduced risk
 mobilizes cholesterol from developing and existing atheromas and transports it to the liver for excretion in the bile higher levels of HDL correlate with reduced risk")
26
CHOLESTEROL CLEFTS Needle shaped washed out spaces in arteries, are cholesterol clefts, and can be nothing else, and like all other fat, yellow grossly, white microscopically.

27
HYPERTENSION major risk factor for atherosclerosis both systolic and diastolic levels are important

28
HYPERTENSION HYPERTENSION causes ATHEROSCLEROSIS. Why?
ATHEROSCLEROSIS causes HYPERTENSION. Why?

29
CIGARETTES a well-established risk factor

30
DIABETES Diabetes mellitus induces hypercholesterolemia
100-fold increased risk of atherosclerosis-induced gangrene of the lower extremities

31
NON-modifiable Age is a dominant influence accumulation of atherosclerotic plaque is typically a progressive process incidence of myocardial infarction in men increases fivefold between ages 40 and 60 Death rates from IHD rise with each decade even into advanced age

32
NON-modifiable Gender premenopausal women are relatively protected against atherosclerosis After menopause incidence of atherosclerosis-related diseases increases and with greater age eventually exceeds that of men

33
NON-modifiable Genetics
familial predisposition to atherosclerosis and IHD is multifactorial well-defined genetic derangements in lipoprotein metabolism, such as familial hypercholesterolemia that result in excessively high blood lipid levels familial clustering of other risk factors, such as hypertension or diabetes

34
NON major factors Homocysteinuria/homocysteinemia, related to low B6 and folate intake Coagulation defects Lipoprotein Lp(a), independent of cholesterol. Lp(a) is an altered form of LDL Inadequate exercise, Type “A” personality, obesity (independent of diabetes) Protective effect of moderate alcohol?
, independent of cholesterol. Lp(a) is an altered form of LDL Inadequate exercise, Type A personality, obesity (independent of diabetes) Protective effect of moderate alcohol")
35
PATHOGENESIS Atherosclerosis is
a chronic inflammatory response of the arterial wall initiated by injury to the endothelium

36
PATHOGENESIS Lesion progression occurs through interactions of
modified lipoproteins monocyte-derived macrophages T lymphocytes normal cellular constituents of the arterial wall

37
PATHOGENESIS Chronic endothelial injury
Accumulation of lipoproteins in arterial WALL OXIDATION of lipoproteins Monocytes migrate endothelium Platelet adhesion and activation Migration of SMOOTH MUSCLE from media to intima to activate macrophages (foam cells) Proliferation of SMOOTH MUSCLE and ECM Accumulation of lipids in cells and ECM
 Proliferation of SMOOTH MUSCLE and ECM Accumulation of lipids in cells and ECM.")
38
PATHOGENESIS Endothelial Injury Causes hemodynamic forces, immune complex deposition, irradiation, or chemicals Early lesions begin at sites of morphologically intact endothelium

39
PATHOGENESIS Non-denuding endothelial dysfunction underlies atherosclerosis in the setting of intact but dysfunctional ECs there is increased endothelial permeability enhanced leukocyte adhesion altered gene expression

40
PATHOGENESIS Causes of endothelial dysfunction
Hemodynamic disturbances Hypercholesterolemia Toxins from cigarette smoke, Homocysteine infectious agents Inflammatory cytokines (e.g., tumor necrosis factor, TNF)
")
41
PATHOGENESIS Hypercholesterolemia can directly impair EC function by increasing local production of reactive oxygen species With chronic hyperlipidemia, lipoproteins accumulate within the intima

42
PATHOGENESIS These lipids are oxidized through the action of oxygen free radicals locally generated by macrophages or Ecs Oxidized LDL is ingested by macrophages through a scavenger receptor resulting in foam-cell formation

43
PATHOGENESIS Oxidized LDL
stimulates the release of growth factors, cytokines, and chemokines by ECs and macrophages that increase monocyte recruitment into lesions cytotoxic to ECs and SMCs and can induce EC dysfunction

44
PATHOGENESIS Causes of Dyslipoproteinemias
mutations that encode defective apoproteins alter the lipoprotein receptors on cells other underlying disorder that affects the circulating levels of lipids (e.g., nephrotic syndrome, alcoholism, hypothyroidism, or diabetes mellitus)
")
45
PATHOGENESIS Common lipoprotein abnormalities in the general population include increased LDL cholesterol levels (2) decreased HDL cholesterol levels (3) increased levels of the abnormal Lp(a) Genetic defects in lipoprotein uptake and metabolism that cause hyperlipoproteinemia are associated with accelerated atherosclerosis
 decreased HDL cholesterol levels. (3) increased levels of the abnormal Lp(a) Genetic defects in lipoprotein uptake and metabolism that cause hyperlipoproteinemia are associated with accelerated atherosclerosis.")
46
PATHOGENESIS Inflammation Inflammatory cells and mediators are involved in the initiation, progression, and the complications of atherosclerotic lesions

47
PATHOGENESIS Inflammation
Dysfunctional arterial ECs express adhesion molecules that encourage leukocyte adhesion Monocytes and T cells adhere to the endothelium, they migrate into the intima under the influence of locally produced chemokines

48
PATHOGENESIS Monocytes transform into macrophages and avidly engulf lipoproteins, including oxidized LDL progressive accumulation of oxidized LDL drives lesion progression

49
PATHOGENESIS Activated macrophages
cytokine production (e.g., TNF) that further increases leukocyte adhesion and chemokine production that in turn propel mononuclear inflammatory cell recruitment produce reactive oxygen species, aggravating LDL oxidation
 that further increases leukocyte adhesion and chemokine production that in turn propel mononuclear inflammatory cell recruitment. produce reactive oxygen species, aggravating LDL oxidation.")
50
PATHOGENESIS T lymphocytes recruited to the intima interact with macrophages and can generate a chronic immune inflammatory state Activated T cells in the growing intimal lesions elaborate inflammatory cytokines, (e.g., interferon-γ), which in turn can stimulate macrophages as well as ECs and SMCsAs
, which in turn can stimulate macrophages as well as ECs and SMCsAs")
51
PATHOGENESIS A consequence of the chronic inflammatory state activated leukocytes and vascular wall cells release growth factors that promote SMC proliferation and ECM synthesis

52
PATHOGENESIS Infection
may drive the local inflammatory process that underlies atherosclerosis (hypothesis has yet to be conclusively proven) Herpesvirus, cytomegalovirus, and Chlamydia pneumoniae have all been detected in atherosclerotic plaques but not in normal arteries increased antibody titers to C. pneumoniae in patients with more severe atherosclerosis
 Herpesvirus, cytomegalovirus, and Chlamydia pneumoniae have all been detected in atherosclerotic plaques but not in normal arteries. increased antibody titers to C. pneumoniae in patients with more severe atherosclerosis.")
53
PATHOGENESIS Smooth Muscle Proliferation
Intimal smooth muscle cell proliferation and ECM deposition convert a fatty streak (the earliest lesion) into a mature atheroma contribute to the progressive growth of atherosclerotic lesions ( intimal smooth muscle cells may be recruited from circulating precursors and they have a proliferative and synthetic phenotype distinct from the underlying medial smooth muscle cells)
 into a mature atheroma. contribute to the progressive growth of atherosclerotic lesions. ( intimal smooth muscle cells may be recruited from circulating precursors and they have a proliferative and synthetic phenotype distinct from the underlying medial smooth muscle cells)")
54
PATHOGENESIS Growth factors (PDGF, FGF, TGF-α)
Smooth Muscle Proliferation & ECM synthesis Growth factors (PDGF, FGF, TGF-α) The recruited smooth muscle cells synthesize ECM (notably collagen) that stabilizes atherosclerotic plaques Activated inflammatory cells in atheromas can cause intimal smooth muscle cell apoptosis, and also increase ECM catabolism resulting in unstable plaques
 The recruited smooth muscle cells synthesize ECM (notably collagen) that stabilizes atherosclerotic plaques. Activated inflammatory cells in atheromas can cause intimal smooth muscle cell apoptosis, and also increase ECM catabolism resulting in unstable plaques.")
55
The intimal plaque may progressively
encroach on the vessel lumen compress and cause degeneration of the underlying media disruption of the fibrous cap can lead to thrombosis and acute vascular occlusion

56
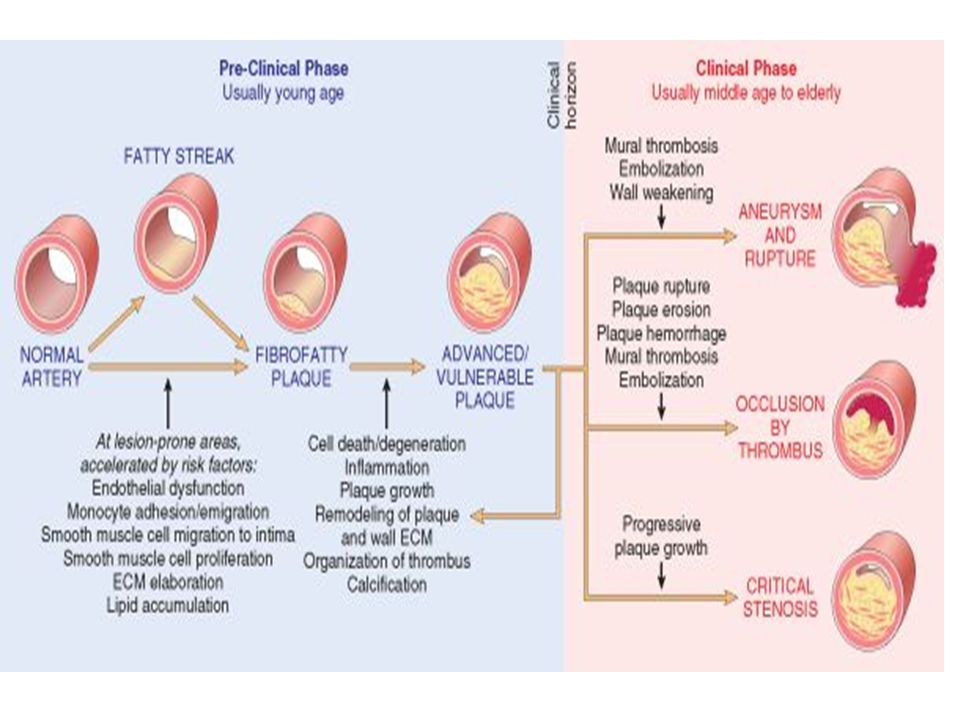
A very well constructed graphic understanding of the pathogenesis of atherosclerosis. Please be expected to not only KNOW these five items, but their correct ORDER too.

57
Main FOUR STARS of PATHOGENESIS
1) Endothelial Injury 2) Inflammation 3) Lipids 4) Smooth Muscle Cells, SMCs
 Endothelial Injury. 2) Inflammation. 3) Lipids. 4) Smooth Muscle Cells, SMCs.")
59
MORPHOLOGIC CONCEPTS Intimal Thickening Lipid Accumulation Streak
Atheroma Smooth Muscle Hyperplasia and Migration Fibrosis Calcification Aneurysm Thrombosis

60
Morphology Most extensively involved vessels are lower abdominal aorta
coronary arteries popliteal arteries internal carotid arteries vessels of the circle of Willis

61
Morphology Fatty Streaks composed of histologically
lipid-filled foam cells but are not significantly raised Gross Multiple minute yellow, flat spots that can coalesce into elongated streaks, 1 cm long or longer

63
Morphology Atherosclerotic Plaque Grossly appear white to yellow
superimposed thrombus over ulcerated plaques is red-brown Plaques vary from 0.3 to 1.5 cm in diameter but can coalesce to form larger masses patchy, usually involving only a portion of any given arterial wall

64
Morphology Atherosclerotic plaques have three principal components:
cells, including smooth muscle cells, macrophages, and T cells ECM, including collagen, elastic fibers, and proteoglycans intracellular and extracellular lipid (These components occur in varying proportions and configurations in different lesions)
")
65
Morphology A superficial fibrous cap composed of smooth muscle cells and relatively dense collagen Beneath and to the side of the cap (the “shoulder”) is a more cellular area containing macrophages, T cells, and smooth muscle cells Deep to the fibrous cap is a necrotic core, containing lipid (primarily cholesterol and cholesterol esters)
 is a more cellular area containing macrophages, T cells, and smooth muscle cells. Deep to the fibrous cap is a necrotic core, containing lipid (primarily cholesterol and cholesterol esters)")
67
clinically important changes
Rupture, ulceration, or erosion & thrombosis calcification Hemorrhage into a plaque Atheroembolism Aneurysm formation

68
MILD ADVANCED

69
fibrous cap (F) central necrotic (largely lipid) core (C) lumen (L Histologic features of atheromatous plaque in the coronary artery

70
*NATURAL HISTORY

72
1) FATTY STREAK (non-palpable)
2) ATHEROMA (plaque) (palpable) 3) THROMBUS (non-functional, symptomatic) Atherosclerosis is a LIFELONG, even childhood, process. This chart is worth knowing.
 ATHEROMA. (plaque) (palpable) 3) THROMBUS (non-functional, symptomatic) Atherosclerosis is a LIFELONG, even childhood, process. This chart is worth knowing.")
73
Commonly affecting sites

74
CONSEQUENCES OF ATHEROSCLEROTIC DISEASE
Myocardial infarction (heart attack) cerebral infarction (stroke) aortic aneurysms peripheral vascular disease (gangrene of the legs)
 cerebral infarction (stroke) aortic aneurysms. peripheral vascular disease (gangrene of the legs)")
75
Atherosclerosis affecting coronary artery

76
Atherosclerosis affecting cerebral artery

77
Myocardial infarction

78
Stroke 4/28/2017 7:35 AM

79
Aneurysm

80
CONSEQUENCES OF ATHEROSCLEROTIC DISEASE
Atherosclerotic Stenosis chronic occlusion - significantly limits flow [mesenteric occlusion and bowel ischemia, chronic IHD, ischemic encephalopathy, and intermittent claudication (diminished extremity perfusion)] acute plaque rupture -dangerous complication
] acute plaque rupture -dangerous complication.")
81
CONSEQUENCES OF ATHEROSCLEROTIC DISEASE
Acute Plaque Change Rupture/fissuring, exposing highly thrombogenic plaque constituents Erosion/ulceration, exposing the thrombogenic subendothelial basement membrane to blood Hemorrhage into the atheroma expanding its volume Plaque erosion or rupture is typically promptly followed by partial or complete vascular thrombosis

Similar presentations


















>")






