Download presentation
Presentation is loading. Please wait.

1
Bone forming drug Pol.Maj.Dr. Tanawat amphansap
MD,FRCOST (Trauma), FDVSE Police General Hospital
, FDVSE. Police General Hospital.")
2
Mechanism of Action of Available Osteoporosis Therapies
Osteoclast Precursors RANKL RANK Wnt (anabolic pathway) Estrogen therapy SERM, Hormones Bisphosphonates Binds to bone; inhibits osteoclasts Teriparatide, PTH analog Slide has animation , only click once at beginning of slide. Key Points: All therapeutic options work differently: PTH: appears to have direct actions on osteoblast activity, with biochemical and histomorphometric evidence. PTH activates bone remodeling but still appears to favour bone formation over bone resorption. PTH stimulates insulin-like growth factor-1 (IGF-1) and collagen production and appears to increase osteoblast number by stimulation replication, enhancing osteoblast recruitment and inhibiting apoptosis. SERMs: are estrogen receptor ligands that act like estrogens in some tissues, but block estrogen in others. Thus, SERMs may exhibit an agonistic or antagonistic biocharacter, depending on the context in which their activity is examined. The majority of estrogen effects on bone resorption are mediated through paracrine factors produced by osteopblasts. These actions include 1) increasing IGF-1 and transforming growth factor and 2) suppressing interleukin, tumour necrosis factor and osteocalcin synthesis. The indirect estrogen actions primarily decrease bone resorption. BPs: Pharmacologic agents that control osteoclasts either act directly on the osteoclast or on the bone itself and then are taken up into osteoclasts. When osteoclasts begin to resorb bone that is impregnated with BP, the BP released during resorption impairs the ability of the osteoclasts to form the ruffled border. Denosumab: is a fully human monoclonal antibody with high affinity and specificity for RANKL. When denosumab inhibits the action of RANKL, it reduces the differentiation, activation, and survival of osteoclasts, thereby slowing bone resorption. Note: Concern that arrow from various osteoporotic treatments only points to osteoblasts may be misleading, and although the mechanism is complex, these compounds ultimately supress bone resorption. Should there be an arrow from treatments to osteoclasts? References: Lindsay R, Cosman F. Osteoporosis. In: Braunwald E, Fauci A, Kasper D, et al., eds. Harrison’s Principles of Internal Medicine. 16th edition. New York: McGraw-Hill; 2005: Boyle WJ, Simonet WS, Lacey DL. Osteoclast differentiation and activation. Nature. 2003;423: Lewiecki EM. RANK ligand inhibition with denosumab for the management of osteoporosis. Expert Opin Biol Ther. 2006;6: EVISTA Product Monograph, Eli Lilly, 2008. Denosumab RANK Ligand inhibitor Osteoblast Osteoclast Adapted from: Boyle WJ et al. Nature 2003; 423:
 Estrogen therapy. SERM, Hormones. Bisphosphonates Binds to bone; inhibits osteoclasts. Teriparatide, PTH analog. Slide has animation , only click once at beginning of slide. Key Points: All therapeutic options work differently: PTH: appears to have direct actions on osteoblast activity, with biochemical and histomorphometric evidence. PTH activates bone remodeling but still appears to favour bone formation over bone resorption. PTH stimulates insulin-like growth factor-1 (IGF-1) and collagen production and appears to increase osteoblast number by stimulation replication, enhancing osteoblast recruitment and inhibiting apoptosis. SERMs: are estrogen receptor ligands that act like estrogens in some tissues, but block estrogen in others. Thus, SERMs may exhibit an agonistic or antagonistic biocharacter, depending on the context in which their activity is examined. The majority of estrogen effects on bone resorption are mediated through paracrine factors produced by osteopblasts. These actions include 1) increasing IGF-1 and transforming growth factor and 2) suppressing interleukin, tumour necrosis factor and osteocalcin synthesis. The indirect estrogen actions primarily decrease bone resorption. BPs: Pharmacologic agents that control osteoclasts either act directly on the osteoclast or on the bone itself and then are taken up into osteoclasts. When osteoclasts begin to resorb bone that is impregnated with BP, the BP released during resorption impairs the ability of the osteoclasts to form the ruffled border. Denosumab: is a fully human monoclonal antibody with high affinity and specificity for RANKL. When denosumab inhibits the action of RANKL, it reduces the differentiation, activation, and survival of osteoclasts, thereby slowing bone resorption. Note: Concern that arrow from various osteoporotic treatments only points to osteoblasts may be misleading, and although the mechanism is complex, these compounds ultimately supress bone resorption. Should there be an arrow from treatments to osteoclasts References: Lindsay R, Cosman F. Osteoporosis. In: Braunwald E, Fauci A, Kasper D, et al., eds. Harrison’s Principles of Internal Medicine. 16th edition. New York: McGraw-Hill; 2005: Boyle WJ, Simonet WS, Lacey DL. Osteoclast differentiation and activation. Nature. 2003;423: Lewiecki EM. RANK ligand inhibition with denosumab for the management of osteoporosis. Expert Opin Biol Ther. 2006;6: EVISTA Product Monograph, Eli Lilly, Denosumab. RANK Ligand inhibitor. Osteoblast. Osteoclast. Adapted from: Boyle WJ et al. Nature 2003; 423:")
3
Therapeutic options for osteoporosis
Inhibitors of bone resorption Bisphosphonates Alendronate Etidronate Risedronate Calcitonin Estrogen ± progestin Selective estrogen receptor modulators (SERMs) Raloxifene Stimulators of bone formation Parathyroid hormone Mixed mechanism of action Active Vitamin D metabolites Strontium ranelate Recommended for all women at risk for osteoporosis Calcium and vitamin D Slide 34 Speaker Notes: Over the last few years, many new therapeutic options have become available for the prevention and treatment of osteoporosis. Commonly used agents include a variety of estrogen and estrogen-plus-progestin preparations, selective estrogen receptor modulators (SERMs) (such as raloxifene), calcitonin, and bisphosphonates (such as etidronate, alendronate, and risedronate). Calcium and vitamin D are recommended for all women at risk for osteoporosis unless there are specific contraindications.
 Raloxifene. Stimulators of. bone formation. Parathyroid hormone. Mixed mechanism of action. Active Vitamin D metabolites. Strontium ranelate. Recommended for all women at risk for osteoporosis. Calcium and vitamin D. Slide 34. Speaker Notes: Over the last few years, many new therapeutic options have become available for the prevention and treatment of osteoporosis. Commonly used agents include a variety of estrogen and estrogen-plus-progestin preparations, selective estrogen receptor modulators (SERMs) (such as raloxifene), calcitonin, and bisphosphonates (such as etidronate, alendronate, and risedronate). Calcium and vitamin D are recommended for all women at risk for osteoporosis unless there are specific contraindications.")
4
Human Parathyroid Hormone 1-34 (teriparatide) and 1-84
10 20 30 Ser Val Glu Ile Gln Leu Met His Asn Gly Lys Arg Trp Asp Phe 50 40 60 70 80 - COOH H 2 N hPTH/PTHrP Receptor hPTH (1-34) hPTH 1 - 34 (crystal structure) Adapted from Proc Natl Acad Sci USA (1974);71:384 Adapted from Jin et al. J Biol Chem (2000);35:27238
 hPTH (crystal structure) Adapted from Proc Natl Acad Sci USA (1974);71:384. Adapted from Jin et al. J Biol Chem (2000);35:")
5
Classical Actions of PTH
Source: see notes reference; originally created by Joanne Lorraine Classical Actions of PTH Review: WPDF global kit #LX200308c (Li Xie ) 2004 update: J. Alam WPDF#ja200411a PTH Absorb Ca++ and PO4-- In Small Intestine PTH Reviewer Memo: Release Ca++ from bone Reabsorb Ca++ in kidneys Synthesis of 1,25 (0H)2 D3 Naturally occurring parathyroid hormone primarily maintains serum calcium levels within a very tight range. A balance in serum calcium levels is achieved by PTH acting on: Bone: calcium resorption from bone Vitamin D: hydroxylation of vitamin D; the 1,25 dihydroxy active version of vitamin D assists in the resorption of both calcium and phosphorus from the intestine; Kidney: PTH acts on the renal tubules to reabsorb filtered calcium, to inhibit the re-absorption of phosphate, and to enhance the synthesis of 1,25 di-hydroxy vitamin D. Calcium receptors recognize extracellular calcium ions as their principal ligand. The calcium receptor is found on the surface of parathyroid cells, as well as on the calcitonin-secreting C cells of the thyroid, renal tubular cells, bone cells, and some intestinal epithelial cells that are involved in calcium absorption. When serum levels of ionized calcium drop, the calcium receptor (which is coupled to different G proteins) activates or inhibits various intracellular enzymes, with the end result of PTH secretion. High levels of ionized serum calcium suppress PTH secretion. __________________ Data adapted from Juppner H, Brown EM, Kronenber HM. Parathyroid hormone. Ch 13 in Primer on the Metabolic Bone Diseases and Disorders of Bone Mineral Metabolism. Ed Murray J Favus. Lippincott, Williams and Wilkins, Philadelphia, pp Maintain Serum Calcium Levels Sourced from Juppner H, Brown EM, Kronenber HM. 1999 Slide Modified: on: 9/4/2003 8:12:23 AM SL3 Rev: 45 on: 9/25/2003 6:38:58 PM SL1 Rev: 128 Memo: added reference from Joanne Lorraine to notes 06Aug03 - MR minor edits to notes 18Aug03 - MR
 2004 update: J. Alam WPDF#ja200411a. PTH. Absorb Ca++ and PO4-- In Small Intestine. PTH. Reviewer Memo: Release Ca++ from bone. Reabsorb Ca++ in kidneys. Synthesis of 1,25 (0H)2 D3. Naturally occurring parathyroid hormone primarily maintains serum calcium levels within a very tight range. A balance in serum calcium levels is achieved by PTH acting on: Bone: calcium resorption from bone. Vitamin D: hydroxylation of vitamin D; the 1,25 dihydroxy active version of vitamin D assists in the resorption of both calcium and phosphorus from the intestine; Kidney: PTH acts on the renal tubules to reabsorb filtered calcium, to inhibit the re-absorption of phosphate, and to enhance the synthesis of 1,25 di-hydroxy vitamin D. Calcium receptors recognize extracellular calcium ions as their principal ligand. The calcium receptor is found on the surface of parathyroid cells, as well as on the calcitonin-secreting C cells of the thyroid, renal tubular cells, bone cells, and some intestinal epithelial cells that are involved in calcium absorption. When serum levels of ionized calcium drop, the calcium receptor (which is coupled to different G proteins) activates or inhibits various intracellular enzymes, with the end result of PTH secretion. High levels of ionized serum calcium suppress PTH secretion. __________________. Data adapted from Juppner H, Brown EM, Kronenber HM. Parathyroid hormone. Ch 13 in Primer on the Metabolic Bone Diseases and Disorders of Bone Mineral Metabolism. Ed Murray J Favus. Lippincott, Williams and Wilkins, Philadelphia, pp Maintain Serum Calcium Levels. Sourced from Juppner H, Brown EM, Kronenber HM Slide Modified: on: 9/4/2003 8:12:23 AM SL3 Rev: 45. on: 9/25/2003 6:38:58 PM SL1 Rev: 128. Memo: added reference from Joanne Lorraine to notes 06Aug03 - MR minor edits to notes 18Aug03 - MR.")
6
PTH once-daily continuous osteoclast osteoblast number/function
Source: once-daily continuous osteoblast apoptosis bone lining cells cbfa1 BMP PPAR Wnt IGF 1,2 amphiregulin RANKL OPG RANKL OPG Review: 2004 update: J. Alam WPDF#ja200411a osteoclast Reviewer Memo: The skeletal effects of PTH depend upon the pattern of systemic exposure. Once-daily administration of PTH stimulates new bone formation on trabecular and cortical bone surfaces by preferential stimulation of osteoblastic activity over osteoclastic activity. This effect of PTH leads to a rapid increase in skeletal mass and an increase in bone turnover markers. By increasing new bone formation, PTH improves skeletal microarchitecture, bone mass and bone strength, and thereby reduces the risk of fracture. Numerous factors have been implicated in the bone forming response, but selective down regulation of osteoclast differentiation factor or RANKL and stimulation of osteoprotegerin (OPG) secretion by osteoblasts seems to play a key role. By contrast, continuous excess of endogenous PTH, as occurs in severe hyperparathyroidism, may be detrimental to the skeleton because bone resorption is stimulated more than bone formation (Hock JM 2001). The continuous infusion of PTH(1-38) in rats resulted in the increased expression of RANKL and decreased expression of both OPG and bone-formation-associated genes such as osteoblast specific transcription factor, osteocalcin, bone sialoprotein, and type I collagen. __________________ Dobnig H, Turner RT. Evidence that intermittent treatment with parathyroid hormone increases bone formation in adult rats by activation of bone lining cells. Endocrinology 1995; 136(8): Dobnig H, and Turner RT. Evidence that intermittent treatment with parathyroid hormone increases bone formation in adult rats by activation of bone lining cells. Endocrinology 1995;136: Hock, JM. Anabolic Actions of PTH in the skeletons of animals. J Musculoskel Neuron Interact 2001; 2:33-47. Jilka RL, Weinstein RS, Bellido T, et al. Increased bone formation by prevention of osteoblast apoptosis with parathyroid hormone. J Clin Invest 1999;104: Kalu DN, Pennock J, Doyle FH, et al. Parathyroid hormone and experimental osteosclerosis. Lancet 1970;1: Ma YL, Cain RL, Halladay DL, et al. Catabolic Effects of continuous human PTH (1-38) in vivo is associated with sustained stimulation of RANKL and inhibition of osteoprotegerin and gene-associated bone formation. Endocrinology 2001; 142: Neer RM, Arnaud CD, Zanchetta JR, et al. Effect of parathyroid hormone (1-34) on fractures and bone mineral density in postmenopausal women with osteoporosis. N Engl J Med 2001;344: Podbesek R, Edouard C, Meunier PJ, et al. Effects of two treatment regimes with synthetic human parathyroid hormone fragment on bone formation and the tissue balance of trabecular bone in greyhounds. Endocrinology 1983; 112: Tam CS, Heersche JNM, Murray TM et al. Parathyroid hormone stimulates the bone apposition rate independently of its resorptive action: Differential effects of intermittent and continuous administration. Endocrinology 1982;110: osteoblast number/function bone resorption bone formation serum Ca++ bone mass/strength Slide Modified: Memo:
 secretion by osteoblasts seems to play a key role. By contrast, continuous excess of endogenous PTH, as occurs in severe hyperparathyroidism, may be detrimental to the skeleton because bone resorption is stimulated more than bone formation (Hock JM 2001). The continuous infusion of PTH(1-38) in rats resulted in the increased expression of RANKL and decreased expression of both OPG and bone-formation-associated genes such as osteoblast specific transcription factor, osteocalcin, bone sialoprotein, and type I collagen. __________________. Dobnig H, Turner RT. Evidence that intermittent treatment with parathyroid hormone increases bone formation in adult rats by activation of bone lining cells. Endocrinology 1995; 136(8): Dobnig H, and Turner RT. Evidence that intermittent treatment with parathyroid hormone increases bone formation in adult rats by activation of bone lining cells. Endocrinology 1995;136: Hock, JM. Anabolic Actions of PTH in the skeletons of animals. J Musculoskel Neuron Interact 2001; 2: Jilka RL, Weinstein RS, Bellido T, et al. Increased bone formation by prevention of osteoblast apoptosis with parathyroid hormone. J Clin Invest 1999;104: Kalu DN, Pennock J, Doyle FH, et al. Parathyroid hormone and experimental osteosclerosis. Lancet 1970;1: Ma YL, Cain RL, Halladay DL, et al. Catabolic Effects of continuous human PTH (1-38) in vivo is associated with sustained stimulation of RANKL and inhibition of osteoprotegerin and gene-associated bone formation. Endocrinology 2001; 142: Neer RM, Arnaud CD, Zanchetta JR, et al. Effect of parathyroid hormone (1-34) on fractures and bone mineral density in postmenopausal women with osteoporosis. N Engl J Med 2001;344: Podbesek R, Edouard C, Meunier PJ, et al. Effects of two treatment regimes with synthetic human parathyroid hormone fragment on bone formation and the tissue balance of trabecular bone in greyhounds. Endocrinology 1983; 112: Tam CS, Heersche JNM, Murray TM et al. Parathyroid hormone stimulates the bone apposition rate independently of its resorptive action: Differential effects of intermittent and continuous administration. Endocrinology 1982;110: osteoblast number/function. bone resorption. bone formation. serum Ca++ bone mass/strength. Slide Modified: Memo:")
9
Antiresorptive Therapy Anabolic Therapy Targets osteoclasts1
Targets osteoblasts5 Reduces bone turnover1 Increases bone formation5,6 Reduces cortical porosity1 Increases trabecular bone volume6 Increases BMD1-3 Increases BMD5,7 Reduces fracture risk2-4 Improves cancellous microarchitecture6 Increases cortical thickness and improves cortical bone geometry6 Reduces fracture risk5,7 SPEAKER NOTES: Antiresorptive therapies and anabolic therapies, such as teriparatide, have different effects on bone. Antiresorptives maintain bone by inhibiting osteoclasts and reducing bone turnover. This leads to an increase in BMD, a reduction in bone perforations, and subsequently a reduction in fracture risk. Teriparatide is an anabolic therapy that stimulates osteoblasts to build new bone. This leads to an increase in bone volume and BMD and also improves bone microarchitecture. PRESENTATION TIPS: This is a critical differentiating factor between teriparatide and most other therapeutic choices for osteoporosis. Stress to the audience that antiresorptives maintain bone, whereas teriparatide builds new bone, and that this is an important therapeutic difference when approaching a patient who has already experienced a fragility fracture. Remind the audience of the patient case of hip fracture: in this patient who has experienced an osteoporotic fracture, these are 2 very different treatment approaches maintain current bone strength or build new bone. This concept is important to keep in mind when going through the data supporting the use of teriparatide. REFERENCES: Fleisch H. Bisphosphonates: mechanisms of action. Endocr Rev. 1998;19(1): Boivin G, Meunier PJ. Effects of bisphosphonates on matrix mineralization. J Musculoskel Neuron Interact. 2002;2(6): Eastell R, Christiansen C, Grauer A, et al. Effects of denosumab on bone turnover markers in postmenopausal osteoporosis. J Bone Miner Res. 2011;26(3): Bilezikian JP. Efficacy of bisphosphonates in reducing fracture risk in postmenopausal osteoporosis. Am J Med. 2009;122 (2)(suppl):S14-S21. Arlot M, Meunier PJ, Boivin G, et al. Differential effects of teriparatide and alendronate on bone remodeling in postmenopausal women assessed by histomorphometric parameters. J Bone Miner Res. 2005;20(7):12441253. Jiang Y, Zhao JJ, Mitlak BH, Wang O, Genant HK, Eriksen EF. Recombinant human parathyroid hormone (134) [teriparatide] improves both cortical and cancellous bone structure. J Bone Miner Res. 2003;18(11): Neer RM, Arnaud CD, Zanchetta JR, et al. Effect of parathyroid hormone (134) on fractures and bone mineral density in postmenopausal women with osteoporosis. N Engl J Med. 2001;344(19):
: Boivin G, Meunier PJ. Effects of bisphosphonates on matrix mineralization. J Musculoskel Neuron Interact. 2002;2(6): Eastell R, Christiansen C, Grauer A, et al. Effects of denosumab on bone turnover markers in postmenopausal osteoporosis. J Bone Miner Res. 2011;26(3): Bilezikian JP. Efficacy of bisphosphonates in reducing fracture risk in postmenopausal osteoporosis. Am J Med. 2009;122 (2)(suppl):S14-S21. Arlot M, Meunier PJ, Boivin G, et al. Differential effects of teriparatide and alendronate on bone remodeling in postmenopausal women assessed by histomorphometric parameters. J Bone Miner Res. 2005;20(7):12441253. Jiang Y, Zhao JJ, Mitlak BH, Wang O, Genant HK, Eriksen EF. Recombinant human parathyroid hormone (134) [teriparatide] improves both cortical and cancellous bone structure. J Bone Miner Res. 2003;18(11): Neer RM, Arnaud CD, Zanchetta JR, et al. Effect of parathyroid hormone (134) on fractures and bone mineral density in postmenopausal women with osteoporosis. N Engl J Med. 2001;344(19):")
10
Teriparatide 20 µg Pharmacokinetics
70 Teriparatide 20 µg Pharmacokinetics 60 Property Teriparatide value Absorption rate Rapid and extensive Time to peak serum concentration 30 minutes Absolute bioavailability 95% Serum Half-life (when given subcutaneously 60 minutes Metabolism Believed to occur in liver and kidneys Elimination rate Rapid – within 3 hours 50 40 Teriparatide concentration (pmol/L) 30 20 10 Upper Limit of Normal Endogenous PTH(1-84) 3 6 9 12 15 18 21 24 Time (Hours)
 Upper Limit of Normal. Endogenous PTH(1-84) Time (Hours)")
11
Clinical relevance and Adherence efficacy
Source: Review: Teriparatide: Clinical relevance and Adherence efficacy Reviewer Memo: For any questions regarding this slide kit, please contact Diane Stothard, Global Medical Education, Slide Modified: Memo:

12
Teriparatide increases Strength with hrQCT
Baseline 6 months 12 months 24 months Baseline Baseline 6 months 6 months 12 months 12 months 24 months 24 months Visualization of the microstructure and the treatment effect. Shown are 3 mm thick, central slices by QCT, from each visits in one patient treated with Teriparatide EUROFORS study. Graeff C et al,J Bone Miner Res 22: , 2007

13
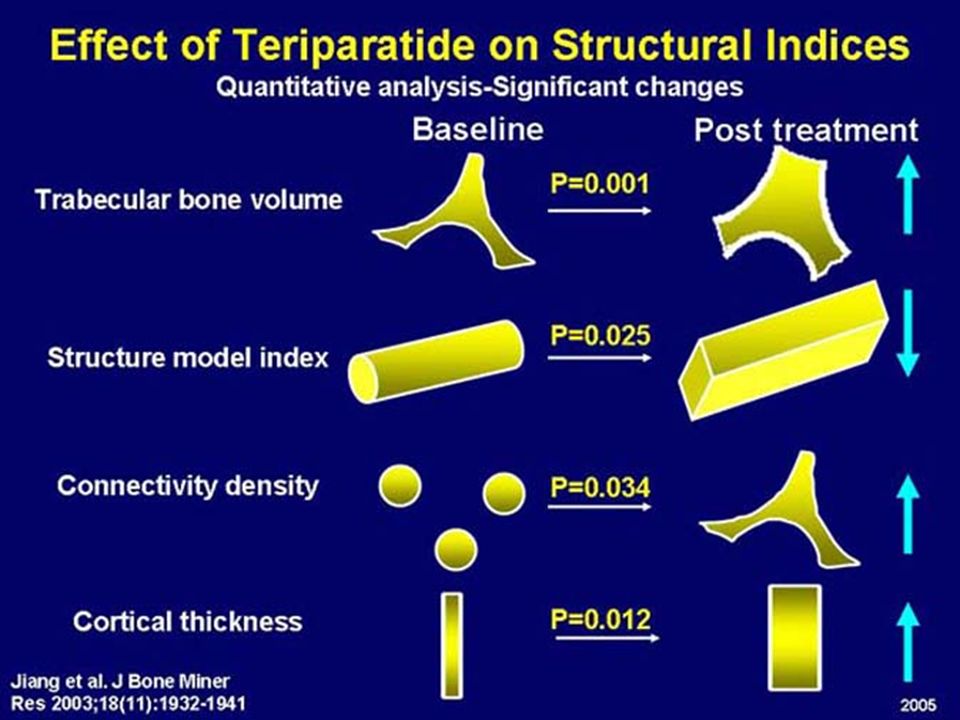
Teriparatide builds new bone
Treatment with teriparatide resulted in increased cortical thickness, trabecular bone volume, and connectivity, as well as the conversion of rods to plates. SPEAKER NOTES: The images are 3-D microCT reconstructions of paired iliac crest bone biopsies from a 65-year-old woman treated with 20 μg teriparatide. A change toward more plate-like morphology and an increase in cortical thickness were observed. The median increase in connectivity density (teriparatide, 19%; placebo, 14%), and median increase in cortical thickness (teriparatide, 22%; placebo, 3%) were found to be significant (P < .05) after teriparatide treatment. PRESENTATION TIPS: This is an opportunity to build consensus within the audience around the unique mechanism of action of teriparatide: teriparatide is the only therapeutic option for building new bone. This slide contains a link to a video clip that highlights the teriparatide mechanism of action. It may be accessed by clicking on the button in the bottom left corner of the slide. REFERENCE: Jiang Y, Zhao JJ, Mitlak BH, Wang O, Genant HK, Eriksen EF. Recombinant human parathyroid hormone (134) [teriparatide] improves both cortical and cancellous bone structure. J Bone Miner Res. 2003;18(11): Baseline Follow-up at 21 Months Paired Bone Biopsy Specimens Jiang Y, et al. J Bone Miner Res. 2003;18(11):
, and median increase in cortical thickness (teriparatide, 22%; placebo, 3%) were found to be significant (P < .05) after teriparatide treatment. PRESENTATION TIPS: This is an opportunity to build consensus within the audience around the unique mechanism of action of teriparatide: teriparatide is the only therapeutic option for building new bone. This slide contains a link to a video clip that highlights the teriparatide mechanism of action. It may be accessed by clicking on the button in the bottom left corner of the slide. REFERENCE: Jiang Y, Zhao JJ, Mitlak BH, Wang O, Genant HK, Eriksen EF. Recombinant human parathyroid hormone (134) [teriparatide] improves both cortical and cancellous bone structure. J Bone Miner Res. 2003;18(11): Baseline. Follow-up at 21 Months. Paired Bone Biopsy Specimens. Jiang Y, et al. J Bone Miner Res. 2003;18(11):")
14
Teriparatide Increases Cortical Bone Thickness
Superior Posterior Medial Baseline Cortical Thickness Map, mm 1 2 3 4 A: Inferomedial cortex B: Femoral neck C: Subcapital superior neck D: Gluteus medius E: Psoas major F: Quadratus femoris SPEAKER NOTES: Teriparatide treatment for 24 months increases cortical bone thickness at sites of compressive stress during locomotion, near key muscle attachments, and in the superior cortex, considered critical for hip fracture susceptibility. Sixty-nine women with severe osteoporosis from the European Study of Forsteo (EUROFORS) Trial were treated with teriparatide for 24 months, with quantitative CT scans at baseline and 24 months. All data from this cohort were analysed, with the exception of those femurs compromised by metalwork and those where one or both of the CT scans did not extend as far as the lesser trochanter. This yielded 119 femurs from 65 women. These figures are cortical thickness maps showing severe osteoporosis and the subsequent increase in thickness following teriparatide treatment. These are medial, superior, and posterior views of the average pre-treatment cortical thickness map in advanced osteoporosis showing remnants of thicker, highly loaded bone (blue/green) at (A) the inferomedial cortex and (B) the calcar femorale regions. Elsewhere, there is thin, submillimetre cortex (pink/red) at key fracture sites including (C) the subcapital superior neck region. Also labelled are the insertion sites of key muscles of locomotion: (D) gluteus medius; (E) psoas major; and (F) quadratus femoris (on the inter-trochanteric crest). The bottom figures are post-treatment percentage changes, which together indicate regeneration of bone at A, B, C, D, E, and F. PRESENTATION TIP: Teriparatide has positive effects not only on trabecular bone, but also on cortical bone. This graphic illustrates those effects in a subset of women from the EUROFORS trial. REFERENCE: Poole KES, Treece GM, Ridgway GR, Mayhew PM, Borggrefe J, Gee AH. Targeted regeneration of bone in the osteoporotic human femur. PLoS ONE. 2011;6(1):e16190. Change in Cortical Thickness, % -2 2 4 6 8 Poole KES, et al. PLoS ONE. 2011;6(1):e16190.
 Trial were treated with teriparatide for 24 months, with quantitative CT scans at baseline and 24 months. All data from this cohort were analysed, with the exception of those femurs compromised by metalwork and those where one or both of the CT scans did not extend as far as the lesser trochanter. This yielded 119 femurs from 65 women. These figures are cortical thickness maps showing severe osteoporosis and the subsequent increase in thickness following teriparatide treatment. These are medial, superior, and posterior views of the average pre-treatment cortical thickness map in advanced osteoporosis showing remnants of thicker, highly loaded bone (blue/green) at (A) the inferomedial cortex and (B) the calcar femorale regions. Elsewhere, there is thin, submillimetre cortex (pink/red) at key fracture sites including (C) the subcapital superior neck region. Also labelled are the insertion sites of key muscles of locomotion: (D) gluteus medius; (E) psoas major; and (F) quadratus femoris (on the inter-trochanteric crest). The bottom figures are post-treatment percentage changes, which together indicate regeneration of bone at A, B, C, D, E, and F. PRESENTATION TIP: Teriparatide has positive effects not only on trabecular bone, but also on cortical bone. This graphic illustrates those effects in a subset of women from the EUROFORS trial. REFERENCE: Poole KES, Treece GM, Ridgway GR, Mayhew PM, Borggrefe J, Gee AH. Targeted regeneration of bone in the osteoporotic human femur. PLoS ONE. 2011;6(1):e Change in Cortical Thickness, % Poole KES, et al. PLoS ONE. 2011;6(1):e")
15
Teriparatide Increases Tetracycline-Labelled New Bone at 6 and 18 months
Alendronate 6 Months 18 Months SPEAKER NOTES: These are 6-month versus 18-month bone biopsy data from the FACT trial. The Forsteo-Alendronate Comparator Trial (FACT) was a randomised, double-blind, active-comparator study comparing once-daily doses of 20 μg of teriparatide and 10 mg of oral alendronate in 203 postmenopausal women. The trial was composed of a 2-month screening phase and an 18-month treatment phase. A total of 641 postmenopausal women aged 45 to 84 years were screened. Of these, 203 patients were randomised to treatment. Patients received daily supplementation of both calcium (1000 mg) and vitamin D ( IU) throughout the study. Percentage change from baseline in areal and volumetric BMD at the lumbar spine and total hip, as well as markers of bone turnover, were the study end points. PRESENTATION TIPS: Dim the lights to view this slide. Stress the differences observed in new bone after teriparatide therapy (anabolic agent) versus alendronate therapy (antiresorptive agent). REFERENCE: Arlot M, Meunier PJ, Boivin G, et al. Differential effects of teriparatide and alendronate on bone remodeling in postmenopausal women assessed by histomorphometric parameters. J Bone Miner Res. 2005;20(7): Arlot M, et al. J Bone Miner Res. 2005;20(7): Permission for images from P. Meunier, 2006.
 was a randomised, double-blind, active-comparator study comparing once-daily doses of 20 μg of teriparatide and 10 mg of oral alendronate in 203 postmenopausal women. The trial was composed of a 2-month screening phase and an 18-month treatment phase. A total of 641 postmenopausal women aged 45 to 84 years were screened. Of these, 203 patients were randomised to treatment. Patients received daily supplementation of both calcium (1000 mg) and vitamin D ( IU) throughout the study. Percentage change from baseline in areal and volumetric BMD at the lumbar spine and total hip, as well as markers of bone turnover, were the study end points. PRESENTATION TIPS: Dim the lights to view this slide. Stress the differences observed in new bone after teriparatide therapy (anabolic agent) versus alendronate therapy (antiresorptive agent). REFERENCE: Arlot M, Meunier PJ, Boivin G, et al. Differential effects of teriparatide and alendronate on bone remodeling in postmenopausal women assessed by histomorphometric parameters. J Bone Miner Res. 2005;20(7): Arlot M, et al. J Bone Miner Res. 2005;20(7): Permission for images from P. Meunier,")
16
Teriparatide Increases lumbar spine BMD
16 14 12 10 8 6 4 2 P < .001 vs placebo at each time point SPEAKER NOTES: This is lumbar spine BMD data from the FPT. In the FPT, teriparatide 20 µg/d increased lumbar spine BMD significantly compared with placebo. Lumbar spine BMD increased significantly (P < .001) with teriparatide treatment at each visit where it was assessed, including at the first visit after 3 months. At study end point, the percent change in lumbar spine BMD was 9.7% in the teriparatide group versus 1.1% in the placebo group (P < .001). PRESENTATION TIPS: Key takeaway from this slide is not only the significant increase in BMD versus placebo, but also the rapid increase observed. Increases in lumbar spine BMD were significantly greater with teriparatide at every time point, including the first time point of 3 months. REFERENCES: Neer RM, Arnaud CD, Zanchetta JR, et al. Effect of parathyroid hormone (134) on fractures and bone mineral density in postmenopausal women with osteoporosis. N Engl J Med. 2001;344(19): Marcus R, Wang O, Satterwhite J, Mitlak B. The skeletal response to teriparatide is largely independent of age, initial bone mineral density, and prevalent vertebral fractures in postmenopausal women with osteoporosis. J Bone Miner Res. 2003;18(1):18-23. Neer RM, et al. N Engl J Med. 2001;344(19): Marcus R, et al. J Bone Miner Res. 2003;18(1):18-23.
 with teriparatide treatment at each visit where it was assessed, including at the first visit after 3 months. At study end point, the percent change in lumbar spine BMD was 9.7% in the teriparatide group versus 1.1% in the placebo group (P < .001). PRESENTATION TIPS: Key takeaway from this slide is not only the significant increase in BMD versus placebo, but also the rapid increase observed. Increases in lumbar spine BMD were significantly greater with teriparatide at every time point, including the first time point of 3 months. REFERENCES: Neer RM, Arnaud CD, Zanchetta JR, et al. Effect of parathyroid hormone (134) on fractures and bone mineral density in postmenopausal women with osteoporosis. N Engl J Med. 2001;344(19): Marcus R, Wang O, Satterwhite J, Mitlak B. The skeletal response to teriparatide is largely independent of age, initial bone mineral density, and prevalent vertebral fractures in postmenopausal women with osteoporosis. J Bone Miner Res. 2003;18(1): Neer RM, et al. N Engl J Med. 2001;344(19): Marcus R, et al. J Bone Miner Res. 2003;18(1):")
17
Teriparatide Increases femoral neck BMD
Teriparatide 20 μg Placebo 6 5 4 3 2 1 -1 -2 P < .001 vs placebo at each time point % Change ± SE SPEAKER NOTES: This is femoral neck BMD data from the FPT. In the FPT, teriparatide 20 µg/d increased femoral neck BMD significantly compared with placebo. REFERENCES: Neer RM, Arnaud CD, Zanchetta JR, et al. Effect of parathyroid hormone (134) on fractures and bone mineral density in postmenopausal women with osteoporosis. N Engl J Med. 2001;344(19): Marcus R, Wang O, Satterwhite J, Mitlak B. The skeletal response to teriparatide is largely independent of age, initial bone mineral density, and prevalent vertebral fractures in postmenopausal women with osteoporosis. J Bone Miner Res. 2003;18(1):18-23. 12 End Point 24 Months Neer RM, et al. N Engl J Med. 2001;344(19): Marcus R, et al. J Bone Miner Res. 2003;18(1):18-23.
 on fractures and bone mineral density in postmenopausal women with osteoporosis. N Engl J Med. 2001;344(19): Marcus R, Wang O, Satterwhite J, Mitlak B. The skeletal response to teriparatide is largely independent of age, initial bone mineral density, and prevalent vertebral fractures in postmenopausal women with osteoporosis. J Bone Miner Res. 2003;18(1): End. Point. 24. Months. Neer RM, et al. N Engl J Med. 2001;344(19): Marcus R, et al. J Bone Miner Res. 2003;18(1):")
18
% of women with >1 vertebral fracture
Fracture Prevention Trial Effect of Teriparatide on the Risk of New Vertebral Fractures Source: Neer et al. N Engl J Med 2001; 344: Li added: Table GHAC (Page 150). ARR: RMP.B3DSGJAC.SASPGM.EFS0042A 2 4 6 8 10 12 14 16 Placebo (64 / 448) TPTD20 (22 / 444) RR 65%* % of women with >1 vertebral fracture ARR = 9.33% Review: Li Xie 07/07/2003 WPDF global kit #LX200308c (Li Xie ) Review: J. Alam Reviewer Memo: Reviewed the reformatted slides and added detailed information to the source. Baseline factors for new vertebral fractures and values for serum 25-hydroxyvitamin-D were similar for all three groups (N=1326). The relative risk for one or more new vertebral fractures was reduced in the teriparatide-treated 20- and 40-g groups by 65% and 69%, respectively, compared with placebo. __________________ Neer RM, Arnaud CD, Zanchetta JR, Prince R, Gaich GA, Reginster JY et al. Effect of parathyroid hormone (1-34) on fractures and bone mineral density in postmenopausal women with osteoporosis. N Engl J Med 2001; 344(19): *P <0.001 vs. placebo RR = relative risk vs. placebo ARR = absolute risk reduction Neer et al. N Engl J Med 2001; 344(19): Slide Modified: on: 2/19/ :42:09 AM SL7 Rev: 217 on: 6/23/2003 1:15:38 PM SL45 Rev: 429 on: 6/24/2003 8:15:41 AM SL46 Rev: 437 on: 6/26/ :51:49 AM SL47 Rev: 458 on: 7/22/2003 7:27:21 PM SL3 Rev: 10 on: 9/4/2003 8:15:54 AM SL14 Rev: 69 on: 9/25/2003 6:38:58 PM SL1 Rev: 128 on: 10/18/2004 3:37:02 PM SL12 Rev: 19 Memo: Added new notes, modified slide per GP & JK, gave to MEP for recreating as object 23Jun03 - MR added RR = to asterisk text changed formatting to eliminate risk reduction second axis (MEP )
. ARR: RMP.B3DSGJAC.SASPGM.EFS0042A Placebo. (64 / 448) TPTD20. (22 / 444) RR 65%* % of women with >1 vertebral fracture. ARR = 9.33% Review: Li Xie 07/07/2003. WPDF global kit #LX200308c (Li Xie ) Review: J. Alam Reviewer Memo: Reviewed the reformatted slides and added detailed information to the source. Baseline factors for new vertebral fractures and values for serum 25-hydroxyvitamin-D were similar for all three groups (N=1326). The relative risk for one or more new vertebral fractures was reduced in the teriparatide-treated 20- and 40-g groups by 65% and 69%, respectively, compared with placebo. __________________. Neer RM, Arnaud CD, Zanchetta JR, Prince R, Gaich GA, Reginster JY et al. Effect of parathyroid hormone (1-34) on fractures and bone mineral density in postmenopausal women with osteoporosis. N Engl J Med 2001; 344(19): *P <0.001 vs. placebo. RR = relative risk vs. placebo. ARR = absolute risk reduction. Neer et al. N Engl J Med 2001; 344(19): Slide Modified: on: 2/19/ :42:09 AM SL7 Rev: 217 on: 6/23/2003 1:15:38 PM SL45 Rev: 429 on: 6/24/2003 8:15:41 AM SL46 Rev: 437 on: 6/26/ :51:49 AM SL47 Rev: 458 on: 7/22/2003 7:27:21 PM SL3 Rev: 10 on: 9/4/2003 8:15:54 AM SL14 Rev: 69. on: 9/25/2003 6:38:58 PM SL1 Rev: 128 on: 10/18/2004 3:37:02 PM SL12 Rev: 19. Memo: Added new notes, modified slide per GP & JK, gave to MEP for recreating as object 23Jun03 - MR added RR = to asterisk text. changed formatting to eliminate risk reduction second axis (MEP )")
19
Teriparatide Reduces the risk of Moderate/Severe Vertebral Fractures
ARR = 8.5% RRR = 90% P ≤ .001 vs placebo SPEAKER NOTES: The phase 3 registration trial for teriparatide in both the US and EU was the Fracture Prevention Trial (FPT). The objective of this trial was to assess teriparatide treatment in patients with moderate to severe osteoporosis. 1637 postmenopausal women from 99 centres in 17 countries who had a prior vertebral fracture were enrolled and assigned to either placebo, 20 g teriparatide, or 40 g teriparatide. Patients self-administered teriparatide (or placebo) by daily subcutaneous injection and supplemented this by taking both calcium and vitamin D throughout the trial. Occurrence of new vertebral or nonvertebral fracture was a primary end point. The other primary end points were changes to baseline BMD at 3, 6, 12, and 18 months, and the end of the study. BMD was measured in the lumbar spine, proximal femur, radius, and total body bone mineral. This graph shows how teriparatide 20 μg given once daily to postmenopausal women with osteoporosis for a median duration of 21 months reduced the risk of at least 1 moderate or severe vertebral fracture by 90%. PRESENTATION TIPS: Stress the importance of such a significant relative risk reduction for devastating moderate to severe vertebral fractures. This slide is a great opportunity for surprise building to relevance: the magnitude of the 90% RRR for moderate to severe fractures. REFERENCE: Neer RM, Arnaud CD, Zanchetta JR, et al. Effect of parathyroid hormone (1-34) on fractures and bone mineral density in postmenopausal women with osteoporosis. N Engl J Med. 2001;344(19): ARR, absolute risk reduction; RRR, relative risk reduction. Neer RM, et al. N Engl J Med. 2001;344(19):
. The objective of this trial was to assess teriparatide treatment in patients with moderate to severe osteoporosis postmenopausal women from 99 centres in 17 countries who had a prior vertebral fracture were enrolled and assigned to either placebo, 20 g teriparatide, or 40 g teriparatide. Patients self-administered teriparatide (or placebo) by daily subcutaneous injection and supplemented this by taking both calcium and vitamin D throughout the trial. Occurrence of new vertebral or nonvertebral fracture was a primary end point. The other primary end points were changes to baseline BMD at 3, 6, 12, and 18 months, and the end of the study. BMD was measured in the lumbar spine, proximal femur, radius, and total body bone mineral. This graph shows how teriparatide 20 μg given once daily to postmenopausal women with osteoporosis for a median duration of 21 months reduced the risk of at least 1 moderate or severe vertebral fracture by 90%. PRESENTATION TIPS: Stress the importance of such a significant relative risk reduction for devastating moderate to severe vertebral fractures. This slide is a great opportunity for surprise building to relevance: the magnitude of the 90% RRR for moderate to severe fractures. REFERENCE: Neer RM, Arnaud CD, Zanchetta JR, et al. Effect of parathyroid hormone (1-34) on fractures and bone mineral density in postmenopausal women with osteoporosis. N Engl J Med. 2001;344(19): ARR, absolute risk reduction; RRR, relative risk reduction. Neer RM, et al. N Engl J Med. 2001;344(19):")
20
Teriparatide Reduces the risk of Nonvertebral Fragility Fractures
ARR = 2.9% RRR = 53% P ≤ .05 vs placebo SPEAKER NOTES: In the FPT, the incidence of 1 or more new nonvertebral fractures (hip, radius, ankle, humerus, rib, foot, pelvis, and other sites) was a secondary end point. Nonvertebral fractures were classified as “fragility fractures” if, as determined by the local investigator, the associated trauma would not have resulted in the fracture of a normal bone (eg, falling from a standing height). The relative risk of ≥2 new nonvertebral fragility fractures was reduced in the teriparatide-treated 20-µg group by 53% compared with placebo. REFERENCE: Neer RM, Arnaud CD, Zanchetta JR, et al. Effect of parathyroid hormone (134) on fractures and bone mineral density in postmenopausal women with osteoporosis. N Engl J Med. 2001;344(19): ARR, absolute risk reduction; RRR, relative risk reduction. Neer RM, et al. N Engl J Med. 2001;344(19):
 was a secondary end point. Nonvertebral fractures were classified as fragility fractures if, as determined by the local investigator, the associated trauma would not have resulted in the fracture of a normal bone (eg, falling from a standing height). The relative risk of ≥2 new nonvertebral fragility fractures was reduced in the teriparatide-treated 20-µg group by 53% compared with placebo. REFERENCE: Neer RM, Arnaud CD, Zanchetta JR, et al. Effect of parathyroid hormone (134) on fractures and bone mineral density in postmenopausal women with osteoporosis. N Engl J Med. 2001;344(19): ARR, absolute risk reduction; RRR, relative risk reduction. Neer RM, et al. N Engl J Med. 2001;344(19):")
21
Antifracture Efficacy of Antiosteoporotic Agents
Incident vertebral fractures - Relative risk RR ± 95% CI RLX 60 (MORE)* RLX 60 (MORE)** ALN 5/10 (FIT1)* ALN 5/10 (FIT2)** RIS 5 (VERT - NA)* RIS 5 (VERT - MN)* CT 200 (PROOF)* Teriparatide 20µg Strontium ranelate (SOTI)* Strontium ranelate (SOTI + TROPOS)** 0.2 0.4 0.6 0.8 1.0 * with prevalent vertebral fracture ** without prevalent vertebral fracture Updated from Delmas, Lancet 2002 21
* RLX 60 (MORE)** ALN 5/10 (FIT1)* ALN 5/10 (FIT2)** RIS 5 (VERT - NA)* RIS 5 (VERT - MN)* CT 200 (PROOF)* Teriparatide 20µg. Strontium ranelate (SOTI)* Strontium ranelate (SOTI + TROPOS)** * with prevalent vertebral fracture. ** without prevalent vertebral fracture. Updated from Delmas, Lancet")
22
Antifracture Efficacy of Osteoporosis Agents
HORIZON-PFT Study 2301 Core Slides June-08 Antifracture Efficacy of Osteoporosis Agents Incident Vertebral Fractures RR±95% CI Incident Nonvertebral Fractures RR±95% CI RLX 60 (MORE)* RLX 60 (MORE)** CT 200 (PROOF)* Teriparatide 20µg* ALN 5/10 (FIT1)* ALN 5/10 (FIT2)** RIS 5 (VERT-NA)* RIS 5 (VERT-MN)* Strontium ranelate (SOTI)* (SOTI +TROPOS)** IBAN 2.5 *** IBAN intermittent (BONE) Zoledronic acid IV 0.6 1.0 0.2 RLX 60, 120 (MORE)*** RIS 2.5/5 (Hip Study)** (TROPOS)*** IBAN *With prevalent vertebral fracture(s) ; **Without prevalent vertebral fractures; ***With or without prevalent vertebral fractures; †Not from head-to-head studies Adapted from Delmas PD. Lancet. 2002;359:2018–26. CONFIDENTIAL HORIZON-PFT Slide Library - 22
* RLX 60 (MORE)** CT 200 (PROOF)* Teriparatide 20µg* ALN 5/10 (FIT1)* ALN 5/10 (FIT2)** RIS 5 (VERT-NA)* RIS 5 (VERT-MN)* Strontium ranelate. (SOTI)* (SOTI +TROPOS)** IBAN 2.5 *** IBAN intermittent. (BONE) Zoledronic acid IV RLX 60, 120 (MORE)*** RIS 2.5/5 (Hip Study)** (TROPOS)*** IBAN. *With prevalent vertebral fracture(s) ; **Without prevalent vertebral fractures; ***With or without prevalent vertebral fractures; †Not from head-to-head studies. Adapted from Delmas PD. Lancet. 2002;359:2018–26. CONFIDENTIAL. HORIZON-PFT Slide Library")
23
Pohl, et al. Arthritis Rheum 2003;48(Suppl 9):S234
Source: Data:RMP.SAS.B3DM.MCGHACSW.SUBMISS Program:RMP.B3DSGHAC.SASPGM(FRSN02JA) Abstract presented at ACR 2003: Pohl, et al. Effect of duration of teriparatide therapy on nonvertebral fracture risk. Arthritis Rheum 2003;48(Suppl 9):S234. The Longer the Duration of Treatment with Teriparatide, the Greater the Decrease in Risk for Nonvertebral Fragility Fractures Review: GMP200310A 2004 Update: J.Alam WPDF#ja200411a Reviewer Memo: N: Placebo=544 TPTD20=541 TPTD40=522 Post-menopausal women with osteoporosis and prevalent vertebral fracture were randomized to placebo (N=544), teriparatide 20 g (N=541) or teriparatide 40 g (N=552) once daily by subcutaneous injection for a median of 19 months (max 2 years). Rates of patients sustaining fracture diverged throughout the trial. In a Cox regression model treating time on therapy as a continuous time-dependent covariate, the hazard ratio (95% CI) for the combined teriparatide groups versus placebo decreased proportionally 9.1% (p=0.002) for each additional month of therapy, i.e., ( ). There is added clinical benefit with increased duration of teriparatide therapy throughout the 2 years studied in this trial. ___________________ Pohl G, Wang J, Scheele WH. Effect of duration of teriparatide therapy on nonvertebral fracture risk. Arthritis Rheum 2003;48(Suppl 9):S234. Pohl, et al. Arthritis Rheum 2003;48(Suppl 9):S234 Slide Modified: on: 10/29/2003 1:29:43 PM SL12 Rev: 171 Memo: New Notes 25Oct04 - MR
 Abstract presented at ACR 2003: Pohl, et al. Effect of duration of teriparatide therapy on nonvertebral fracture risk. Arthritis Rheum 2003;48(Suppl 9):S234. The Longer the Duration of Treatment with Teriparatide, the Greater the Decrease in Risk for Nonvertebral Fragility Fractures. Review: GMP200310A Update: J.Alam WPDF#ja200411a. Reviewer Memo: N: Placebo=544. TPTD20=541. TPTD40=522. Post-menopausal women with osteoporosis and prevalent vertebral fracture were randomized to placebo (N=544), teriparatide 20 g (N=541) or teriparatide 40 g (N=552) once daily by subcutaneous injection for a median of 19 months (max 2 years). Rates of patients sustaining fracture diverged throughout the trial. In a Cox regression model treating time on therapy as a continuous time-dependent covariate, the hazard ratio (95% CI) for the combined teriparatide groups versus placebo decreased proportionally 9.1% (p=0.002) for each additional month of therapy, i.e., ( ). There is added clinical benefit with increased duration of teriparatide therapy throughout the 2 years studied in this trial. ___________________. Pohl G, Wang J, Scheele WH. Effect of duration of teriparatide therapy on nonvertebral fracture risk. Arthritis Rheum 2003;48(Suppl 9):S234. Pohl, et al. Arthritis Rheum 2003;48(Suppl 9):S234. Slide Modified: on: 10/29/2003 1:29:43 PM SL12 Rev: 171. Memo: New Notes 25Oct04 - MR.")
25
Candidates for PTH Therapy
Postmenopausal women or men > 65 with severe osteoporosis T-score < -3.5 with Spine fracture 1 level T-score < -2.5 with fragility fractures (Hip or Spine 2 level) Patients who fail other osteoporosis therapies (2 years) New fracture in spite of compliance with therapy Decrease BMD in spine >3% or in hip > 5% C/I of BPs: GI mucosal irritation, bed ridden Most cause of BPs failure Poor compliance Inadequate Ca and Vit D
 Patients who fail other osteoporosis therapies (2 years) New fracture in spite of compliance with therapy. Decrease BMD in spine >3% or in hip > 5% C/I of BPs: GI mucosal irritation, bed ridden. Most cause of BPs failure. Poor compliance. Inadequate Ca and Vit D.")
26
Pretreatment Evaluation
Serum Ca, PO4, albumin Serum creatinine Serum alkaline phosphatase Serum PTH Serum uric acid 25-hydoxyvitamin D

27
What test should be done prior to starting therapy
What test should be done prior to starting therapy? Lab test & expected results Tests Disease Ca PO4 ALP PTH 25(OH)D osteoporosis N osteomalacia low high hyperparathyroidism Note: Creatinine is the must for all elderly
D. osteoporosis. N. osteomalacia. low. high. hyperparathyroidism. Note: Creatinine is the must for all elderly.")
28
Contraindication for PTH treatment
Children and adolescent Primary, secondary, tertiary hyperparathyroidism Renal insufficiency Paget’s disease Vitamin D deficiency Gout or significant hyperuricemia Hypercalcemia Prenancy or breast feeding Bone tumor or history of bone irradiation High alkaline phosphatase level

29
Adverse events Hypercalcemia Hypercalciuria
Occasional hypotension, Dizziness** Tachycardia Nausea Headache Hyperuricemia Muscle cramps**

30
Adverse Events Fracture Prevention Trial
Source: Data for Dizziness is from GHAC CSR (Table GHAC.12.3, Page 479); Data for nausea, Headache and Leg cramps is from GHAC study report (Table GHAC.12.2, Page 451); Table GHAC is for frequency of withdrawn for AE. Program for P-values: MC1STAT02/MC1STAT02.GRP/RMP/B3DS/GHAC/other/gsk_P-values_for AE (GHAC).sas; gsk_P-values_for AE dizziness (GHAC).sas. Adverse Events Fracture Prevention Trial Validation: Placebo (n=544) N (%) 33 (6) 41 (8) 45 (8) 6 (1) 32 (6) TPTD20 (n=541) N (%) 50 (9)* 51 (9) 44 (8) 17 (3) * 35 (7) TPTD40 (n=552) N (%) 44 (8) 98 (18)‡ 72 (13) * 13 (2) 59 (11) † Dizziness Nausea Headache Leg cramps Withdrawn for AE StatsMemo: Review: Li Xie 6/30/03; 8/5/03; 8/15/03 WPDF global kit #LX200308c (Li Xie ) In the fracture prevention trial, the overall treatment group difference in adverse events was not statistically significant at the 0.05 level (P=0.098). There was a statistically significant reduction (P=0.047) in the overall incidence of treatment-emergent adverse events in the teriparatide TPTD20/day treatment group, compared with placebo. There were no statistically significant differences or trends among treatment groups in the incidence of dizziness. Dizziness was the most commonly reported adverse event in the nervous system, with 33 (6.1%) patients in the placebo group, 50 (9.2%) patients in the TPTD20 group, and 44 (8.0%) patients in the TPTD40 group reporting dizziness (P=0.144). The frequencies of nausea and headache in the TPTD20 group were similar to placebo, 3% reported leg cramps. Participants reported significantly more nausea and headache in the TPTD40 group than in placebo (P<0.001). Incidences of leg cramps in the TPTD40 group were similar to placebo. One hundred twenty-six (7.7%) patients discontinued the study due to adverse events: 32 (5.9% of 544) in the placebo group, 35 (6.5% of 541) in the teriparatide TPTD20 treatment group, and 59 (10.7% of 552) in the teriparatide TPTD40 treatment group. _________________ Neer RM, Arnaud CD, Zanchetta JR, Prince R, Gaich GA, Reginster JY et al. Effect of parathyroid hormone (1-34) on fractures and bone mineral density in postmenopausal women with osteoporosis. N Engl J Med 2001; 344(19): Data on file, Eli Lilly and Company Reviewer Memo: * P<0.05, †P<0.01 , ‡ P<0.001 vs. Placebo Neer et al. N Engl J Med 2001; 344(19): Slide Modified: on: 1/22/2002 9:49:39 AM SL15 Rev: 250 on: 2/13/2002 7:01:47 PM SL15 Rev: 252 on: 2/19/ :42:14 AM SL16 Rev: 217 on: 6/26/ :53:12 AM SL92 Rev: 458 on: 9/4/ :23:40 AM SL15 Rev: 27 on: 9/25/2003 6:38:58 PM SL1 Rev: 128 Memo: modified notes, added to 03Jul03 - MR modified notes 11Aug03 - MR
; Data for nausea, Headache and Leg cramps is from GHAC study report (Table GHAC.12.2, Page 451); Table GHAC is for frequency of withdrawn for AE. Program for P-values: MC1STAT02/MC1STAT02.GRP/RMP/B3DS/GHAC/other/gsk_P-values_for AE (GHAC).sas; gsk_P-values_for AE dizziness (GHAC).sas. Adverse Events Fracture Prevention Trial. Validation: Placebo (n=544) N (%) 33 (6) 41 (8) 45 (8) 6 (1) 32 (6) TPTD20. (n=541) N (%) 50 (9)* 51 (9) 44 (8) 17 (3) * 35 (7) TPTD40. (n=552) N (%) 44 (8) 98 (18)‡ 72 (13) * 13 (2) 59 (11) † Dizziness. Nausea. Headache. Leg cramps. Withdrawn for AE. StatsMemo: Review: Li Xie 6/30/03; 8/5/03; 8/15/03. WPDF global kit #LX200308c (Li Xie ) In the fracture prevention trial, the overall treatment group difference in adverse events was not statistically significant at the 0.05 level (P=0.098). There was a statistically significant reduction (P=0.047) in the overall incidence of treatment-emergent adverse events in the teriparatide TPTD20/day treatment group, compared with placebo. There were no statistically significant differences or trends among treatment groups in the incidence of dizziness. Dizziness was the most commonly reported adverse event in the nervous system, with 33 (6.1%) patients in the placebo group, 50 (9.2%) patients in the TPTD20 group, and 44 (8.0%) patients in the TPTD40 group reporting dizziness (P=0.144). The frequencies of nausea and headache in the TPTD20 group were similar to placebo, 3% reported leg cramps. Participants reported significantly more nausea and headache in the TPTD40 group than in placebo (P<0.001). Incidences of leg cramps in the TPTD40 group were similar to placebo. One hundred twenty-six (7.7%) patients discontinued the study due to adverse events: 32 (5.9% of 544) in the placebo group, 35 (6.5% of 541) in the teriparatide TPTD20 treatment group, and 59 (10.7% of 552) in the teriparatide TPTD40 treatment group. _________________. Neer RM, Arnaud CD, Zanchetta JR, Prince R, Gaich GA, Reginster JY et al. Effect of parathyroid hormone (1-34) on fractures and bone mineral density in postmenopausal women with osteoporosis. N Engl J Med 2001; 344(19): Data on file, Eli Lilly and Company. Reviewer Memo: * P<0.05, †P<0.01 , ‡ P<0.001 vs. Placebo. Neer et al. N Engl J Med 2001; 344(19): Slide Modified: on: 1/22/2002 9:49:39 AM SL15 Rev: 250 on: 2/13/2002 7:01:47 PM SL15 Rev: 252 on: 2/19/ :42:14 AM SL16 Rev: 217 on: 6/26/ :53:12 AM SL92 Rev: 458 on: 9/4/ :23:40 AM SL15 Rev: 27. on: 9/25/2003 6:38:58 PM SL1 Rev: 128. Memo: modified notes, added to 03Jul03 - MR modified notes 11Aug03 - MR.")
31
Precautions and Side Effects of Teriparatide
Hypercalcemia & hypercalciuria Ca++ < 1500 mg/D Osteosarcoma (Rat) Duration < 2 years Dizziness, leg cramps Avoid concurrent Rx with bisphosphonates Sequential Rx after PTH discontinued is beneficial effects Hodsman AB et al. Endocrine Reviews 2005; 26:
 Duration < 2 years. Dizziness, leg cramps. Avoid concurrent Rx with bisphosphonates. Sequential Rx after PTH discontinued is beneficial effects. Hodsman AB et al. Endocrine Reviews 2005; 26:")
32
Combination therapy of Teriparatide with the other drug
Up to Date

34
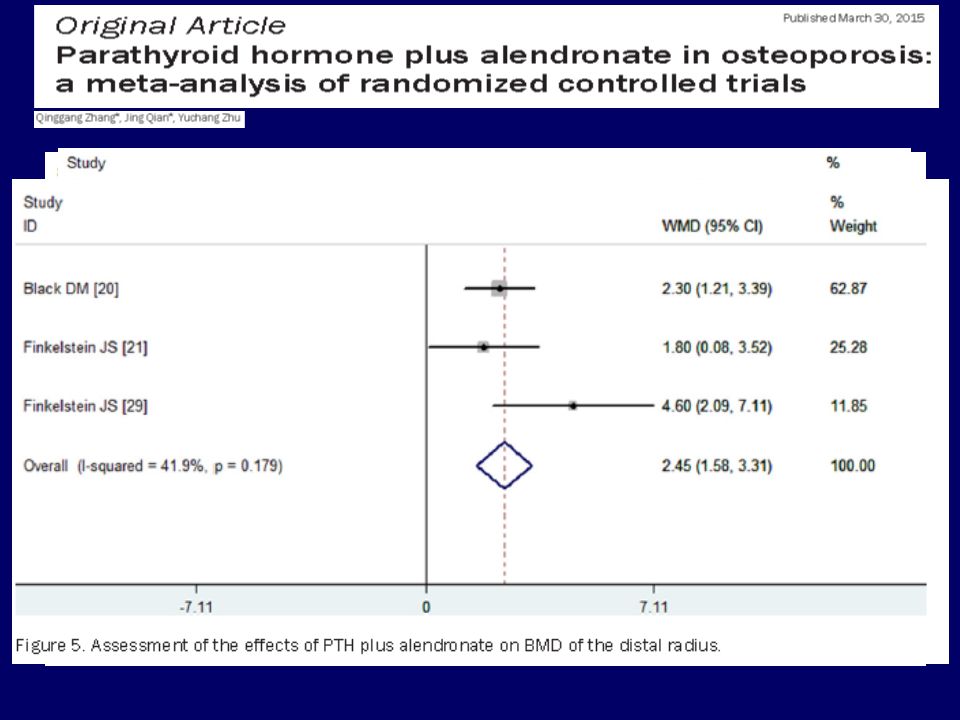
Conclusion: Our findings indicated that the addition of alendronate to PTH in the treatment of osteoporosis, reduced the ability of PTH therapy to increase the BMD at the lumbar spine, femoral neck, and total hip.

37
It supports the hypothesis that increased remodeling by TPTD increases Ct.Th and trabecular BMD by new bone deposits, which is associated with an increased porosity as reflected by the decreased CBMD.

40
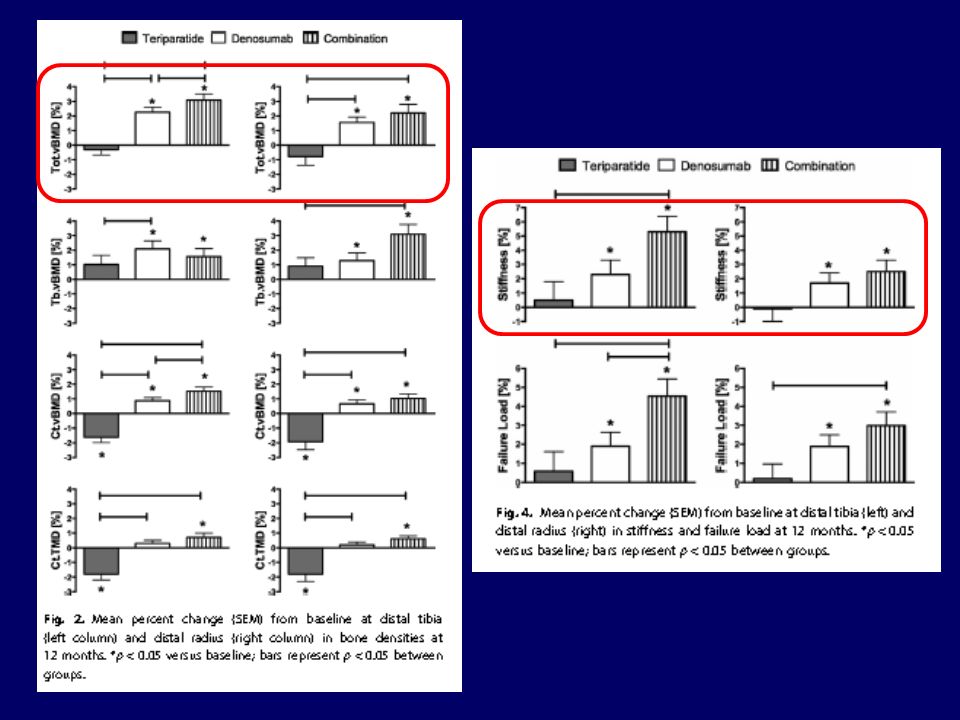
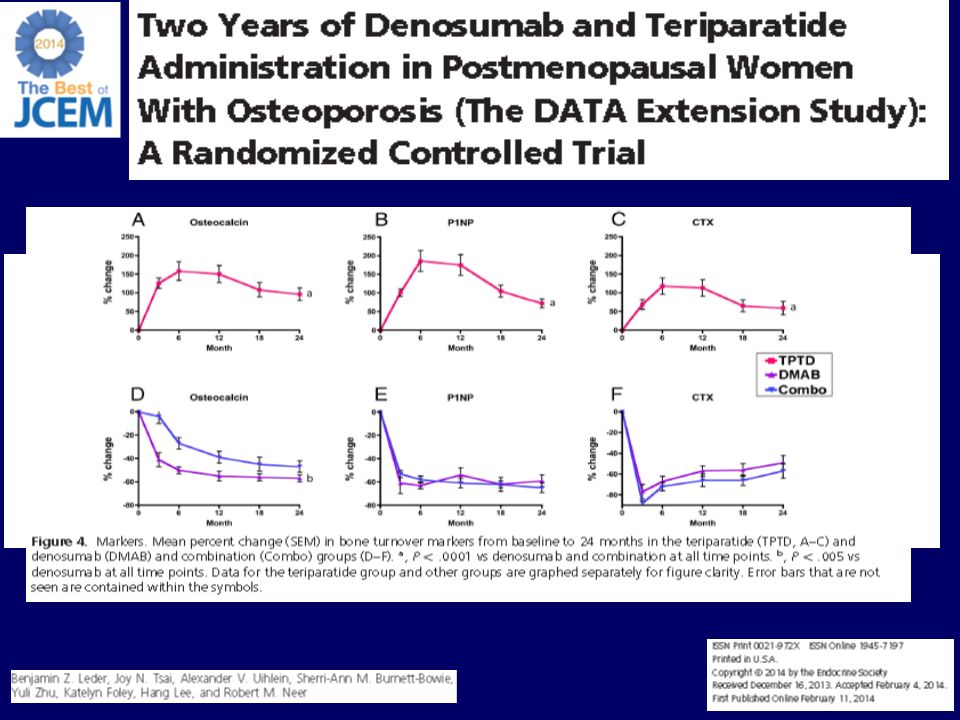
The results of this study demonstrate that 12 months of combined denosumab and teriparatide therapy improves peripheral cortical and total bone density, cortical micro-architecture, and estimated bone strength more than either drug alone. Although superior efficacy is noted at both the tibia and the radius in the combination group, the advantage of the combined treatment is numerically greater at the tibia than at the radius.

43
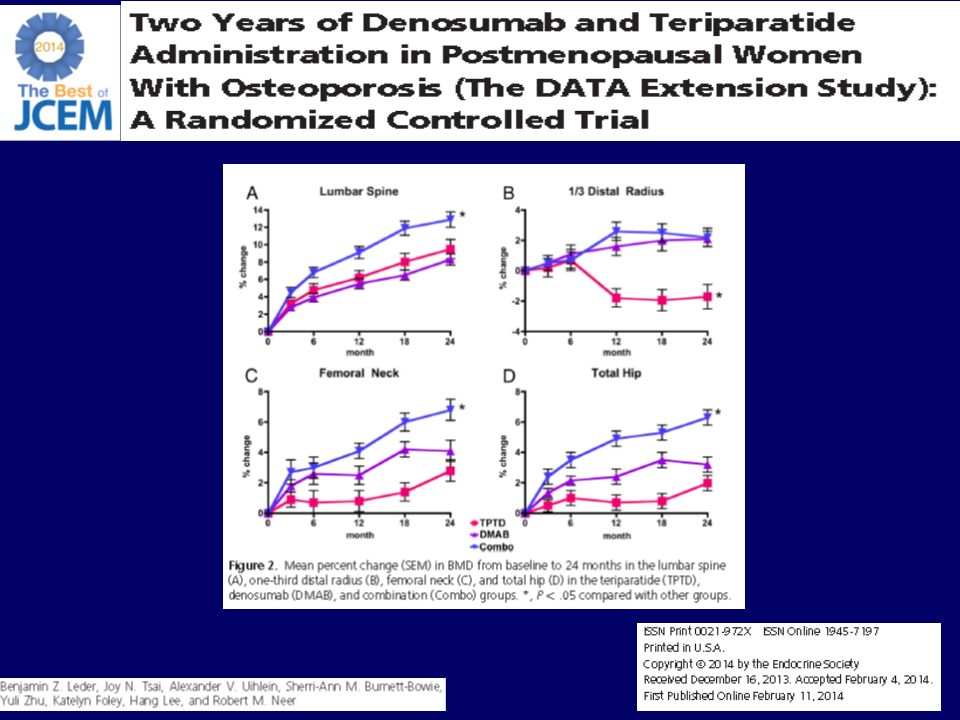
In summary, we have shown that 24 months of combined denosumab and teriparatide therapy increases BMD at the spine, hip, and femoral neck more than either drug alone and more than any currently available agent. Although a larger study would be needed to definitively demonstrate a fracture-reduction benefit.

44
Take home message Teriparatide is an anabolic therapy that builds new bone. Improves cancellous microarchitecture Increases cortical thickness and improves cortical bone geometry Teriparatide significantly reduces the risk of subsequent vertebral and nonvertebral fragility fractures in patients with osteoporosis: 65% RRR vs placebo for new vertebral fractures 90% RRR vs placebo for moderate/severe vertebral fractures 53% RRR vs placebo for all nonvertebral fragility fractures Teriparatide improves lumbar spine and femoral neck BMD

45
Drug combination PTH with SERM -> some paper support PTH with oral BPs -> not recommend (No synergistic) PTH with IV BPs -> early benefit primarily (6 mth) PTH with Denosumab -> studies ongoing (Benefit) After PTH months -> Must use antiresoptive drug
 PTH with Denosumab -> studies ongoing (Benefit) After PTH months -> Must use antiresoptive drug.")
46
Police General hospital

Similar presentations










 FOSALAN (alendronate) is a trademark.>")
>")












 on Aromatase Inhibitor-Associated Bone Loss in Postmenopausal Women with Early Breast Cancer Receiving Adjuvant Letrozole:>")