Download presentation
Presentation is loading. Please wait.

1
Falls and Fracture Risk assessment and management

2
Disclosures: Although various guidelines and studies were reviewed, this represents my own personal bias and conclusions.

3
1) Fractures are bad, worse in the elderly, especially hip fractures. 2) There are multiple factors leading to increased fracture risk, the obvious ones being age and risk of falls. 3) There are industry funded studies that demonstrate significant fracture reduction with medications. 4) There are numerous guidelines out there – BC, National, US (NOF), UK (NOGG), UK (NICE), European, Australian. What do we know?
 There are multiple factors leading to increased fracture risk, the obvious ones being age and risk of falls. 3) There are industry funded studies that demonstrate significant fracture reduction with medications. 4) There are numerous guidelines out there – BC, National, US (NOF), UK (NOGG), UK (NICE), European, Australian. What do we know .")
4
5) There are multiple fracture risk assessment tools- FRAX, QFracture, Garvan, CAROC. 6) There are significant healthcare costs involved- BMD scans, medication costs, hospitalization and physician costs not to mention quality of life issues. 7) The decision to treat lies with the patient and we need to be able to provide objective information to the patient to help guide their decision.
 There are significant healthcare costs involved- BMD scans, medication costs, hospitalization and physician costs not to mention quality of life issues. 7) The decision to treat lies with the patient and we need to be able to provide objective information to the patient to help guide their decision..")
5
BC guidelines http://www2.gov.bc.ca/gov/content/health/practitioner-professional-resources/bc- guidelines/osteoporosishttp://www2.gov.bc.ca/gov/content/health/practitioner-professional-resources/bc- guidelines/osteoporosis http://www2.gov.bc.ca/assets/gov/health/practitioner-pro/bc- guidelines/osteoprosis_summary.pdfhttp://www2.gov.bc.ca/assets/gov/health/practitioner-pro/bc- guidelines/osteoprosis_summary.pdf Osteoporosis Canada http://www.osteoporosis.ca/multimedia/pdf/Quick_Reference_Guide_October_2010.pdf NOF http://nof.org/files/nof/public/content/file/2791/upload/919.pdf NOGG https://www.shef.ac.uk/NOGG/NOGG_Pocket_Guide_for_Healthcare_Professionals.pdf NICE https://www.nice.org.uk/guidance/TA160/chapter/1-Guidance European http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3587294/ Australian http://www.racgp.org.au/download/documents/Guidelines/Musculoskeletal/op_algorithm.pdf http://www.racgp.org.au/afp/2012/march/osteoporosis-pharmacological-prevention-and- management/http://www.racgp.org.au/afp/2012/march/osteoporosis-pharmacological-prevention-and- management/

6
So where do we start?

7
Basic principles

8
Fracture Risk Assessment The most studied and validated tool is the WHO FRAX tool. There is a specific Canadian cohort for the FRAX. It has its limitations, but is simpler to use than the others (fewer inputs). Despite it being a WHO tool, the formula is proprietary through the University of Sheffield and although use of the online calculator is free, to be able to use the tool on your desktop you have to pay a license fee. The tool can be used with and without a BMD value. https://www.shef.ac.uk/FRAX/
. Despite it being a WHO tool, the formula is proprietary through the University of Sheffield and although use of the online calculator is free, to be able to use the tool on your desktop you have to pay a license fee. The tool can be used with and without a BMD value.")
9
Falls Risk Assessment There are many comprehensive tools out there, most require some basic equipment and a stopwatch and look to take 15-30 min to complete. However, there is one tool: Fracture Risk Assessment Tool-FRAT, that has been produced specifically for the use in a GP office and will take less than one minute. http://www.bhps.org.uk/falls/documents/FRATtool.pdf

10
Fracture risk reduction Probably the basic interventions are the most important interventions: 1) Encourage maintaining an active lifestyle and include activities to improve leg strength and balance: 30-60min of walking per day. 2) Encourage proper technique when lifting: keep your back straight rather than bent. Also, consider whether the object to be lifted can be divided into smaller portions before lifting. 3) Ensure adequate daily intake of both calcium (generally about 1000- 1200 total mg/day) and vitamin D (about 1000 IU/day).
 Encourage proper technique when lifting: keep your back straight rather than bent. Also, consider whether the object to be lifted can be divided into smaller portions before lifting. 3) Ensure adequate daily intake of both calcium (generally about total mg/day) and vitamin D (about 1000 IU/day)..")
11
. 4) Reduce risk for falls: Having a fall is the single greatest risk for breaking a bone. a) Review medications regularly Polypharmacy (greater than 3 medications) is independent risk factor Common culprits OR Percentage increase Antidepressants 1.68 68% Antipsychotics 1.59 59% Benzodiazepines 1.57 57% Sedatives 1.47 47% Antihypertensive 1.24 24% NSAID 1.21 21% Diuretics 1.07 7% B-Blockers 1.01 1% Narcotics 0.96 - (CI 0.78-1.18) Woolcott J., Richardson K., Wiens M., Patel B., Marin J., Khan K., et al.. (2009) Meta-analysis of the impact of 9 medication classes on falls in elderly persons. Arch Intern Med 169: 1952–1960 b) Encourage regular vision checks. c) Consider home assessment for the high risk patient by the FHA Mobile Falls Prevention team. http://www.cdc.gov/HomeandRecreationalSafety/Falls/WhatYouCanDoToPreventFalls.html http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4125318/#bibr55-2042098613486829
 Review medications regularly Polypharmacy (greater than 3 medications) is independent risk factor Common culprits OR Percentage increase Antidepressants % Antipsychotics % Benzodiazepines % Sedatives % Antihypertensive % NSAID % Diuretics % B-Blockers % Narcotics (CI ) Woolcott J., Richardson K., Wiens M., Patel B., Marin J., Khan K., et al.. (2009) Meta-analysis of the impact of 9 medication classes on falls in elderly persons. Arch Intern Med 169: 1952–1960 b) Encourage regular vision checks. c) Consider home assessment for the high risk patient by the FHA Mobile Falls Prevention team.")
12
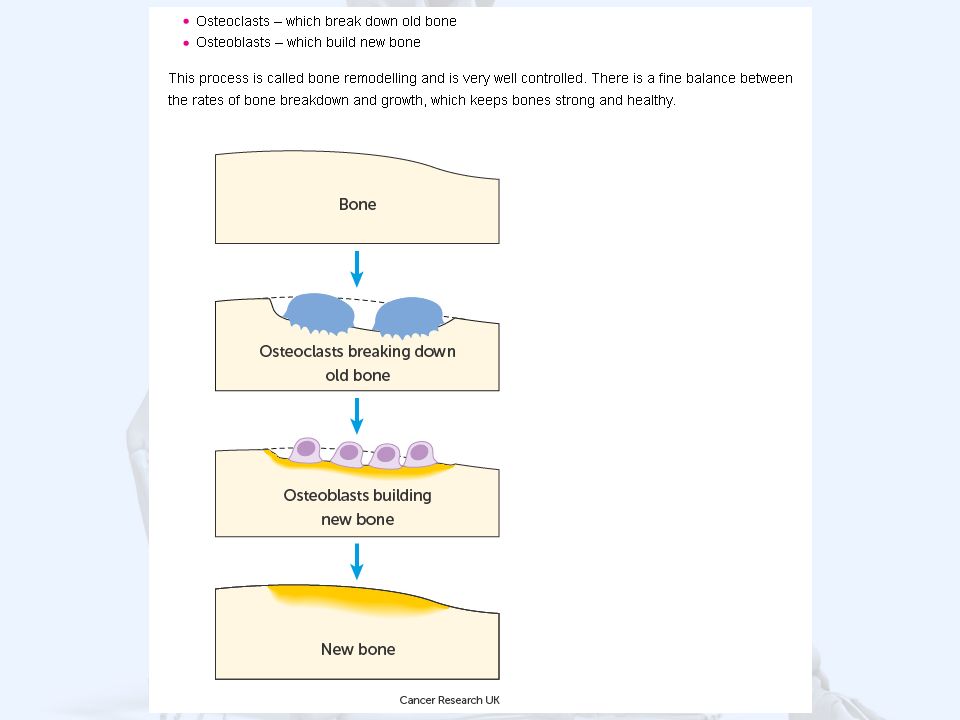
5) Medications to strengthen bones: Commonest used in general practice are the bisphosphonate group. Bisphosphonates target the areas of higher bone turnover. The osteoclast cells absorb the bisphosphonate drug, which slows down their activity and reduces bone break down. There are several different types of bisphosphonates, and they each work slightly differently.types of bisphosphonates We know that they can Interfere with the formation of osteoclasts Make osteoclasts self destruct, or die early Change the signalling between osteoclasts and osteoblasts Form a barrier between the bone and the osteoclast

14
Tolerability of bisphosphonates: GIT adverse effects Results: A total of 11% of the alendronate patients and 13% of the placebo patients reported an upper GI tract adverse event. Discontinuations due to drug- related upper GI tract adverse events occurred in 3% of alendronate patients and 1% of placebo patients. Results: Of 438 patients who were randomized, 367 completed the study. The proportions of patients who experienced an upper GI AE during the study period were 66 (22.7%) and 30 (20.4%) for alendronate vs placebo. Renal impairment Both oral and intravenous bisphosphonates are not recommended when eGFR is < 30 (<35 for IV).
 and 30 (20.4%) for alendronate vs placebo. Renal impairment Both oral and intravenous bisphosphonates are not recommended when eGFR is < 30 (<35 for IV)..")
15
Some of the rare serious side effects: Osteonecrosis of the jaw It has been estimated that the risk of ONJ is approximately 1 in 10,000 to 1 in 100,000 patient-years in patients taking oral bisphosphonates for osteoporosis. Atypical Femur Fractures Although long-term use (median treatment seven years) of bisphosphonates increases the RR of atypical fractures, the absolute risk is low (3.2 to 50 cases per 100,000 person-years). The risk may rise with duration of bisphosphonate exposure (100 per 100,000 person-years). When bisphosphonates are stopped, the risk of atypical fracture declines.
 of bisphosphonates increases the RR of atypical fractures, the absolute risk is low (3.2 to 50 cases per 100,000 person-years). The risk may rise with duration of bisphosphonate exposure (100 per 100,000 person-years). When bisphosphonates are stopped, the risk of atypical fracture declines..")
16
There are many industry sponsored trials. I have reviewed the FIT,VERT-NA and HORIZON trials as these appear to be the original trials of note for bisphosphonates:

17
“A single, annual intravenous (IV) infusion of zoledronic acid can decrease the risk of vertebral fracture by 70% and the risk of hip fracture by 41% among women with osteoporosis, according to the 3-year results of the Health Outcomes and Reduced Incidence with Zoledronic Acid Once Yearly (HORIZON) Pivotal Fracture Trial. The results were published in the New England Journal of Medicine (NEJM).”
. .")
18
HORIZON Trial (Aclasta/Zoledronic acid) 7765 women 65-89yrs (mean 73yrs) over 3 yrs Tscore < -2.5 or Tscore <-1.5 and vertebral fracture Morphometric vertebral #: 3.3% cf 10.9% RRR 70% ARR 7.6% Hip fracture: 1.4% cf 2.5% RRR 41% ARR 1.1%
 7765 women 65-89yrs (mean 73yrs) over 3 yrs Tscore < -2.5 or Tscore <-1.5 and vertebral fracture Morphometric vertebral #: 3.3% cf 10.9% RRR 70% ARR 7.6% Hip fracture: 1.4% cf 2.5% RRR 41% ARR 1.1%")
19
3658 Women aged 55-80yrs Average age 70yrs Alendronate 5mg daily increased to 10mg daily plus 500mg Ca and 250iu Vit D Femoral neck T-score <-2.5 or previous vertebral fracture 3-4 yrs of treatment, effect noted within 12 months Fracture reduction: RRR ARR Hip 53% 1.2% Vertebral (radiological) 48% 7.2% Vertebral (clinical) 45% 2.3% All fractures 30% 5.5% http://press.endocrine.org/doi/full/10.1210/jcem.85.11.6953 FIT trial Sponsor—Merck Research Laboratories
 48% 7.2% Vertebral (clinical) 45% 2.3% All fractures 30% 5.5% FIT trial Sponsor—Merck Research Laboratories")
20
Started with 2458 women <85yrs All had vertebral fracture seen on screening Xray Average age 70yrs Ended up with 949 women, 3 years of treatment Residronate 5mg daily plus Ca 1000mg and up to 500iu Vit D if indicated http://jama.jamanetwork.com/article.aspx?articleid=191987 VERT-NA Residronate - Procter & Gamble Fracture reduction: RRR ARR Vertebral(radiological) 41% 4% Non vertebral 39% 3.2%
 41% 4% Non vertebral 39% 3.2%")
21
Summary based on these trials: For females around age of 70yrs with either a prior vertebral fracture or a BMD < -2.5 (ie evidence of osteoporosis), taking a bisphosphonate will reduce the: ABSOLUTE risk of Hip fractures by about 1% Vertebral (clinical) fractures by about 2% All fractures (include radiological) by about 5%. Most guidelines focus on the RRR (53%/45%/30%) and then apply these numbers to the risk calculated by the FRAX tool (10yr predication) which leads to some interesting results.
 and then apply these numbers to the risk calculated by the FRAX tool (10yr predication) which leads to some interesting results..")
22
Cochrane review of fracture risk prevention with bisphosphonates: Note that their definition of “secondary prevention” includes patient with low bone mass. http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD001155.pub2/abstract;jsessio nid=984707094936288431A1897617796A0B.f01t02

23
Goals of this Fracture Risk Assessment Tool 1) To facilitate appropriate screening of patients for increased fall and fracture risk. 2) Use these results to remind us to address the various physical and polypharmacy issues. 3) Provide meaningful information to present to the patient to aid in their decision making if they are considering bone building medications.
 Use these results to remind us to address the various physical and polypharmacy issues. 3) Provide meaningful information to present to the patient to aid in their decision making if they are considering bone building medications..")
24
Lets look at some numbers from our clinic……..

25
Number of patients in clinic over the age of 50 yrs: 2472 (>65yrs 1267) Number of patients in clinic on bisphosphonates: 31 1.4 million Canadians suffer from osteoporosis One in four women over the age of 50 has osteoporosis One in eight men over the age of 50 has osteoporosis 70 per cent of hip fractures are related to osteoporosis Up to 20 per cent of hip fractures result in death Up to 50 per cent of hip fractures result in permanent disability More women die each year as a result of osteoporotic fractures than from breast and ovarian cancer combined
 Number of patients in clinic on bisphosphonates: million Canadians suffer from osteoporosis One in four women over the age of 50 has osteoporosis One in eight men over the age of 50 has osteoporosis 70 per cent of hip fractures are related to osteoporosis Up to 20 per cent of hip fractures result in death Up to 50 per cent of hip fractures result in permanent disability More women die each year as a result of osteoporotic fractures than from breast and ovarian cancer combined")
26
Results for females screened in last month with the new tool Hip Fracture RiskTotal Fracture RiskAge 18%38%89 63%65%85 9.10%24%85 13%35%83 8.00%22%83 11%32%82 16%35%82 6.70%19%81 5.20%16%80 6.00%18%80 29%41%79 5.70%17%79 4.50%14%78 4.90%15%77 6.80%17%77 3.80%13%76 3.80%12%73 3.50%16%72 3.10%11%70 0.30%9%67 Averages 11%29%78.9

27
Results for males screened in last month Hip Fracture RiskTotal Fracture RiskAge 6.40%11%95 4.10%8.90%88 5.00%10%88 3.30%7.80%83 19%26%82 4.90%13%81 3.30%8.10%79 1.70%5.40%76 4.20%7.50%75 3.80%17%66 Averages 6%11%81.3

28
?

29
Lets apply some guidelines….

30
BC Guidelines

31
NOF (USA) Guidelines Pharmacologic treatment recommendations: Initiate pharmacologic treatment in those with hip or vertebral (clinical or asymptomatic) fractures. Initiate therapy in those with T-scores < -2.5 at the femoral neck, total hip or lumbar spine by dual-energy x-ray absorptiometry (DXA). Initiate treatment in postmenopausal women and men age 50 and older with low bone mass (T-score between -1.0 and -2.5, osteopenia) at the femoral neck, total hip or lumbar spine by DXA and a 10-year hip fracture probability > 3 percent or a 10-year major osteoporosis- related fracture probability > 20 percent based on the U.S.-adapted WHO absolute fracture risk model (FRAX®; www.NOF.org and www.shef.ac.uk/FRAX).
. Initiate treatment in postmenopausal women and men age 50 and older with low bone mass (T-score between -1.0 and -2.5, osteopenia) at the femoral neck, total hip or lumbar spine by DXA and a 10-year hip fracture probability > 3 percent or a 10-year major osteoporosis- related fracture probability > 20 percent based on the U.S.-adapted WHO absolute fracture risk model (FRAX®; and")
32
NICE (UK) Guidelines Alendronate is recommended as a treatment option for the primary prevention of osteoporotic fragility fractures in the following groups: Women aged 70 years or older who have an independent clinical risk factor for fracture or an indicator of low BMD and who are confirmed to have osteoporosis (that is, a T-score of −2.5 SD or below). Women aged 65–69 years who have an independent clinical risk factor for fracture and who are confirmed to have osteoporosis (that is, a T-score of −2.5 SD or below). Postmenopausal women younger than 65 years who have an independent clinical risk factor for fracture and at least one additional indicator of low BMD and who are confirmed to have osteoporosis (that is, a T-score of −2.5 SD or below).
. Postmenopausal women younger than 65 years who have an independent clinical risk factor for fracture and at least one additional indicator of low BMD and who are confirmed to have osteoporosis (that is, a T-score of −2.5 SD or below)..")
33
NOGG Executive NOGG Executive http://www.shef.ac.uk/NOGG/NOGG_Executive_Summary.pdf Men and women with probabilities below the lower assessment threshold can be reassured. Men and women with probabilities above the upper assessment threshold can be considered for treatment. Men and women with probabilities between the upper and lower assessment threshold should be referred for bone mineral density measurements and their fracture probability reassessed.

34
Guideline outcomes Total = 20 Females GuidelineBMDNothingRx w/o BMD ?Final Rx? ????? BC 111810 NOF (US) 1910 NICE (UK) 15504 NOGG (UK) 14337 Modified NOGG 71305
 1910 NICE (UK) NOGG (UK) Modified NOGG")
35
Modified NOGG 85 23 42 35 90 28 49 40 Below intervention threshold reassure Equal or above intervention threshold do BMD first and consider treatment if remains equal or above the intervention threshold and femoral neck Tscore < -1.75. 7 8.5 10.5 12.5 16 20 24 29 34

36
All Wales Medicine Strategy Group Evidence shows that the patients most likely to benefit from treatment with bisphosphonates are women who have already been diagnosed with low BMD or have already had a vertebral fracture. The number of patients that are needed to treat (NNT)in order to avoid a vertebral or hip fracture is given in Table 1. Table 1. NNTs for alendronate plus calcium/vitamin D – taken from NHS Highland’s Guidance for prescribing in frail adults. Age 2-year vertebral # (NNT) 2-year hip # (NNT) 70–74 years 65 430 75–79 years 45 180 80–84 years 60 105 85–89 years 55 45 ≥ 90 years 40 40 F or example if 65 patients aged between 70 and 74 years take alendronate plus calcium/vitamin D for 2 years, 1 vertebral fracture will be avoided.
in order to avoid a vertebral or hip fracture is given in Table 1. Table 1. NNTs for alendronate plus calcium/vitamin D – taken from NHS Highland’s Guidance for prescribing in frail adults. Age 2-year vertebral # (NNT) 2-year hip # (NNT) 70–74 years –79 years –84 years –89 years ≥ 90 years F or example if 65 patients aged between 70 and 74 years take alendronate plus calcium/vitamin D for 2 years, 1 vertebral fracture will be avoided..")
39
1) Screen females > 65 yrs and males >75 yrs with ‘FRAX without BMD’ Repeat screening every 5yrs to age 75 then every 3 yrs to age 85 then every 2 yrs thereafter. 2) Modified NOGG thresholds used to decide on need for BMD and based on the BMD results (both the calculated total fracture risk as well as the femoral neck Tscore), the need for medication. 3) Threshold of 2o% is used to recommend a falls prevention program to all ages. Logic incorporated in the tool:
 Modified NOGG thresholds used to decide on need for BMD and based on the BMD results (both the calculated total fracture risk as well as the femoral neck Tscore), the need for medication. 3) Threshold of 2o% is used to recommend a falls prevention program to all ages. Logic incorporated in the tool:.")
40
Final Conclusions Fractures are a significant medical problem particularly in the aging population. There are multiple risk factors for increasing fracture risk, especially important are falls and lifestyle (exercise, smoking, alcohol, caffeine). Bone building medications have a place but the data is incomplete so decisions need to be made on ‘Expert opinion’ and simple common sense.
. Bone building medications have a place but the data is incomplete so decisions need to be made on ‘Expert opinion’ and simple common sense..")
41
GPSC Fee code 14066 14066 Personal Health Risk Assessment Eligible population – must have one of four risks: Smoking Dx 786 Obesity (BMI >30 ) Dx 783 Unhealthy Eating Dx 783 Inadequate Exercise Dx 785 INTENT: Risk assessment & planning visit both for identified risks & to review relevant recommended prevention services based on age, sex and gender (eg. Pap, mammogram, stool OB, immunizations, etc.)
.")
42
The End

Similar presentations



, confirmed after.>")
, Fellowship Diabetes/Endocrinology (AKUH), PG Dip Diab (UK) Consultant Endocrinologist.>")



>")






>")




