Download presentation
Presentation is loading. Please wait.

1
Management of pleural infection in adults: British Thoracic Society pleural disease guideline 2010 Helen E Davies, Robert J O Davies, Christopher W H Davies, on behalf of the BTS Pleural Disease Guideline Group Thorax 2010;65(Suppl 2): ii41 - ii53 R3 박지영
: ii41 - ii53 R3 박지영")
2
INTRODUCTION Pleural infection is a frequent clinical problem ~80,000 cases/year in the UK and USA patients with empyema 20% die 20% require surgery to recover Prompt evaluation and therapeutic intervention Reduce morbidity and mortality as well as healthcare costs The results of a systematic literature review combined with expert opinion of the preferred management of pleural infection in adults for clinicians Specifically do not cover in detail the complex areas of tuberculous empyema, paediatric empyema or the surgical management of post- pneumonectomy space infection

4
Epidemiology The overall incidence of pleural infection is increasing 4,424 patients with pleural infection : increase in incidence of 2.8%/year Farjah F et al. Thorac Cardiovasc Surg 2007;133:346-51 11,294 patients with pleural infection (1995 and 2003) : incidence rate ratio (IRR) of 2.2 <19 years old 1.23 >19 years old Finley et al. Can Respir J 2008;15:85-9
 : incidence rate ratio (IRR) of 2.2 <19 years old 1.23 >19 years old Finley et al. Can Respir J 2008;15:85-9.")
5
Pathophysiology ‘Simple’ self-resolving parapneumonic pleural effusion ‘complicated’ multiloculated fibrinopurulent collection associated with clinical and/or biochemical features of sepsis The development of empyema in association with pneumonia (1)simple exudate (2)fibrinopurulent stage (3)later organising stage with scar tissue (pleural peel) formation
simple exudate (2)fibrinopurulent stage (3)later organising stage with scar tissue (pleural peel) formation")
6
early exudative stage capillary vascular permeability↑ fluid movement into the pleural space proinflammatory cytokines ↑ (IL-8, TNF-α) facilitate fluid entry free-flowing exudate : WBC↓, LDH < serum ½ normal pH, glucose levels treatment with antibiotics fibrinopurulent stage bacterial invasion immune response ↑ further migration of neutrophils activation of the coagulation cascade procoagulant ↑ fibrinolytic activity ↓ organising phase fibroblasts ↑ preventing re-expansion impairing lung function creating a persistent pleural space with continuing potential for infection
 facilitate fluid entry free-flowing exudate : WBC↓, LDH < serum ½ normal pH, glucose levels treatment with antibiotics fibrinopurulent stage bacterial invasion immune response ↑ further migration of neutrophils activation of the coagulation cascade procoagulant ↑ fibrinolytic activity ↓ organising phase fibroblasts ↑ preventing re-expansion impairing lung function creating a persistent pleural space with continuing potential for infection")
7
pleural fluid culture (-) in 40%
 in 40%")
8
LITERATURE EVIDENCE & EXPERT OPINION Respiratory specialist care A chest physician or thoracic surgeon should be involved in the care of all patients requiring chest tube drainage for pleural infection. (C) Nutrition Clinicians should ensure adequate nutrition in patients with pleural infection. (C) Thrombosis prophylaxis in pleural infection All patients with pleural infection are at high risk for the development of venous thromboembolism and should receive adequate thrombosis prophylaxis with heparin unless contraindicated. (A)
 Nutrition Clinicians should ensure adequate nutrition in patients with pleural infection. (C) Thrombosis prophylaxis in pleural infection All patients with pleural infection are at high risk for the development of venous thromboembolism and should receive adequate thrombosis prophylaxis with heparin unless contraindicated. (A).")
9
LITERATURE EVIDENCE & EXPERT OPINION Identification: clinical Features of ongoing sepsis and raised CRP in patients with pneumonia after ≥3 days may indicate progression to pleural infection. (C) seven clinical variables : predicting development of pleural infection COPD :↓ Positive predictive value: using two or more points (1) albumin 100 mg/l, (3) platelet count >400x10 /l, (4) sodium <130 mmol/l, (5) intravenous drug abuse, (6) chronic alcohol abuse Chalmers JD et al. Thorax 2009;64:556-8 All patients with suspected pleural infection should have blood cultures for aerobic and anaerobic bacteria performed. (C) positive in about 14% of patients with pleural infection 9
 seven clinical variables : predicting development of pleural infection COPD :↓ Positive predictive value: using two or more points (1) albumin 100 mg/l, (3) platelet count >400x10 /l, (4) sodium <130 mmol/l, (5) intravenous drug abuse, (6) chronic alcohol abuse Chalmers JD et al. Thorax 2009;64:556-8 All patients with suspected pleural infection should have blood cultures for aerobic and anaerobic bacteria performed. (C) positive in about 14% of patients with pleural infection 9.")
10
LITERATURE EVIDENCE & EXPERT OPINION Identification: imaging Ultrasound homogeneous echogenic effusions empyema or hemorrhage CT scanning to differentiate pleural empyema from a parenchymal lung abscess ‘split pleura’ pleural thickening : 86-100% of empyemas 56% of exudative parapneumonic effusions MRI no advantage over CT allergy to contrast agents chest wall involvement with the infection

12
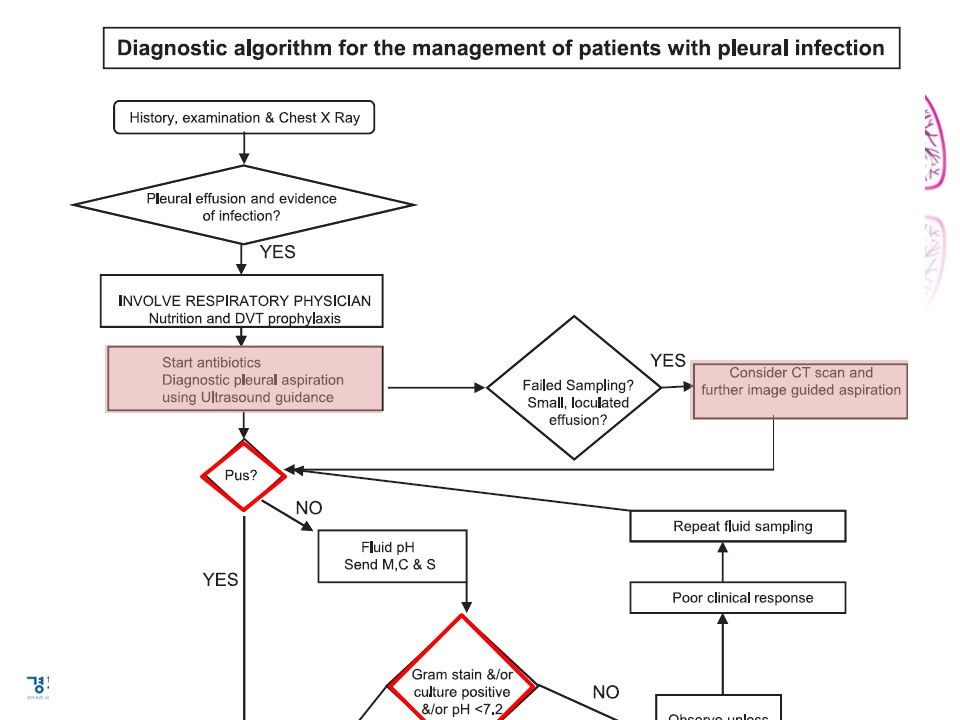
LITERATURE EVIDENCE & EXPERT OPINION Identification: pleural fluid aspiration All patients with a pleural effusion in association with sepsis or a pneumonic illness require diagnostic pleural fluid sampling. (C) pleural effusion >10 mm Pleural fluid pH should be assessed in all non-purulent effusions when pleural infection is suspected. (B) pleural fluid pH of <7.2 If pleural fluid pH measurement is not available, pleural fluid glucose assessment should be performed where pleural infection is possible. (B) pleural fluid glucose level <3.4 mmol/l DDx : Rheumatoid effusions
 pleural effusion >10 mm Pleural fluid pH should be assessed in all non-purulent effusions when pleural infection is suspected. (B) pleural fluid pH of <7.2 If pleural fluid pH measurement is not available, pleural fluid glucose assessment should be performed where pleural infection is possible. (B) pleural fluid glucose level <3.4 mmol/l DDx : Rheumatoid effusions.")
13
LITERATURE EVIDENCE & EXPERT OPINION Indications for pleural fluid drainage in pleural infection Patients with frankly purulent or turbid/cloudy pleural fluid on sampling should receive prompt pleural space chest tube drainage. (B) The presence of organisms identified by Gram stain and/or culture from a non-purulent pleural fluid sample indicates that pleural infection is established and should lead to prompt chest tube drainage. (B) Pleural fluid pH <7.2 in patients with suspected pleural infection indicates a need for chest tube drainage. (B)
 The presence of organisms identified by Gram stain and/or culture from a non-purulent pleural fluid sample indicates that pleural infection is established and should lead to prompt chest tube drainage. (B) Pleural fluid pH <7.2 in patients with suspected pleural infection indicates a need for chest tube drainage. (B).")
14
LITERATURE EVIDENCE & EXPERT OPINION Parapneumonic effusions that do not fulfil any of these criteria for chest tube drainage could be treated with antibiotics alone provided clinical progress is good. (B) Poor clinical progress during treatment with antibiotics alone should lead to prompt patient review, repeat pleural fluid sampling and probably chest tube drainage. (B) Patients with a loculated pleural collection should receive early chest tube drainage. (C) Large non-purulent effusions could be drained by aspiration and/or chest tube if required for symptomatic benefit. (C)
 Poor clinical progress during treatment with antibiotics alone should lead to prompt patient review, repeat pleural fluid sampling and probably chest tube drainage. (B) Patients with a loculated pleural collection should receive early chest tube drainage. (C) Large non-purulent effusions could be drained by aspiration and/or chest tube if required for symptomatic benefit. (C).")
15
LITERATURE EVIDENCE & EXPERT OPINION Chest tube drainage A small-bore catheter 10-14 F will be adequate for most cases of pleural infection. However, there is no consensus on the size of the optimal chest tube for drainage. (C) small-bore cath : easier, less traumatic to insert, comfortable If a small-bore flexible catheter is used, regular flushing is recommended to avoid catheter blockage. (C) Chest tube insertion should be performed under imaging guidance wherever possible. (D)
 small-bore cath : easier, less traumatic to insert, comfortable If a small-bore flexible catheter is used, regular flushing is recommended to avoid catheter blockage. (C) Chest tube insertion should be performed under imaging guidance wherever possible. (D).")
16
LITERATURE EVIDENCE & EXPERT OPINION Antibiotics All patients should receive antibiotics targeted to treat the bacterial profile of modern pleural infection and based on local antibiotic policies and resistance patterns. (B) Antibiotics to cover anaerobic infection should be used in all patients except those with culture proven pneumococcal infection. (B) Macrolide antibiotics are not indicated unless there is objective evidence for or a high clinical index of suspicion of ‘atypical’ pathogens. (B) Where possible, antibiotic choice should be guided by bacterial culture results and advice from a microbiologist. (B)
 Antibiotics to cover anaerobic infection should be used in all patients except those with culture proven pneumococcal infection. (B) Macrolide antibiotics are not indicated unless there is objective evidence for or a high clinical index of suspicion of ‘atypical’ pathogens. (B) Where possible, antibiotic choice should be guided by bacterial culture results and advice from a microbiologist. (B).")
17
LITERATURE EVIDENCE & EXPERT OPINION Penicillins, penicillins combined with b-lactamase inhibitors, metronidazole and cephalosporins penetrate the pleural space well. Aminoglycosides should be avoided. (B) AG: poor penetration into the pleural space inactive in the presence of pleural fluid acidosis When bacterial cultures are negative, antibiotics should cover both common community-acquired bacterial pathogens and anaerobic organisms. (B) β-lactam+β-lactamase inhibitor clindamycin : good penetration of the infected pleural space Empirical antibiotic treatment for hospital-acquired empyema should include treatment for MRSA and anaerobic bacteria. (B)
 AG: poor penetration into the pleural space inactive in the presence of pleural fluid acidosis When bacterial cultures are negative, antibiotics should cover both common community-acquired bacterial pathogens and anaerobic organisms. (B) β-lactam+β-lactamase inhibitor clindamycin : good penetration of the infected pleural space Empirical antibiotic treatment for hospital-acquired empyema should include treatment for MRSA and anaerobic bacteria. (B).")
18
LITERATURE EVIDENCE & EXPERT OPINION Intravenous antibiotics should be changed to oral therapy once there is clinical and objective evidence of improvement in sepsis. (D) Intrapleural antibiotics are not recommended. (D) Prolonged courses of antibiotics may be necessary and can often be administered as an outpatient after discharge. (D) at least 3 weeks : based on clinical, biochemical, radiological response
 Intrapleural antibiotics are not recommended. (D) Prolonged courses of antibiotics may be necessary and can often be administered as an outpatient after discharge. (D) at least 3 weeks : based on clinical, biochemical, radiological response.")
19
LITERATURE EVIDENCE & EXPERT OPINION Intrapleural fibrinolytics There is no indication for the routine use of intrapleural fibrinolytics in patients for pleural infection. (A)
.")
20
LITERATURE EVIDENCE & EXPERT OPINION Persistent sepsis and pleural collection Patients with persistent sepsis and a residual pleural collection should undergo further radiological imaging. (C) Patients with persistent sepsis and a residual pleural collection should be discussed with a thoracic surgeon to consider all possible surgical options available. (D)
 Patients with persistent sepsis and a residual pleural collection should be discussed with a thoracic surgeon to consider all possible surgical options available. (D).")
21
LITERATURE EVIDENCE & EXPERT OPINION Patients with persistent sepsis Patients should receive surgical treatment if they have persisting sepsis in association with a persistent pleural collection, despite chest tube drainage and antibiotics. (C) Failure of chest tube drainage and antibiotics should prompt early discussion with a thoracic surgeon. (C)
 Failure of chest tube drainage and antibiotics should prompt early discussion with a thoracic surgeon. (C).")
22
LITERATURE EVIDENCE & EXPERT OPINION The choice of antibiotic should be reviewed and a prolonged course administered where appropriate. (D) A thoracic surgeon should be involved in assessment of suitability for anaesthesia. Less radical surgical interventions including rib resection and placement of a large-bore drain may be considered in frail patients depending on surgical expertise and access and can be performed in some cases under local anaesthetic or with epidural anaesthesia. (C)
 A thoracic surgeon should be involved in assessment of suitability for anaesthesia. Less radical surgical interventions including rib resection and placement of a large-bore drain may be considered in frail patients depending on surgical expertise and access and can be performed in some cases under local anaesthetic or with epidural anaesthesia. (C).")
23
LITERATURE EVIDENCE & EXPERT OPINION In patients with ineffective effusion drainage and persistent sepsis who are unable to tolerate general anaesthesia, re-imaging of the thorax and placement of a further image-guided small-bore catheter, a largerbore chest tube or intrapleural fibrinolytic could be considered after discussion with a thoracic surgeon. (D) For some patients, palliative treatment and active symptom control measures will be appropriate. (D)
 For some patients, palliative treatment and active symptom control measures will be appropriate. (D).")
24
LITERATURE EVIDENCE & EXPERT OPINION Bronchoscopy Bronchoscopy should only be performed in patients where there is a high index of suspicion of bronchial obstruction. (C) mass, volume loss on radiographic imaging history of possible foreign body Follow-up All patients with empyema and pleural infection require outpatient follow-up. (D) often within 4 weeks following discharge
 mass, volume loss on radiographic imaging history of possible foreign body Follow-up All patients with empyema and pleural infection require outpatient follow-up. (D) often within 4 weeks following discharge.")
25
LITERATURE EVIDENCE & EXPERT OPINION Prognosis in pleural infection The long-term survival of patients with pleural infection is good if prompt treatment is initiated Deaths : usually due to comorbid conditions, not directly due to sepsis from the empyema Long-term sequelae of pleural empyema residual pleural thickening (up to 13% of patients) pleural calcification, bronchopleural fistula formation
 pleural calcification, bronchopleural fistula formation")
Similar presentations