Download presentation
Presentation is loading. Please wait.

1
Pazopanib in Advanced Ovarian Cancer: A new galloping horse. Dr. Raafat Ragaie, MD,FRCR

2
Ovarian Cancer: Why the Anti-Angiogenesis ? Tumor angiogenesis is associated with malignant behavior in ovarian cancer 1,2 BEV as single-agent showed promising activity in recurrent ovarian cancer in phase II studies 3,4 BEV combined with chemotherapy showed positive results in phase III randomized clinical trials in both platinum sensitive (OCEANS) 5 as well as platinum resistant ovarian cancer (AURELIA) 6 1 Hollingsworth et al. Am J Pathol 1995;147:33–41 2 Burger et al. J Clin Oncol 2007;25:2902–8 3 Burger et al. J Clin Oncol 2007;25:5165–71 4 Cannistra et al. J Clin Oncol 2007;25:5180–6 5 C Aghajanian, et al. ASCO 2011 6 Pujade-Lauraine et al. ASCO 2012
 5 as well as platinum resistant ovarian cancer (AURELIA) 6 1 Hollingsworth et al. Am J Pathol 1995;147:33–41 2 Burger et al. J Clin Oncol 2007;25:2902–8 3 Burger et al. J Clin Oncol 2007;25:5165–71 4 Cannistra et al. J Clin Oncol 2007;25:5180–6 5 C Aghajanian, et al. ASCO Pujade-Lauraine et al. ASCO")
3
CG + PL OCEANS: Study schema CG for 6 (up to 10) cycles Stratification variables: Platinum-free interval (6–12 vs >12 months) Cytoreductive surgery for recurrent disease (yes vs no) Platinum-sensitive recurrent OC a Measurable disease ECOG 0/1 No prior chemo for recurrent OC No prior BV (n=484) BV = bevacizumab; PL = placebo a Epithelial ovarian, primary peritoneal, or fallopian tube cancer G 1000 mg/m 2, d1 & 8 C AUC 4 PL q3w until progression C AUC 4 BV 15 mg/kg q3w until progression G 1000 mg/m 2, d1 & 8 CG + BV C Aghajanian, et al ASCO 2011
 cycles Stratification variables: Platinum-free interval (6–12 vs >12 months) Cytoreductive surgery for recurrent disease (yes vs no) Platinum-sensitive recurrent OC a Measurable disease ECOG 0/1 No prior chemo for recurrent OC No prior BV (n=484) BV = bevacizumab; PL = placebo a Epithelial ovarian, primary peritoneal, or fallopian tube cancer G 1000 mg/m 2, d1 & 8 C AUC 4 PL q3w until progression C AUC 4 BV 15 mg/kg q3w until progression G 1000 mg/m 2, d1 & 8 CG + BV C Aghajanian, et al ASCO 2011")
4
OCEANS: PFS by IRC CG + PL (n=242) CG + BV (n=242) Events, n (%) 148 (61)119 (49) Median PFS, months (95% CI) 8.6 (8.3–10.2) 12.3 (10.7–14.6) Stratified analysis HR (95% CI) Log-rank p-value 0.451 (0.351–0.580) <0.0001 1.0 0.8 0.6 0.4 0.2 0 Proportion progression free 0612182430 24216831830CG + PL 242195732270CG + BV Months No. at risk C Aghajanian, et al. ASCO 2011

5
OCEANS: Interim OS 1.0 0.8 0.6 0.4 0.2 0 Proportion alive 0 Months 612303642 No. at risk: 1824 2422351952680CG + PL13177 2422382004280CG + BV14682 CG + PL (n=242) CG + BV (n=242) Events, n (%)78 (32)63 (26) Median OS, months (95% CI) 29.9 (26.4–NE) 35.5 (30.0–NE) Stratified analysis HR (95% CI) Log-rank p-value 0.751 (0.537–1.052) 0.094 a NE = not estimable a p-value does not cross pre-specified boundary of 0.001 C Aghajanian, et al ASCO 2011
 CG + BV (n=242) Events, n (%)78 (32)63 (26) Median OS, months (95% CI) 29.9 (26.4–NE) 35.5 (30.0–NE) Stratified analysis HR (95% CI) Log-rank p-value (0.537–1.052) a NE = not estimable a p-value does not cross pre-specified boundary of C Aghajanian, et al ASCO")
6
AURELIA trial design Stratification factors: Chemotherapy selected Prior anti-angiogenic therapy Treatment-free interval (<3 vs 3 ‒ 6 months from previous platinum to subsequent PD) Platinum-resistant OC a ≤2 prior anticancer regimens No history of bowel obstruction/abdominal fistula, or clinical/ radiological evidence of rectosigmoid involvement Treat to PD/toxicity Investigator’s choice (without BEV) Optional BEV monotherapy c BEV 15 mg/kg q3w b + chemotherapy Chemotherapy R 1:1 Chemotherapy options (investigator’s choice): Paclitaxel 80 mg/m 2 days 1, 8, 15, & 22 q4w Topotecan 4 mg/m 2 days 1, 8, & 15 q4w (or 1.25 mg/m 2, days 1–5 q3w) PLD 40 mg/m 2 day 1 q4w Pujade-Lauraine et al ASCO 2012
 Platinum-resistant OC a ≤2 prior anticancer regimens No history of bowel obstruction/abdominal fistula, or clinical/ radiological evidence of rectosigmoid involvement Treat to PD/toxicity Investigator’s choice (without BEV) Optional BEV monotherapy c BEV 15 mg/kg q3w b + chemotherapy Chemotherapy R 1:1 Chemotherapy options (investigator’s choice): Paclitaxel 80 mg/m 2 days 1, 8, 15, & 22 q4w Topotecan 4 mg/m 2 days 1, 8, & 15 q4w (or 1.25 mg/m 2, days 1–5 q3w) PLD 40 mg/m 2 day 1 q4w Pujade-Lauraine et al ASCO 2012")
7
Progression-free survival Median duration of follow-up: 13.9 months (CT arm) vs 13.0 months (BEV + CT arm) CT (n=182) BEV + CT (n=179) Events, n (%) 166 (91%)135 (75%) Median PFS, months (95% CI) 3.4 (2.2 ‒ 3.7) 6.7 (5.7 ‒ 7.9) HR (unadjusted) (95% CI) Log-rank p-value (2-sided, unadjusted) 0.48 (0.38 ‒ 0.60) <0.001 1.0 0.8 0.6 0.4 0.2 0 Estimated probability 0612182430 Time (months) 18237 810 179881810 CT BEV + CT No. at risk: 93 140 20 49 1 4 0 1 3.46.7 Pujade-Lauraine et al ASCO 2012

8
Ovarian Cancer : Why the Anti-Angiogenesis ? VEGF-associated tumor angiogenesis in ovarian cancer is associated with malignant behavior 1 BEV as single-agent showed promising activity in phase II recurrent ovarian cancer studies BEV combined with chemotherapy showed positive results in phase III randomized clinical trials in both platinum sensitive (OCEANS) 2 as well as platinum resistant ovarian cancer (AURELIA) 3 Two Phase III randomized clinical trials studied BEV in 1 st line treatment as maintenance: –GOG 218 4 –ICON7 5 1 Hollingsworth et al. Am J Pathol 1995;147:33–41 2 C Aghajanian, et al. ASCO 2011 3 Pujade-Lauraine et al. ASCO 2012 4 Buerger et al ASCO, 2010 5 Perren, et al. NEJM 2011
 2 as well as platinum resistant ovarian cancer (AURELIA) 3 Two Phase III randomized clinical trials studied BEV in 1 st line treatment as maintenance: –GOG –ICON7 5 1 Hollingsworth et al. Am J Pathol 1995;147:33–41 2 C Aghajanian, et al. ASCO Pujade-Lauraine et al. ASCO Buerger et al ASCO, Perren, et al. NEJM")
9
9 GOG-0218: Schema Front-line: Epithelial OV, PP or FT cancer Stage III optimal (macroscopic) Stage III suboptimal Stage IV n=1800 (planned) Front-line: Epithelial OV, PP or FT cancer Stage III optimal (macroscopic) Stage III suboptimal Stage IV n=1800 (planned) Stratification variables: GOG performance status (PS) Stage/debulking status RANDOMIZERANDOMIZE RANDOMIZERANDOMIZE 1:1:1 15 months Paclitaxel (P) 175 mg/m 2 Carboplatin (C) AUC 6 Placebo I Arm Cytotoxic (6 cycles) Maintenance (16 cycles) (CP) Carboplatin (C) AUC 6 Paclitaxel (P) 175 mg/m 2 Placebo BEV 15 mg/kg II (CP + BEV) BEV 15 mg/kg Carboplatin (C) AUC 6 Paclitaxel (P) 175 mg/m 2 III (CP + BEV BEV) Buerger et al ASCO, 2010
 Stage III suboptimal Stage IV n=1800 (planned) Front-line: Epithelial OV, PP or FT cancer Stage III optimal (macroscopic) Stage III suboptimal Stage IV n=1800 (planned) Stratification variables: GOG performance status (PS) Stage/debulking status RANDOMIZERANDOMIZE RANDOMIZERANDOMIZE 1:1:1 15 months Paclitaxel (P) 175 mg/m 2 Carboplatin (C) AUC 6 Placebo I Arm Cytotoxic (6 cycles) Maintenance (16 cycles) (CP) Carboplatin (C) AUC 6 Paclitaxel (P) 175 mg/m 2 Placebo BEV 15 mg/kg II (CP + BEV) BEV 15 mg/kg Carboplatin (C) AUC 6 Paclitaxel (P) 175 mg/m 2 III (CP + BEV BEV) Buerger et al ASCO, 2010")
10
CP (Arm I) Arm I CP (n=625) Patients with event, n (%) 423 (67.7) Median PFS, months10.3 Stratified analysis HR (95% CI) One-sided p-value (log rank) GOG-0218: PFS + BEV (Arm II) a p-value boundary = 0.0116 + BEV → BEV maintenance (Arm III) Proportion surviving progression free Months since randomization 1.0 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 0 0122436 Arm III CP + BEV BEV (n=623) 360 (57.8) 14.1 0.717 (0.625–0.824) <0.0001 a 10 Arm II CP + BEV (n=625) 418 (66.9) 11.2 0.908 (0.759–1.040) 0.080 a
 Arm I CP (n=625) Patients with event, n (%) 423 (67.7) Median PFS, months10.3 Stratified analysis HR (95% CI) One-sided p-value (log rank) GOG-0218: PFS + BEV (Arm II) a p-value boundary = BEV → BEV maintenance (Arm III) Proportion surviving progression free Months since randomization Arm III CP + BEV BEV (n=623) 360 (57.8) (0.625–0.824) < a 10 Arm II CP + BEV (n=625) 418 (66.9) (0.759–1.040) a")
11
GOG-0218: OS Analysis At time of final PFS analysis Arm I CP (n=625) Arm II CP + BEV (n=625) Arm III CP + BEV BEV (n=623) Patients with events, n (%) 156 (25.0) 150 (24.0) 138 (22.2) Median, months39.338.739.7 HR a (95% CI) 1.036 (0.827–1.297) 0.915 (0.727–1.152) One-sided p-value0.3610.252 Proportion alive Months since randomization 1.0 0.9 0.8 0.7 0.6 0.5 0.4 0.3 0.2 0.1 0 012243648 11 625/625/623442/432/437173/162/17146/39/40 No. at risk

12
12 Adverse event (grade when limited), n (%) Arm I CP (n=601) Arm II CP + BEV (n=607) Arm III CP + BEV BEV (n=608) Hypertension (grade ≥2)43 (7.2) b 100 (16.5) b 139 (22.9) b Proteinuria (grade ≥3) 4 (0.7) 10 (1.6) Neutropenia (grade ≥4)347 (57.7)384 (63.3)385 (63.3) Febrile neutropenia21 (3.5)30 (4.9)26 (4.3) Venous thromboembolic event35 (5.8)32 (5.3)41 (6.7) Arterial thromboembolic event 5 (0.8)4 (0.7) GOG-0218: Select Adverse Events Onset between cycle 2 and 30 days after date of last treatment RPLS = reversible posterior leukoencephalopathy syndrome a Perforation/fistula/necrosis/leak b p<0.05
, n (%) Arm I CP (n=601) Arm II CP + BEV (n=607) Arm III CP + BEV BEV (n=608) Hypertension (grade ≥2)43 (7.2) b 100 (16.5) b 139 (22.9) b Proteinuria (grade ≥3) 4 (0.7) 10 (1.6) Neutropenia (grade ≥4)347 (57.7)384 (63.3)385 (63.3) Febrile neutropenia21 (3.5)30 (4.9)26 (4.3) Venous thromboembolic event35 (5.8)32 (5.3)41 (6.7) Arterial thromboembolic event 5 (0.8)4 (0.7) GOG-0218: Select Adverse Events Onset between cycle 2 and 30 days after date of last treatment RPLS = reversible posterior leukoencephalopathy syndrome a Perforation/fistula/necrosis/leak b p<0.05")
13
GL/AVAO/1110/0027a RANDOMISERANDOMISE ICON7: scheme Stratification variables: Stage and extent of debulking: I–III debulked ≤1cm vs stage I–III debulked >1cm vs stage IV and inoperable stage III Timing of intended treatment start: ≤ vs > 4 weeks after surgery GCIG group (*also choice of AUC dose 5 [AGO, NSGO, GINECO] or 6) Paclitaxel 175mg/m 2 Carboplatin AUC5 or 6* Paclitaxel 175mg/m 2 1:1 Stage I–IIa (grade 3 or clear cell) or Stage IIb–IV (all grades/ histologic types) debulked ≤1 cm or >1 cm OC, PP, FTC (n=1,528) Bevacizumab 7.5mg/kg q3w 12 months CP CP + B7.5 B7.5 Perren, et al. NEJM 2011
![GL/AVAO/1110/0027a RANDOMISERANDOMISE ICON7: scheme Stratification variables: Stage and extent of debulking: I–III debulked ≤1cm vs stage I–III debulked >1cm vs stage IV and inoperable stage III Timing of intended treatment start: ≤ vs > 4 weeks after surgery GCIG group (*also choice of AUC dose 5 [AGO, NSGO, GINECO] or 6) Paclitaxel 175mg/m 2 Carboplatin AUC5 or 6* Paclitaxel 175mg/m 2 1:1 Stage I–IIa (grade 3 or clear cell) or Stage IIb–IV (all grades/ histologic types) debulked ≤1 cm or >1 cm OC, PP, FTC (n=1,528) Bevacizumab 7.5mg/kg q3w 12 months CP CP + B7.5 B7.5 Perren, et al.](http://images.slideplayer.com/36/10579144/slides/slide_13.jpg "NEJM")
14
GL/AVAO/1110/0027a ICON7: PFS CP CP + B7.5 B7.5 PFS estimate Number at risk CP764474221390 CP + B7.5764599229270 B7.5 CP CP + B7.5 B7.5 Events, n (%) 464 (61)470 (62) Median, months 17.419.8 Log-rank testp=0.039 HR (95% CI)0.87 (0.77–0.99) 1.0 0.8 0.6 0.4 0.2 0 Time (months) 0612182430364248 Perren, et al. NEJM 2011 Data cut-off date: November 30, 2010

15
GL/AVAO/1110/0027a ICON7: OS Number at risk CP7647246726234212127160 CP + B7.5 7647377026574592286940 B7.5 1.00 0.75 0.50 0.25 0 Time (months) 0612182430364248 OS estimate CP CP + B7.5 B7.5 Events, n (%) 200 (26)178 (23) Median, months Not yet reached Log-rank testp=0.11 HR (95% CI)0.85 (0.69–1.04) 1-year OS rate (%)9295 Perren, et al. NEJM 2011 Data cut-off date: November 30, 2010

16
Pazopanib

17
Targeting Angiogenesis by targeting VEGFR and PDGFR Inhibition of progression ↑ VEGF↑ PDGF Vascular permeability Cell survival, proliferation Vascular formation, maturation VEGFRPDGFR VEGF PDGF Vascular Endothelial Cell Pericyte/Fibroblast/ Vascular Smooth Muscle Pericyte/Fibroblast/ Vascular Smooth Muscle Pazopanib Sorafenib Sunitinib Axitinib Bevacizumab

19
[TITLE] Du Bois et al, ASCO 2013
![[TITLE] Du Bois et al, ASCO 2013](http://images.slideplayer.com/36/10579144/slides/slide_19.jpg "[TITLE] Du Bois et al, ASCO 2013")
20
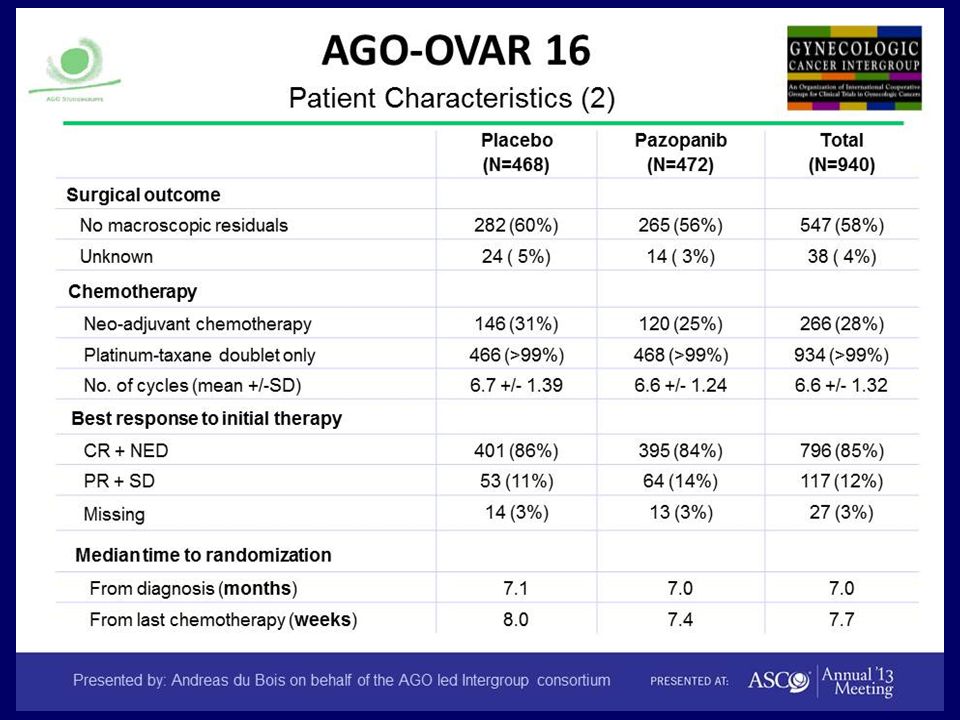
[TITLE]
![[TITLE]](http://images.slideplayer.com/36/10579144/slides/slide_20.jpg "[TITLE]")
22
PFS: AGO-OVAR 16 Du Bois et al, ASCO 2013

23
[TITLE] AGO-OVAR 16 :OS Du Bois et al, ASCO 2013
![[TITLE] AGO-OVAR 16 :OS Du Bois et al, ASCO 2013](http://images.slideplayer.com/36/10579144/slides/slide_23.jpg "[TITLE] AGO-OVAR 16 :OS Du Bois et al, ASCO 2013")
24
[TITLE] AGO-OVAR 16 :Adverse Events Du Bois et al, ASCO 2013
![[TITLE] AGO-OVAR 16 :Adverse Events Du Bois et al, ASCO 2013](http://images.slideplayer.com/36/10579144/slides/slide_24.jpg "[TITLE] AGO-OVAR 16 :Adverse Events Du Bois et al, ASCO 2013")
25
[TITLE]
![[TITLE]](http://images.slideplayer.com/36/10579144/slides/slide_25.jpg "[TITLE]")
26
KASO INTERPRETATION Anti-Angiogenesis will PROBABLY CLICK In Ovarian Cancer Pazopanib provided the best data set for improvement of PFS ? YES However: no OS gain ? Yet Toxicity / including financial toxicity

27
Thank you For your attention

Similar presentations









 in combination with chemotherapy: pivotal metastatic breast cancer survival data 1.>")



 Treated with Anti Vascular Endothelial Growth Factor (VEGF)>")
 All P values vs. placebo Adapted from Miles et al. ASCO 2008, abstract LBA 1011.>")



>")
