Download presentation
Presentation is loading. Please wait.

1
Earica Y. Silla Year Level IV SBCM

2
33 y/o G2P1 (0100) Married Catholic Taguig City 1 st admissionlast March 2, 2011
 Married Catholic Taguig City 1 st admissionlast March 2, 2011")
3
Right lower quadrant pain

4
LMP: September 8, 2010 EDC: June 15, 2011 AOG: G2P1 (0100) Abdominal pregnancy 32 weeks 3/7 days AOG by LMP, NIL (+) intermittent RLQ pain, pressing in nature non- radiating 7/ 10 Assoc w/ fetal movts Slightly relieved by rest Sought consult at QMMC OB- ER Admitted for close observation and monitoring.
 Abdominal pregnancy 32 weeks 3/7 days AOG by LMP, NIL (+) intermittent RLQ pain, pressing in nature non- radiating 7/ 10 Assoc w/ fetal movts Slightly relieved by rest Sought consult at QMMC OB- ER Admitted for close observation and monitoring.")
5
Complete PNCU – private clinic in Taguig MVT and FeSO4 5 mos PTA vaginal spotting vague hypogastric pains Sought consult and was admitted at a private clinic for 4 days and was given unrecalled medications. She was the referred to PGH afterwards. Patient also reported to have UTI twice and took Cefuroxime and Cotrimoxazole for 7 days. At PGH, she diagnosed to have fetal death in utero and was subjected to trial of labor. She was then advised by her uncle to have a second opinion and was referred to QMMC.

6
Past Medical History The patient has no previous surgeries and hospitalizations. She also has no history of Diabetes, Hypertension, Tuberculosis, Asthma, Goiter, Heart problems, Allergies or previous blood transfusion. Family History Unremarkable Personal Social History Patient owns a small sari- sari store in Taguig. Patient has no history of smoking, drinking alcoholic beverages and illicit drug use.

7
14 years old Regular 3- 5 days 2-4 pads/ day No associated symptoms

8
23 years of age 1 partner 2-3x/ week no contraceptives used No associated symptoms

9
G2P1 (0100) G1- 2001, NSD, Fabella, preterm
 G , NSD, Fabella, preterm")
10
General: (+) weight loss (-) easy fatigability CNS: (-) loss of consciousness, headache HEENT: (-) blurring of vision, eye pain, tinnitus, ear pain, epistaxis, sorethroat RESP: (-) difficulty of breathing, (-) cough, (- ) colds CVS: (-) chest pain, (-) palpitations GIT: (-) vomiting, (-) constipation GUT: (-) dysuria, (-) hematuria, (-) oliguria M/S: (-) limitation of movement, (-) joint pain
 weight loss (-) easy fatigability CNS: (-) loss of consciousness, headache HEENT: (-) blurring of vision, eye pain, tinnitus, ear pain, epistaxis, sorethroat RESP: (-) difficulty of breathing, (-) cough, (- ) colds CVS: (-) chest pain, (-) palpitations GIT: (-) vomiting, (-) constipation GUT: (-) dysuria, (-) hematuria, (-) oliguria M/S: (-) limitation of movement, (-) joint pain")
11
GENERAL SURVEY: conscious, cooperative, coherent, ambulatory and not in active labor VITAL SIGNS: BP: 100/70 mmHg PR: 98 bpm RR: 20 bpm T: 37.4 C Skin: Skin is warm and moist to touch. No clubbing, cyanosis.

12
HEENT: Head. Normocephalic, atraumatic, no mass, tenderness or scalp lesions. Fine black well- distributed hair. Eyes. Pupils are both equal and reactive to light. Normal extraocular eye movements. No lid lag. Pinkish palpebral conjunctiva, anicteric sclerae, clear cornea. Ears: Hearing is good. No tenderness or ear discharge. Nose. Nasal mucosa is pink, symmetrical, septum not deviated. No deformities, lesions. Mouth and Pharynx. No lesions. Tongue not deviated on protrusion. Tonsils not inflamed. Uvula at midline. Neck: Symmetrical. Thyroid gland not palpable. Trachea at midline. No abnormalities in neck movement. Thorax and Lungs: No lessions, mass, scar or tenderness. Symmetrical expansion, resonant on percussion, clear breath sounds, vesicular breath heard on all lung fields. No adventitious sounds. Cardiovascular: Adynamic precordium, PMI at 5 th intercostal space. No heaves, thrills. Normal rate. Regular rhythm. Good S1 and S2. No murmur or extra heart sound. Abdomen: Abdomen is globular. (+) striae gravidarum (+) linea nigra FH: 26 cms FHT: 135 (doppler) Extremities: Pink nail beds. No edema. Pulses are full and equal. Musculoskeletal: No joint deformities. Good range of motion of hands, wrist, elbows, shoulders, hips, knees, ankles. (+) low back pains
 striae gravidarum (+) linea nigra FH: 26 cms FHT: 135 (doppler) Extremities: Pink nail beds. No edema. Pulses are full and equal. Musculoskeletal: No joint deformities. Good range of motion of hands, wrist, elbows, shoulders, hips, knees, ankles. (+) low back pains.")
13
Admitting Diagnosis: G2P1 (0100) ABDOMINAL PREGNANCY 24 5/7 WEEKS AOG BY LMP; 23 4/7 WEEKS AOG BY LUTZ, NIL On Admission: VITAL SIGNS BP: 110/80 PR: 81 RR: 20 Temp: afebrile FH: 18 cmsFHT: 140IE: soft and closed Plan: Admit the patient For observation Close monitoring of both the mother and the baby
 ABDOMINAL PREGNANCY 24 5/7 WEEKS AOG BY LMP; 23 4/7 WEEKS AOG BY LUTZ, NIL On Admission: VITAL SIGNS BP: 110/80 PR: 81 RR: 20 Temp: afebrile FH: 18 cmsFHT: 140IE: soft and closed Plan: Admit the patient For observation Close monitoring of both the mother and the baby")
14
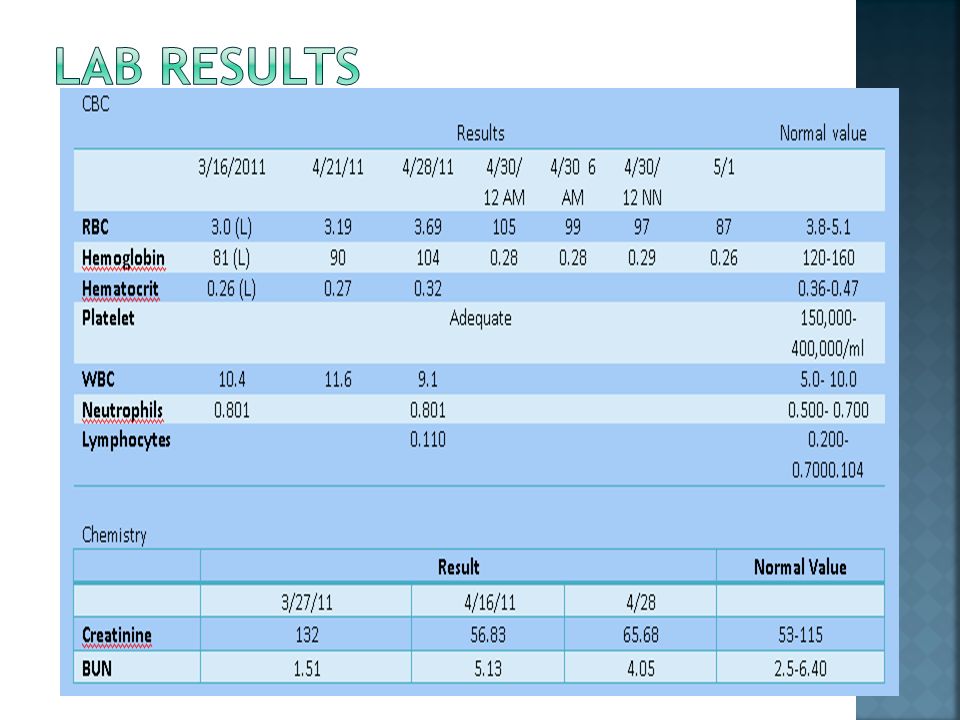
Patient was admitted for observation and monitoring and was put on a daily EFM order. She continued her MVT’s and FeSo4. She was also reported to have intermittent fever while in the wards (38- 40) which was relieved by paracetamol intake. She was also referred to Internal Medicine for co- management when her creatinine levels reached 132. Impression given was AKI secondary to hypovolemia. Her baseline FHT from the daily EFM was 135- 140. Good fetal movements were also noted until the night of April 28, 2011 when she complained of hypogastric pain accompanied by epigastric pain. No fetal movement was noted on UTZ hence subjecting the patient to operation. The patient underwent exploratory laparotomy to remove the dead fetus. Payient had 4L blood loss and was transfused with two(2) units pRBC and four (4) units FFP.
 which was relieved by paracetamol intake. She was also referred to Internal Medicine for co- management when her creatinine levels reached 132. Impression given was AKI secondary to hypovolemia. Her baseline FHT from the daily EFM was Good fetal movements were also noted until the night of April 28, 2011 when she complained of hypogastric pain accompanied by epigastric pain. No fetal movement was noted on UTZ hence subjecting the patient to operation. The patient underwent exploratory laparotomy to remove the dead fetus. Payient had 4L blood loss and was transfused with two(2) units pRBC and four (4) units FFP..")
15
FeSo4 1 tab OD Macrodantin 10 mg BID Trihemic acid tab OD Paracetamol 500 mg/tab: T ≥ 38 q4 Cefuroxime 750 mg TIV q8 Ceftriaxone 1 g IV OD Dexamethasone 6 mg/ IM LD q12 x 4 doses

18
3/14/11 Abdominal Pregnancy, cephalic presentation with placenta anterior and superior. No gross fetal anomaly Secere hydronephrosis on the rt. Side and moderate on the left side due to ureteral compression by fetus and uterus. 3/24/11 Abdominal pregnancy with good cardiac and somatic activities 27 weeks by Fetal biometry. Placenta Rt Lateral Grade 2, Adequate amniotic fluid.

19
Is a rare type of ectopic pregnancy where the conceptus implants into the peritoneal cavity instead of the uterine walls. usual sites of implantation : pelvic cul de sac broad ligament bowel pelvic side wall

21
1: 10,000 live births 1.4% of ectopic pregnancies

22
Primary abdominal pregnancy is very rare and results from intra abdominal fertilization of sperm and ovum. Secondary type is said to be due to tubal rupture where the conceptus is expelled and re- implanted anywhere in the peritoneal cavity where it can establish adequate circulation, survive and grow.

23
Spotting severe abdominal pain Pelvic and uterine changes

24
Life-threatening Clinical management depends on the gestational age at diagnosis. In-hospital expectant management if pregnancy is diagnosed after 24 weeks Partial placental separation can develop spontaneously or in the course of the operation. If it is obvious that the placenta can be safely removed, or if there is already hemorrhage from its implantation site, then removal begins immediately. Leaving the placenta in place represents the lesser of two evils. This decreases the chance of immediate life- threatening hemorrhage, but at the expense of long-term sequelae. Unfortunately, when left in the abdominal cavity, the placenta commonly causes infection with abscesses, adhesions, intestinal obstruction, and wound dehiscence

25
Maternal mortality is increased substantively compared with normal pregnancy. With appropriate preoperative planning, however, maternal mortality has been reduced from approximately 20 percent to less than 5 percent in the past 20 years.

Similar presentations







 Male Filipino Roman Catholic Sampaloc, Manila Informant: Mother Reliability: Good.>")





>")








