Download presentation
Presentation is loading. Please wait.

2
Hiroshima, Japan), 2010 and July 2012, the new shunt tube was used in 100 consecutive patients undergoing OPCABG new coronary shunt tube was easily implanted in nearly all (97.2%) target vessels. All 100 cases were performed completely during off-pump operation (MIDCABG) in 28 patients transsternal OPCABG in 72 patients.
 in 28 patients transsternal OPCABG in 72 patients..")
3
cardiothoracic ratio > 0.7) Hemodynamically unstable patients Patients with critical left main disease. acute myocardial infarction LVEF < 35%

6
total of 202 arterial graft anastomoses Postoperative angiographies were performed within 2 weeks outflow blood weight with a pressure head of 1,000 mm H 2 O using bovine blood in order to determine flow capacity of the shunt tube

8
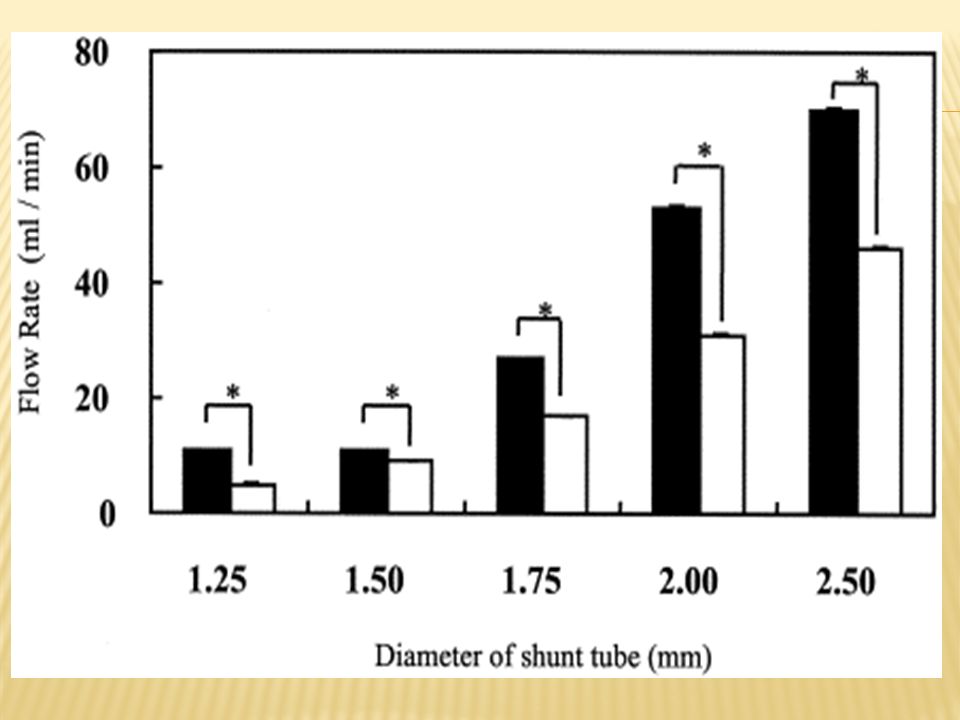
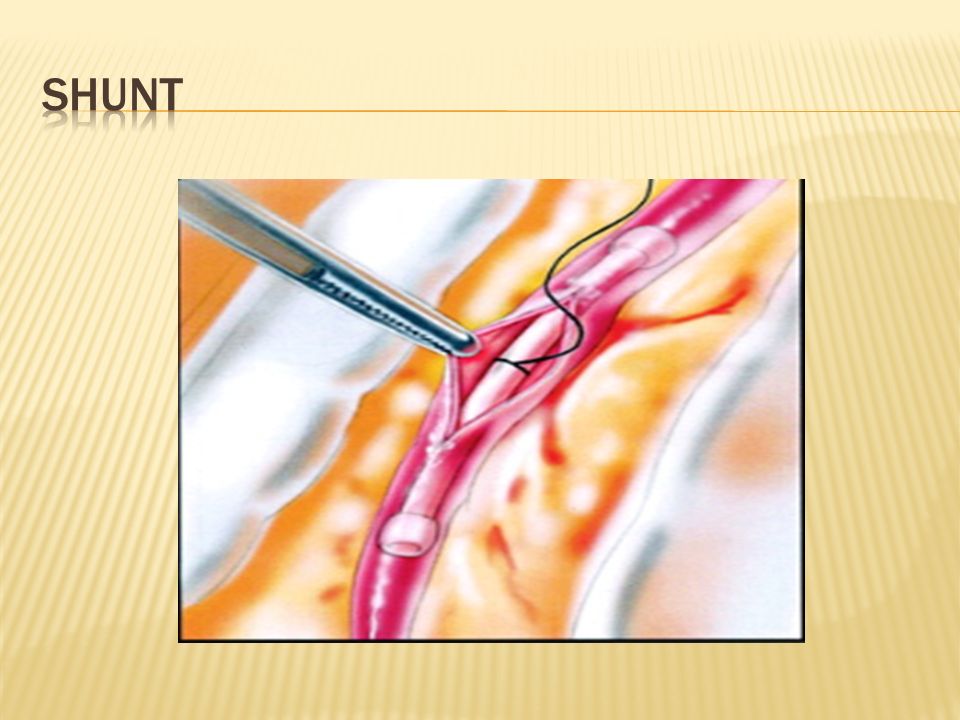
a wedge-shaped head and polyamide guidewire facilitate insertion do adequate kinking and restoring insertion easy and safe coated with heparin, preventing thrombosis and injury to coronary endothelial cells. good rates of blood flow according to diameter

10
Flow rates were measured in bovine blood under conditions as follows: hematocrit 33%, hemoglobin 12.1 g/dL, total protein 5.2 g/dL, temperature 25°C to 27°C, pressure head 1,000 mm H 2 O.

11
Postoperative angiography was performed on all 100 cases. The patency rate was 99.5% for arterial grafts and 96.2% for vein grafts. String signs were observed in 3 arterial grafts Anastomotic stenoses were found in 2 cases No new stenoses occurred in native coronary vessels

12
some surgeons now use intraluminal coronary shunts Success of coronary shunting during revascularization reached 97.2% significantly greater capacity for blood flow compared with the standard shunt tube. hemodyanamic instabilities and ischemic changes on electrocardiography occur in 10% of OPCABG operations after the snaring procedure. However, all these instabilities disappeared after implantation of the coronary shunt tube

13
Although OPCABG is recognized as less invasive than conventional coronary artery bypass grafting, the procedure is somewhat invasive, particularly to the coronary endothelium. Technical devices such as coronary snaring, shunting, and gas insufflation required to obtain optimal operative fields can cause lesions to the endothelium leading to coronary endothelial dysfunction, platelet aggregation, intimal dissection, and plaque ruptur

15
reduces the need for snares clamping gas insufflation coronary shunting could possibly ameliorate coronary endothelial injury

17
Bristol Heart Institute, University of Bristol, Bristol, United Kingdom

18
Forty patients were randomized to off-pump shunt (n = 20) silastic intracoronary shunt (Flothru Biovascular Inc, St Paul, MN) proximal coronary artery occluded by a snare (n = 20) Exclusion criteria included recent ( 1 month) myocardial infarction, reoperative operation, and emergency operation. Cardiac output measurements were carried out using intermittent 10 mL boluses of iced dextrose 5% solution at a temperature of 4°C to 8°C as measured by the inlinein jectate sensor of the thermodilution injectate set. Heart rate, mean systemic arterial pressure, central venous pressure, mean pulmonary arterial pressure, pulmonary capillary wedge pressure (PCWP), cardiac index (CI), stroke volume (SV), systemic vascular resistance index (SVRI),
, cardiac index (CI), stroke volume (SV), systemic vascular resistance index (SVRI),.")
19
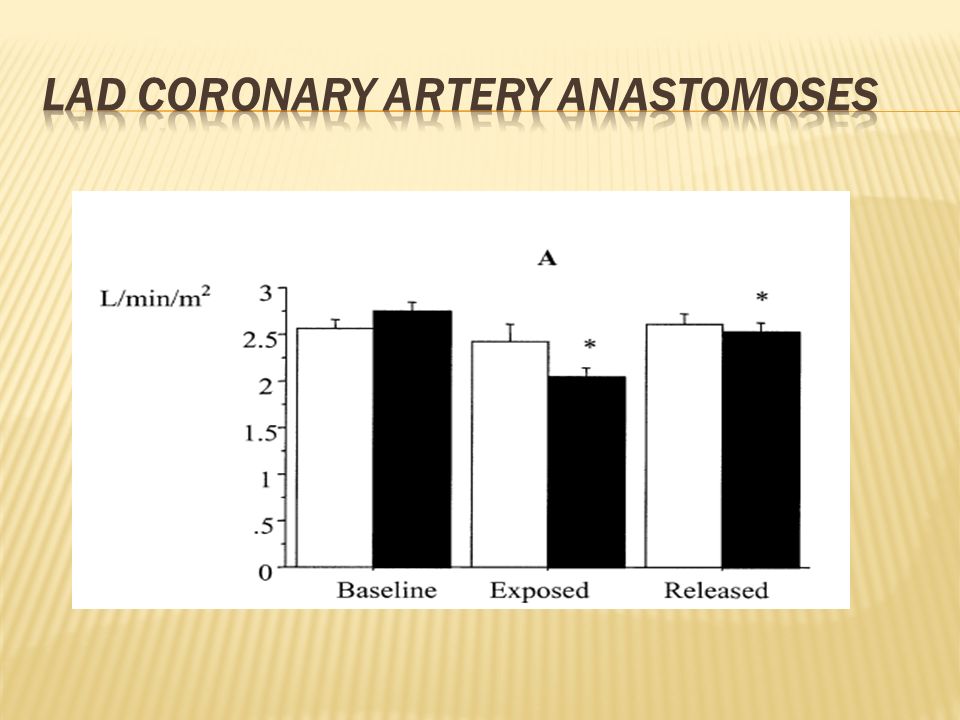
Snaring of the LAD coronary artery resulted in decrease in CI, SV,and mean arterial pressure, as well as increase in PCWP, SVRI, and pulmonary vascular resistance index. These changes were not in the shunted group

21
In both groups there was significant decrease in CI, SV, and mean arterial pressure, and a significant increase in central venous pressure, pulmonary arterial pressure, and PCWP. The snare group demonstrated less rapid recovery as CI and SV were still depressed, and the heart rate and SVRI were still elevated during the recovery position readings, in marked contrast to the shunt group measurements which had already normalized.

23
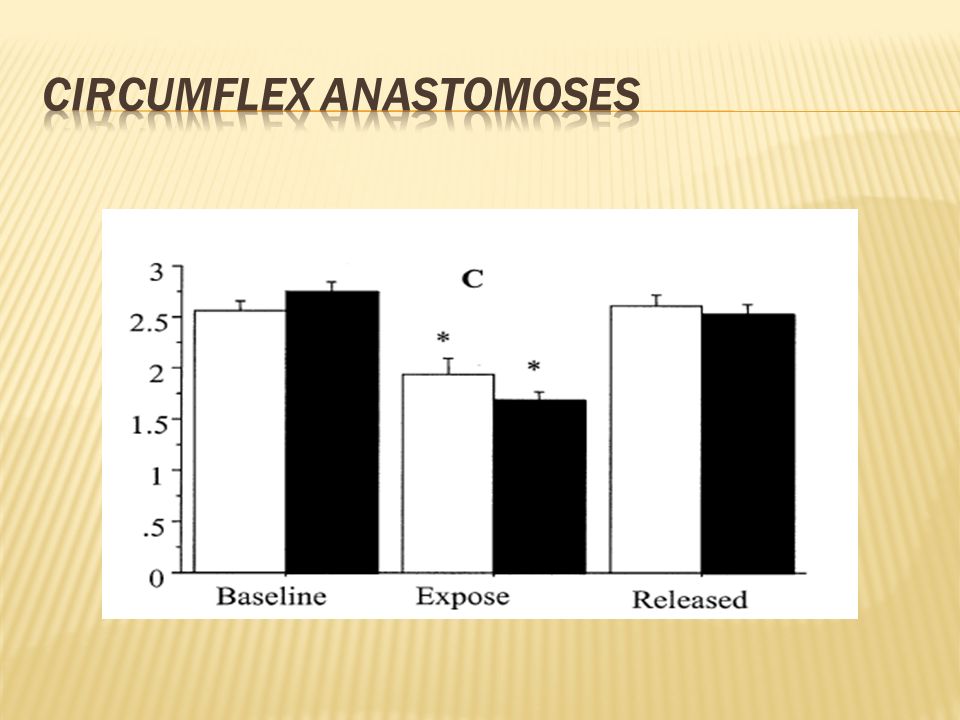
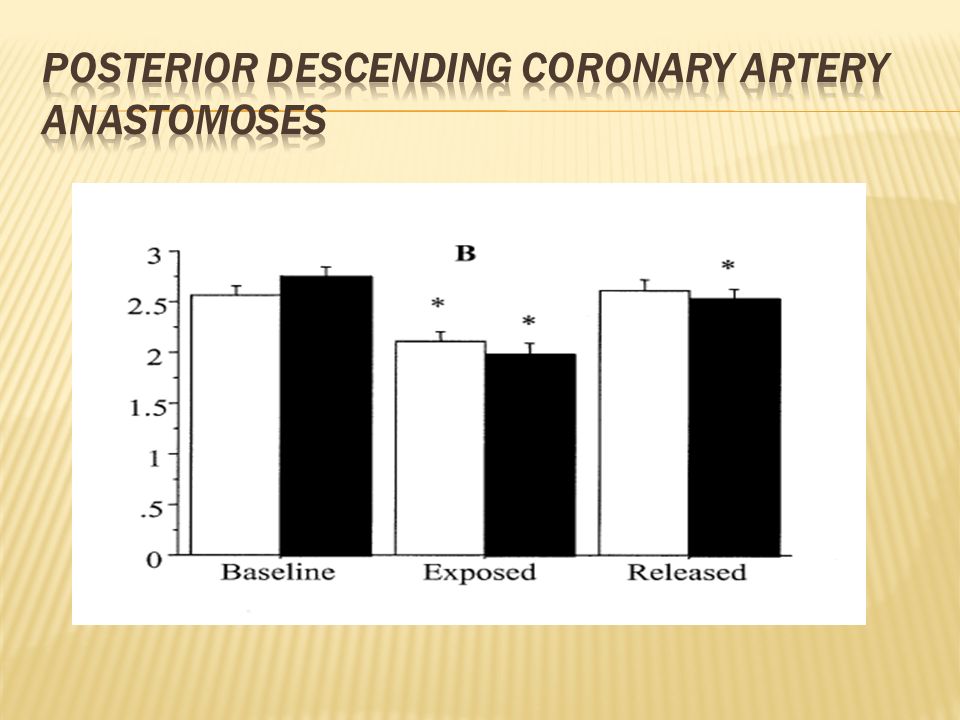
In both groups there was a statistically significant decrease in CI and SV. each of these indices the decrease was greater in the snared group than in the shunted group. significant biventricular dysfunction and relatively delayed recovery in the snared group

25
recovery was complete after 5 minutes of reperfusion in the shunted vessels, but ventricular dysfunction was still evident in the recovery positions in the snared groups.

26
Shunting of coronary arteries is not yet widespread because some do not recognize regional ischemic dysfunction as an important problem. some consider shunts difficult to insert and potentially injurious to endothelial cell

27
this study demonstrates the beneficial effects of using intraluminal coronary shunts in contrast to proximal snaring techniques in preserving intraoperative myocardial function during OPCAB operations in patients with three-vessel coronary artery disease

28
100 OPCABG in two years (between aban 92 & mordad 93) Myocardial revascularization was performed using transsternal sternotomy. No selection of patient. Conversion to on pump if patient not tolerate OPCABG positioning. 5% convert to on pump CABG.

29
Mean EF of patient was 42.3% with total of 308 graft anastomoses. Shunt tube was inserted initially in anastomoses. application of the temporary intraluminal shunt into the target vessel was very easy No macroscopic injuries to target vessels were encountered with shunt tube.

31
In our study all of patient tolerate OPCABG with minimal use of inotrope during & after operation. 99 patient discharge from hospital in mean 5.2 days. one patient with preoperation CRF was died after 3 weeks.

32
Technical devices such as coronary snaring, clamping, and gas insufflation required to obtain optimal operative fields can cause lesions to the endothelium leading to coronary endothelial dysfunction, platelet aggregation, intimal dissection, and plaque rupture.

33
Coronary shunting itself prevents blood from obscuring the operative field, reduces the need for snares, clamping, and gas insufflation, and could possibly ameliorate coronary endothelial injury This shows the capabilities of the shunt tube for preventing ischemia during coronary reconstruction.

Similar presentations





 VAD (Ventricular assist device)>")












 CAD is most common form of heart disease and causes premature death. In UK, 1 in 3 men and.>")



