Download presentation
Presentation is loading. Please wait.

1
Family Medicine Clerkship

2
The Jeopardy board lists dollar values under each heading. The dollar amount on the screen is hyperlinked to the answer. Click on a dollar amount and you will go to a slide with the answer. Click on the answer slide and you will be taken to the correct question for the answer. Click on the illustration in the question slide and you will go back to the Jeopardy board. To get to Double Jeopardy click on the box on the lower half of the slide. To get to Final Jeopardy click anywhere on the Jeopardy board other than a dollar amount. Double jeopardy (2) includes a mini-lecture. The last slide of the mini- lecture takes you back to the jeopardy board. HAVE FUN!!
 includes a mini-lecture. The last slide of the mini- lecture takes you back to the jeopardy board. HAVE FUN!!.")
3
Basic science of evidence Value and Equity Long-term and Less side effects Systems and principles Quality and Safety $1000 $400 $200 $300 $400 $500 $200 $400 $600 $800 $100 $200 $300 $400 $500 $200 $400 $600 $800 $1000 $100 $600 $500 $400 $200 $400 $200 $1000 $300 $800 $100 $200 $500 $300 $100 $200 $400 $600 $800 $1000 $100 $200 $300 $400 $500 $200 $400 $600 $800 $1000

4
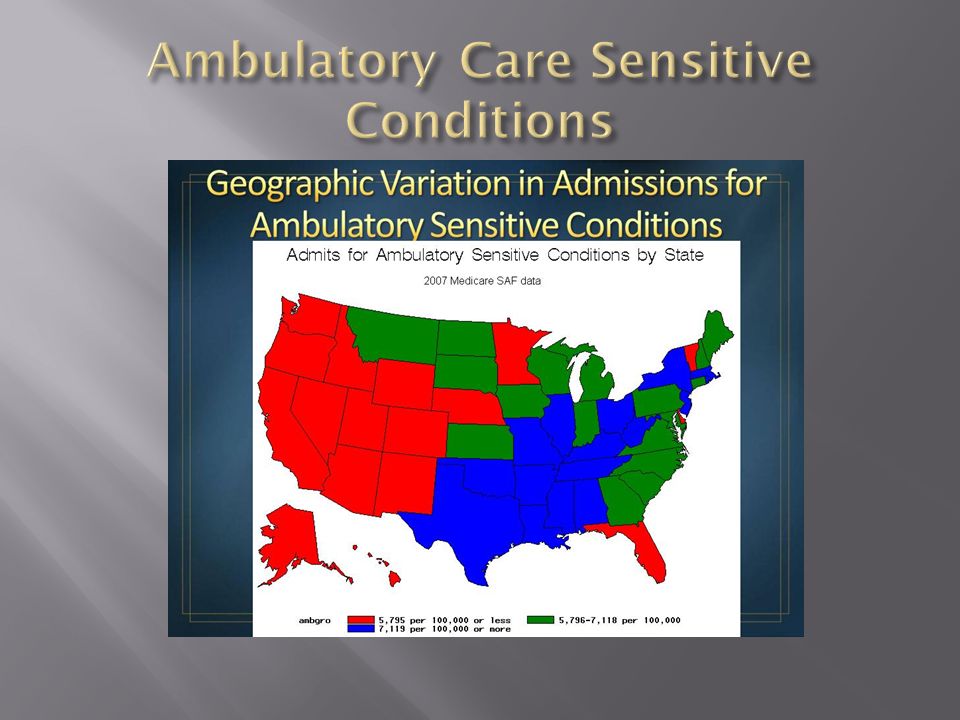
Topic: Geographic variation of care

5
This reporting initiative was launched in 2001 and is now in its fifth version. The Survey assesses hospital performance based on four quality and safety leaps that are proven to reduce preventable medical mistakes and are endorsed by the National Quality Forum National Quality Forum. The Survey is updated annually to reflect changes in reporting standards and the latest evidence base.

7
These are medical problems that are potentially preventable. For example, hypertension (high blood pressure) is a condition that can be treated outside of a hospital. With proper medication and management of care, most people should not need to be hospitalized for hypertension.
 is a condition that can be treated outside of a hospital. With proper medication and management of care, most people should not need to be hospitalized for hypertension..")
9
This is a term to describe a process designed to help patients understand the nature of the disease or condition being addressed; understand the clinical service being provided including benefits, risks, limitations, alternatives and uncertainties; consider their own preferences and values; participate in decision-making at the level they desire; and make decisions consistent with their own preferences and values or choose to defer a decision until a later time.

11
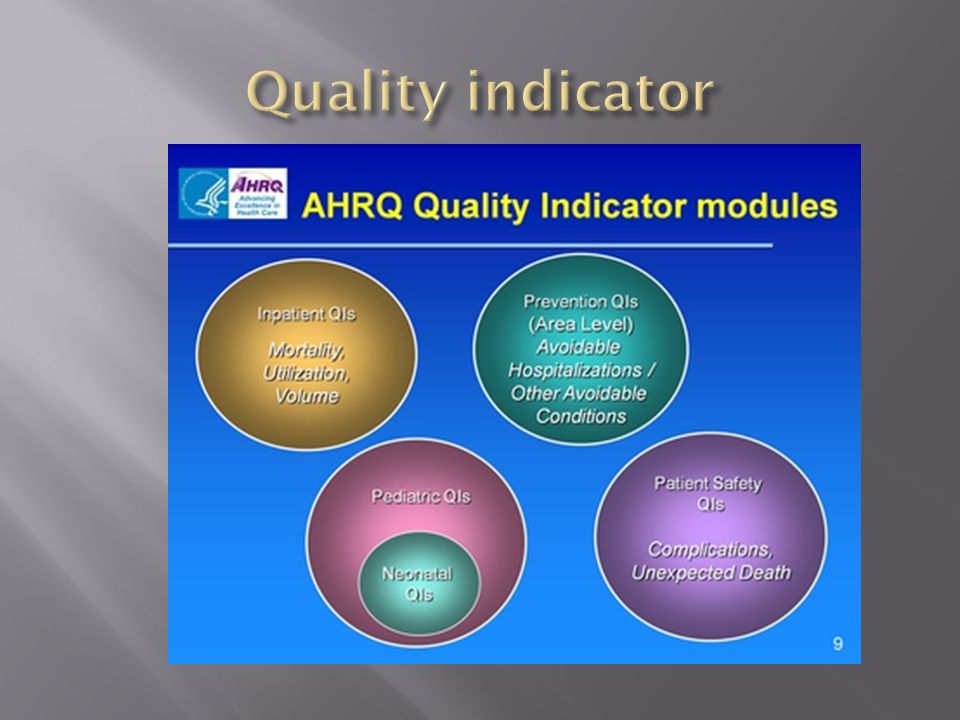
This is an agreed-upon process or outcome measure that is used to determine the level of quality achieved. A measurable variable (or characteristic) that can be used to determine the degree of adherence to a standard or achievement of quality goals.
 that can be used to determine the degree of adherence to a standard or achievement of quality goals..")
13
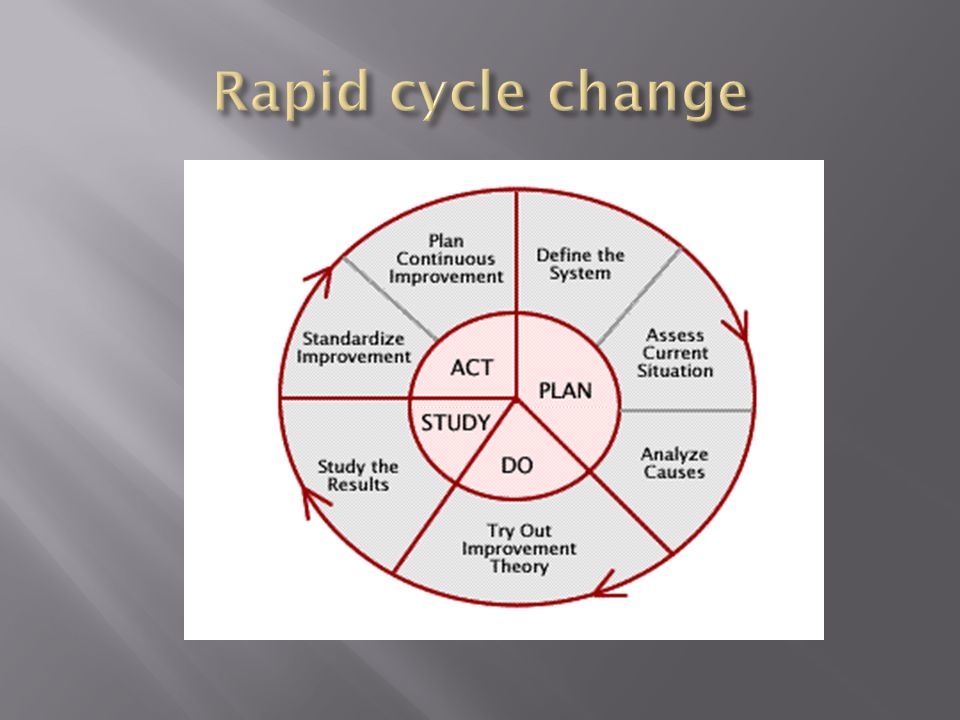
This is a quality-improvement method that identifies, implements and measures changes made to improve a process or a system. After a baseline is established, improvement occurs through small, rapid PDSA (Plan, Do, Study, Act) cycles to advance practice change.
 cycles to advance practice change..")
15
This is any unexpected event in a health care setting that causes death or serious injury to a patient and is not related to the natural course of the patient's illness.

17
This book, published by the Institute of Medicine in 2003 reported that a huge divide exists between the care we should receive and the care that we get. It introduced the notion that health care needs to take a page from industry and use its engineering improvement methods to aim for top quality, efficiency and safety. The report laid out six goals that would become akin to a mantra for the quality improvement movement: care should be "safe, effective, patient-centered, timely, efficient and equitable”

19
This is the term for medical mistakes that should never occur under any circumstance.

21
Initiated by the ABIM, this is a list compiled by nine medical specialty organizations, along with Consumer Reports, of tests or procedures commonly used, whose necessity should be questioned and discussed by patients with their physicians.

23
This term refers to the most up-to-date patient care interventions, which result in the best patient outcomes and minimize patient risk of death or complications.

25
This comprises mechanisms that ensure patients and clinicians have access to, and take into consideration, all required information on a patient's conditions and treatments to ensure that the patient receives appropriate health care services.

27
This model of care considers patients' cultural traditions, personal preferences and values, family situations and lifestyles. Responsibility for important aspects of self-care and monitoring is put in patients' hands—along with the tools and support they need. If care is delivered in this manner, unneeded and unwanted services can be reduced.

30
This is health care model that aims to provide structured, proactive and coordinated care for patients rather than episodic treatments for illnesses. In this model, the primary-care doctor operates as a “home base” for patients, overseeing all aspects of patients’ health and coordinates care with any specialists involved in the patient’s care.

32
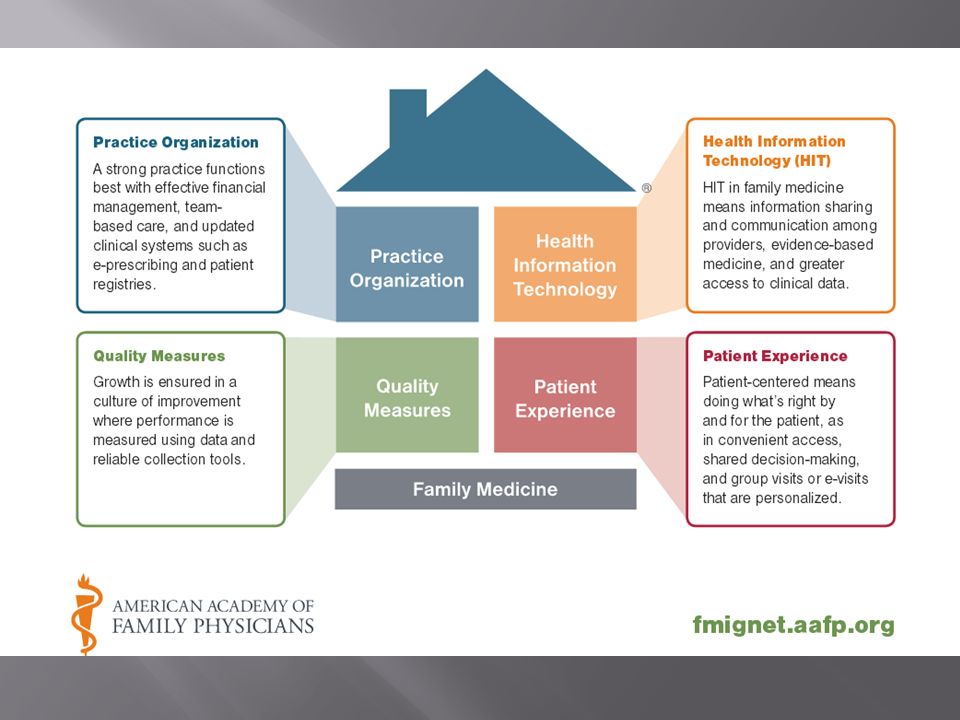
Guided by the “Joint Principles Access to a personal physician who leads the care team within a medical practice A whole-person orientation to providing patient care Integrated and coordinated care Focus on quality and safety

33
Practice organization Standardizing practices and improving practice efficiency Health information technology Use of asynchronous communication Leveraging technology to improve quality and safety Quality of care Improvement based on data Patient-centered care Access, satisfaction, self-management

35
Rules established when the federal government chose to pay for EHR technology in physicians offices to assure the technology was being used for e-prescribing, electronic exchange of health information to improve quality of health care and to submit clinical quality and other measures to payers.

37
This person is responsible for managing high risk chronic illness patients to promote effective education, self-management support, and timely healthcare delivery to achieve optimal quality and financial outcomes.

39
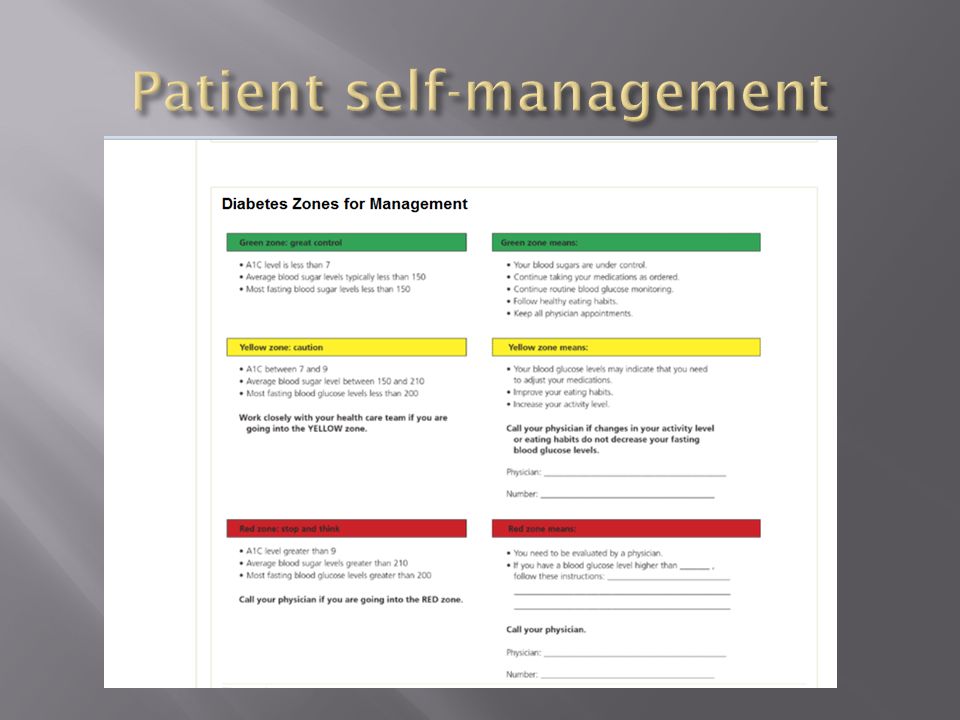
Individuals ability to manage the symptoms, treatment, physical and social consequences and lifestyle changes inherent in living with a chronic condition

41
A method of providing care that utilizes multiple staff members with different skill sets each working to the peak of his or her license to provide care to a group of patients. Typically led by a physician.

43
Systematically developed statements to assist practitioners and patient decisions about appropriate health care for specific circumstances. They are designed to support, not dictate, the decision-making processes in patient care.

45
Categorized as the lowest form of medical evidence, superseded even by methodologically flawed clinical research. It may represent an alternative form of medical knowledge, one that may be complementary to empirical evidence. It is best used to overcome the intrinsic gap between clinical research and the care of individual patients.

47
Care provided by physicians specifically trained for and skilled in comprehensive first contact and continuing care for persons with any undiagnosed sign, symptom, or health concern (the "undifferentiated" patient) not limited by problem origin (biological, behavioral, or social), organ system, or diagnosis. This care includes health promotion, disease prevention, health maintenance, counseling, patient education, diagnosis and treatment of acute and chronic illnesses in a variety of health care settings

49
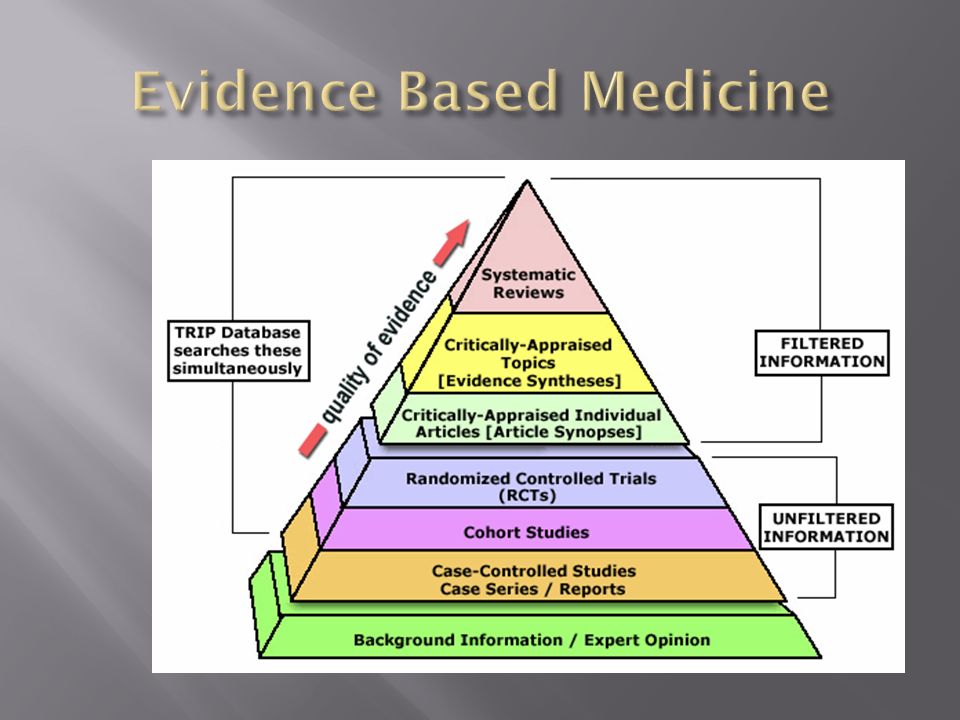
This is the conscientious, explicit, and judicious use of current best evidence in making decisions about the care of individual patients.

51
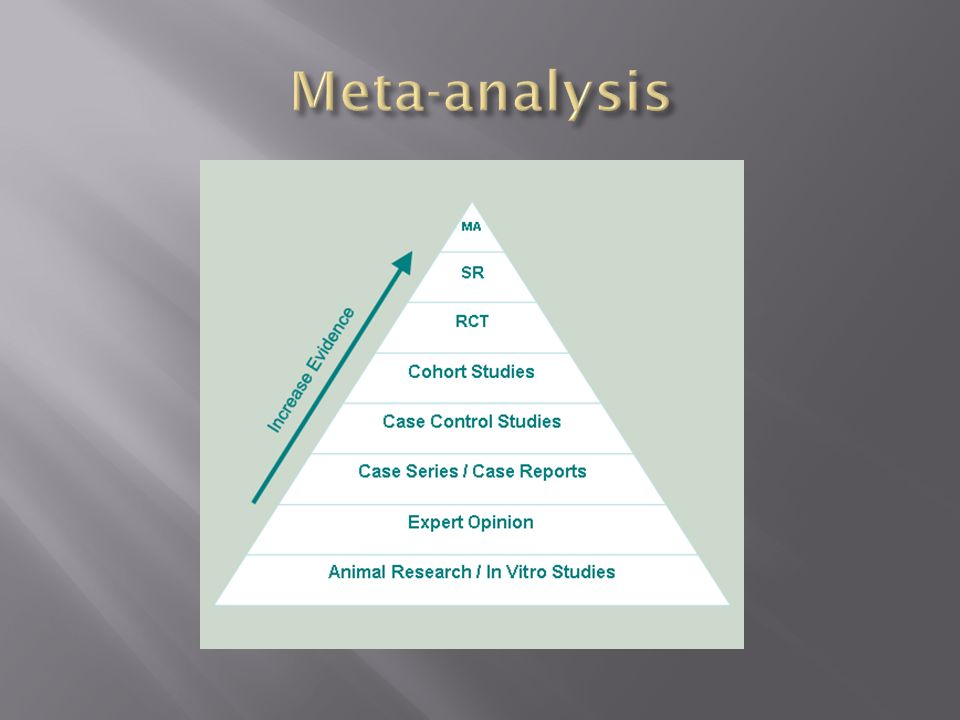
This is a statistical technique for combining the findings from independent studies. It is most often used to assess the clinical effectiveness of healthcare interventions by combining data from two or more randomized control trials and giving due weight to the size of the different studies included. The best of these aim for complete coverage of all relevant studies, look for the presence of heterogeneity, and explore the robustness of the main findings using sensitivity analysis.

53
These are quantitative, comparative, controlled experiments in which a group of investigators studies two or more interventions by administering them to groups of individuals who have been randomly assigned to receive each intervention.

55
Includes many key classes of pharmacotherapy, excluding the so-called specialty or biologic drugs. Although some physicians have complaints, the scientific literature indicates no inferiority of clinical efficacy of the products on this list. Physicians will increasingly use this list, and patients will have to expect that most of their medications will come from this list.

57
Beginning in January 2014, individuals under 65 years of age with income below 133 percent of the federal poverty level (FPL) will be eligible for this program should states opt in. For the first time, low-income adults without children will be guaranteed coverage through this program in every state without need for a waiver, and parents of children will be eligible at a uniform income level across all states.

59
These are groups of doctors, hospitals, and other health care providers, who come together voluntarily to give coordinated high quality care to their patients and are paid differently by Medicare for providing care in this way. The goal of coordinating care in this way is to ensure that patients, especially the chronically ill, get the right care at the right time, while avoiding unnecessary duplication of services and preventing medical errors.

61
These are community-based organizations that provide comprehensive primary care and preventive care, including health, oral, and mental health/substance abuse services to persons of all ages, regardless of their ability to pay or health insurance status. Thus, they are a critical component of the health care safety net. Related terms include Community/Migrant Health Centers (C/MHC), Community Health Centers (CHC), and 330 Funded Clinics.
, Community Health Centers (CHC), and 330 Funded Clinics..")
63
These are intended to increase primary care services for Medicaid and Medicare patients in rural communities. They can be public, private or non-profit. Payments include enhanced reimbursement rates for providing Medicaid and Medicare services in rural areas. They must be located in rural, under-served areas and must use one or more physician assistants or nurse practitioners.

65
In 1989 - 1991, a measles epidemic in the United States resulted in tens of thousands of cases of measles and hundreds of deaths. Upon investigation, CDC found that more than half of the children who had measles had not been immunized, even though many of them had seen a health care provider. This program was started in response and families of children who may not otherwise have access to vaccines by providing free vaccines to doctors who serve them.

67
This is a program administered by the United States Department of Health and Human Services that provides matching funds to states for health insurance to families with children. The program was designed to cover uninsured children in families with incomes that are modest but too high to qualify for Medicaid. At its creation in 1997, it was the largest expansion of taxpayer-funded health insurance coverage for children in the U.S. since Medicaid began in the 1960s.

69
This is a national social insurance program, administered by the U.S. federal government in 1965, that guarantees access to health insurance for Americans ages 65 and older and younger people with disabilities as well as people with end stage renal disease. As a social insurance program, it spreads the financial risk associated with illness across society to protect everyone, and thus has a somewhat different social role from private insurers, which must manage their risk portfolio to guarantee their own solvency.

71
This is a set of state-regulated and standardized health care plans in the United States, from which individuals may purchase health insurance eligible for federal subsidies. All exchanges must be fully certified and operational by January 1, 2014 under federal law.

73
These hospitals are distinguished by their commitment to provide access to care for people with limited or no access to health care due to their financial circumstances, insurance status, or health condition. These hospitals maintain an “open door,” offering patients access to services regardless of their ability to pay; and a substantial share of their patient mix is uninsured, Medicaid, and other vulnerable patients

75
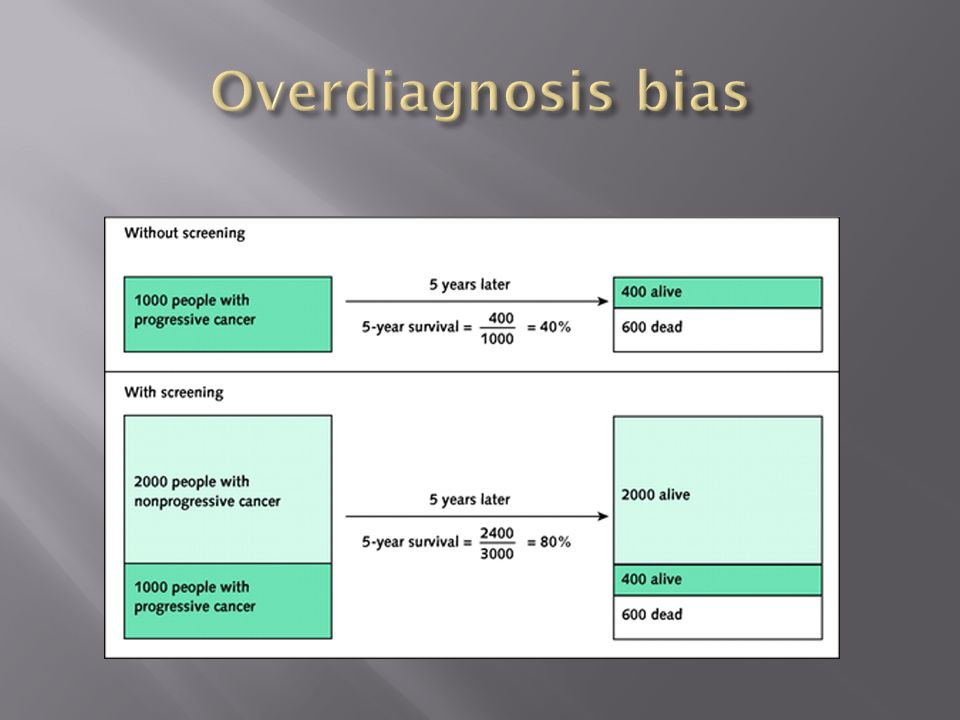
Detection of disease that would remain subclinical prior to death otherwise, thus improving apparent survival

77
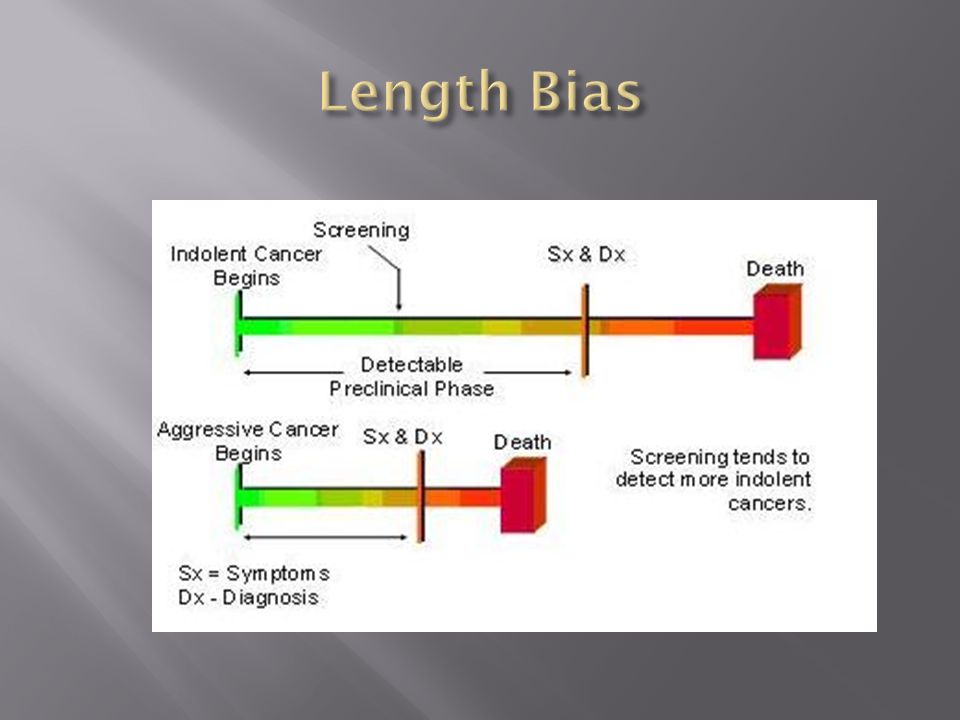
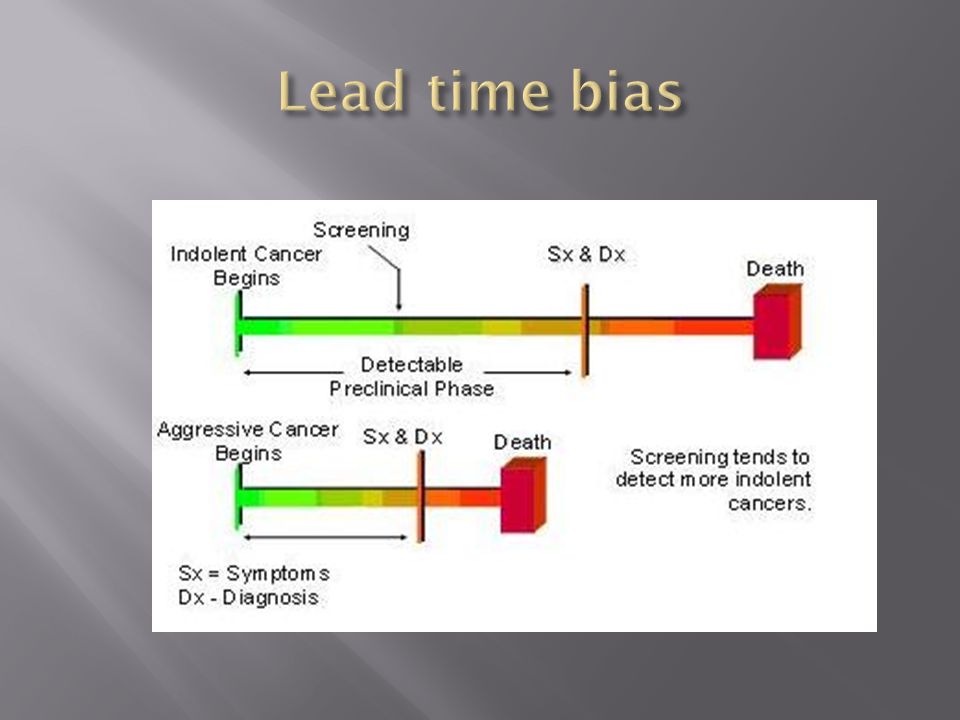
Screening tends to detect more indolent illness thus improving apparent efficacy of treatment

79
This is the number of people in a group who die annually from a disease, divided by the total number of people in the group.

82
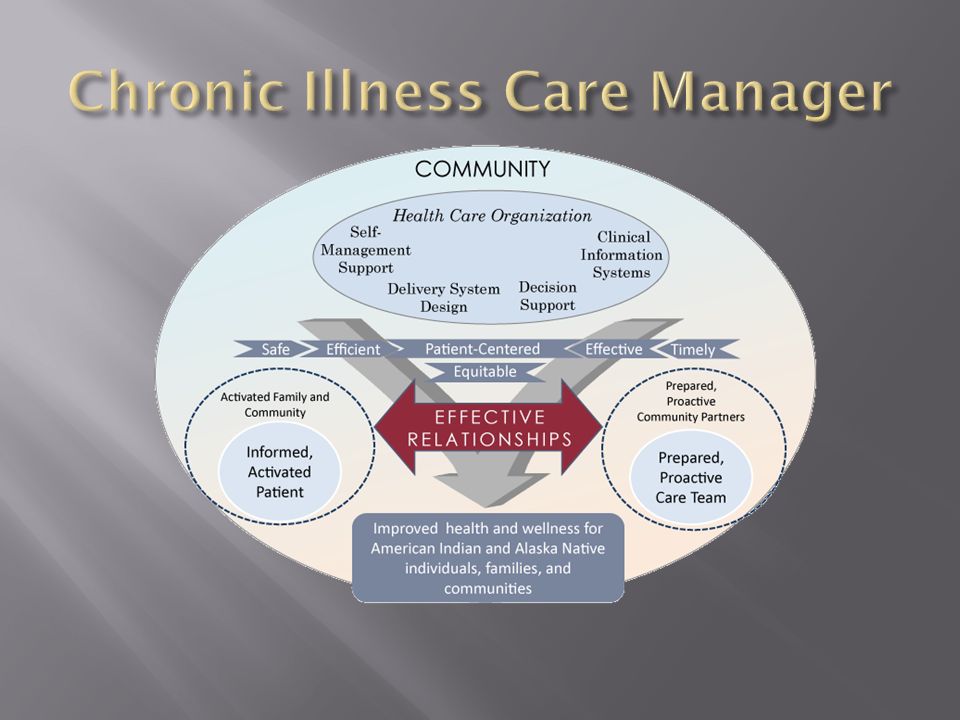
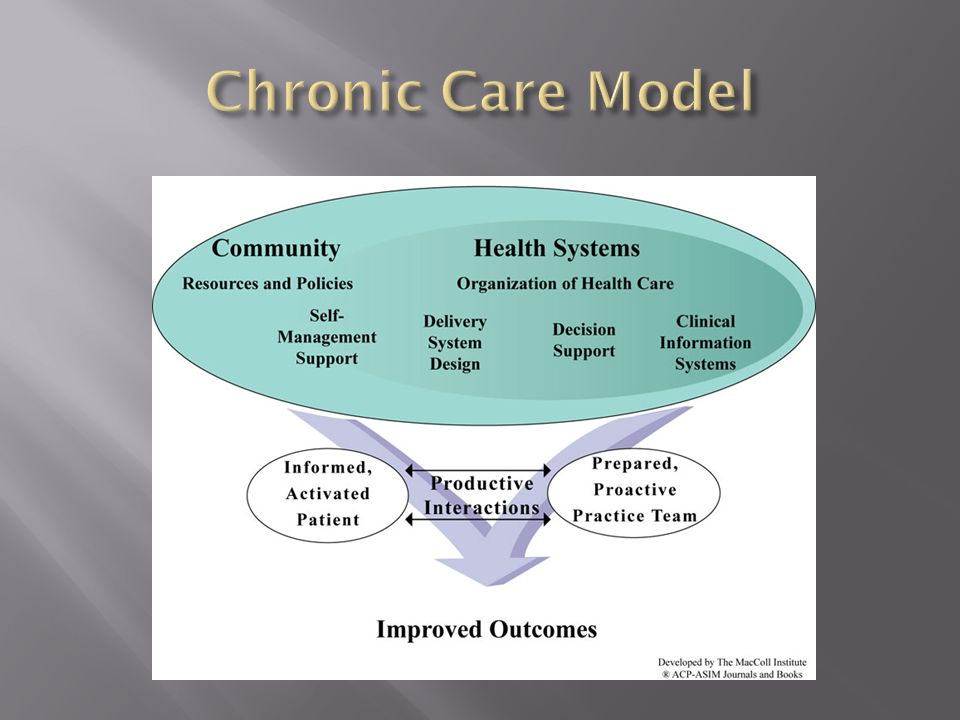
To overcome deficiencies in the current care system including poor compliance with guidelines, poor coordination, and poor patient engagement this model was devised which summarizes the basic elements for improving care in health systems at the community, organization, practice and patient levels.

84
Improvement results from interaction between informed, activated patients and prepared, proactive team of clinicians

85
Improvement occurs on a process level in self- management support, delivery system design, clinical information systems, and decision support

86
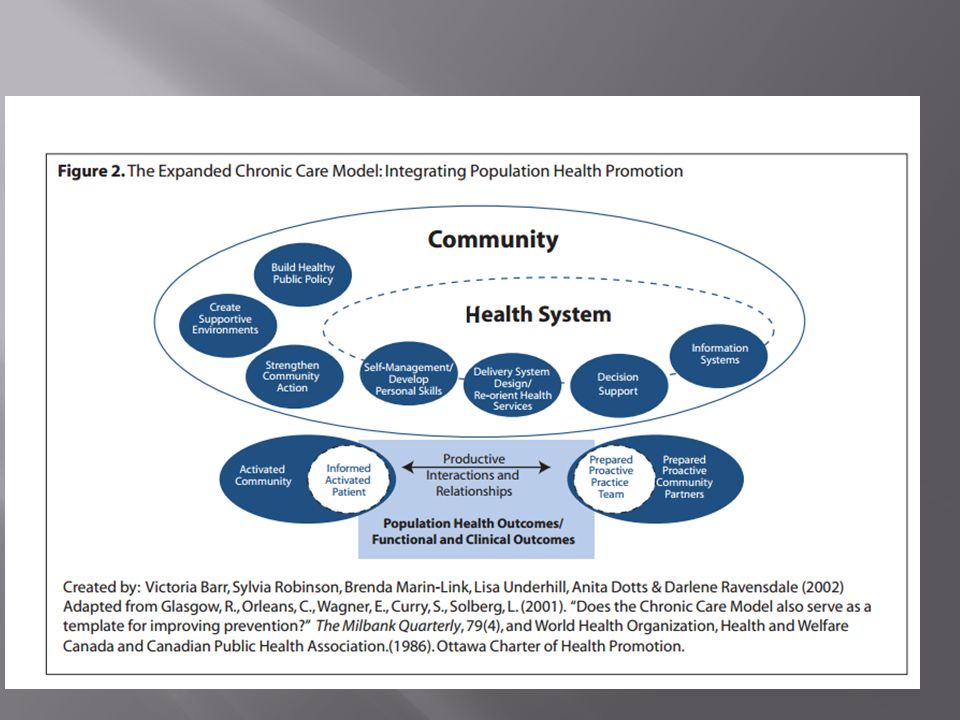
Integration of population health will “connect the dots” Community plays an important role in the social determinants of health Public policy needs to be developed to assist folks in developing personl skills, re-orienting health services to focus away from illness care, build public policy based on creating a healthy environment, and provide support for people who wish to remain (are re-achieve) health
 health")
88
This number reflects the number of patients alive at a specified time following diagnosis (such as after 5 years) divided by the number of patients diagnosed. Can make treatment for diseases such as cancer appear unusually effective

90
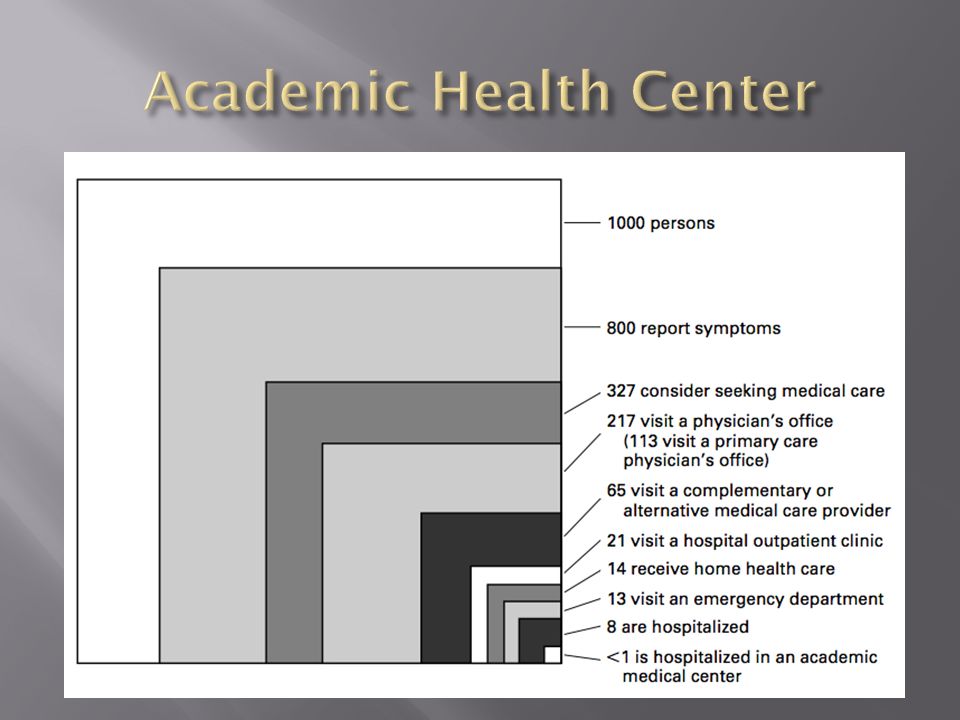
Out of 1000 people, less than one will be cared for in this setting in a given year. It is the setting where most physicians are educated and most research originates in this country

92
This is a ratio of the probabilities of the event occurring in one group (usually the treatment group) versus another group (usually the control group).
 versus another group (usually the control group).")
94
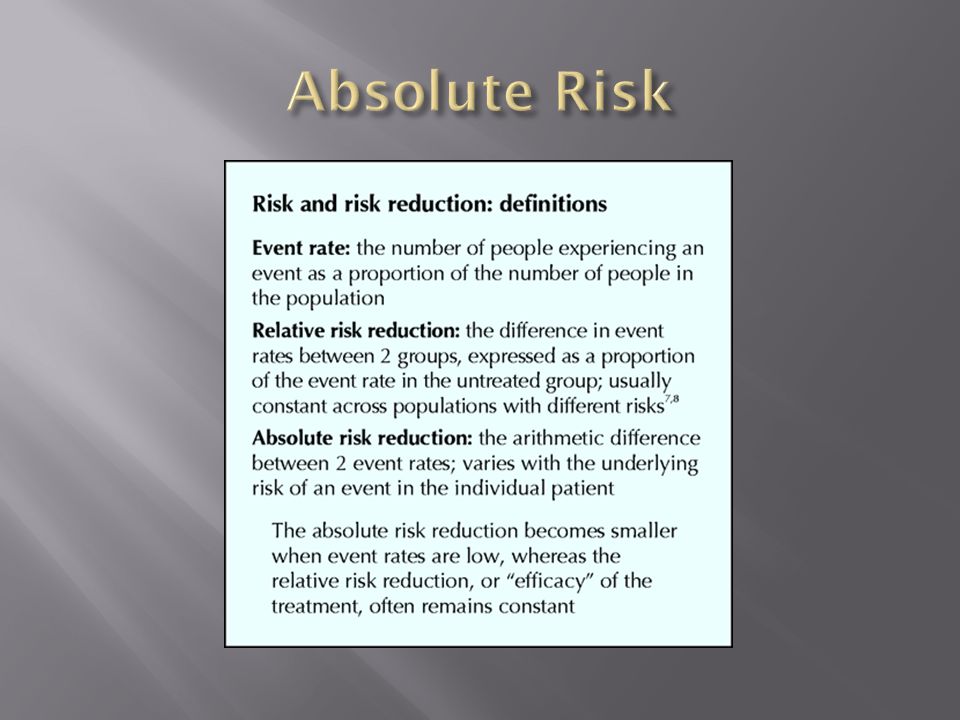
This number is simply the corresponding baseline risk. The reduction of this number is calculated by subtracting the treatment group from the control group:

96
This bias occurs when two tests for a disease are compared, and one test (the new, experimental one) diagnoses the disease earlier, but there is no effect on the outcome of the disease—it may appear that the test prolonged survival, when in fact it only resulted in earlier diagnosis when compared to traditional methods. It is an important factor when evaluating the effectiveness of a specific test.

98
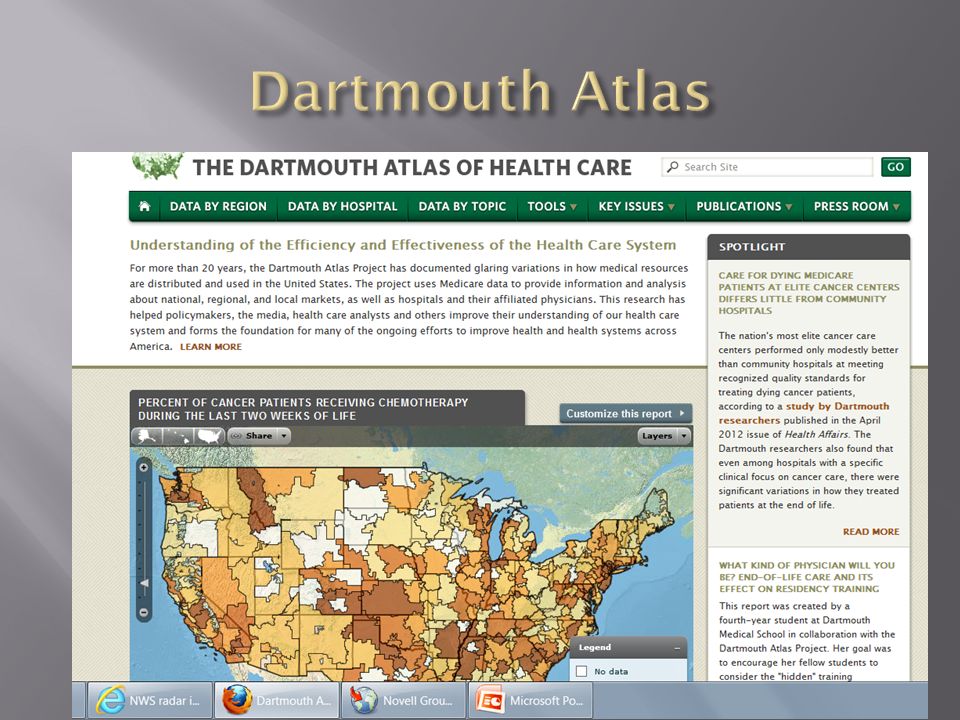
For more than 20 years, these investigators have documented glaring variations in how medical resources are distributed and used in the United States. The project uses Medicare data to provide information and analysis about national, regional, and local markets, as well as hospitals and their affiliated physicians. Their research has helped policymakers, the media, health care analysts and others improve their understanding of our health care system and forms the foundation for many of the ongoing efforts to improve health and health systems across America

100
Click on data by region Group 1 use Hospital Referral Region Select USA, UAB, Providence, and MIMC and Alabama state average Select Terminal care as the topic and view data Group 2 use hospital Service Area Select Mobile, Birmingham, Tuscaloosa, and Alexandria, VA Select physician capacity and discharges for ambulatory conditions Group 3 select Primary care service area Select Mobile, Alabaster, and Uniontown Select number of primary care physicians, specialty physicians, and primary care per population Be prepared to answer questions regarding data and implications

101
Created in 1984, the this group is an independent group of national experts in prevention and evidence-based medicine that works to improve the health of all Americans by making evidence- based recommendations about clinical preventive services such as screenings, counseling services, or preventive medications. The group is made up of 16 volunteer members who come from the fields of preventive medicine and primary care, including internal medicine, family medicine, pediatrics, behavioral health, obstetrics/gynecology, and nursing. All members volunteer their time to serve on the USPSTF, and most are practicing clinicians.

103
The time interval between possible detection by screening and later detection after symptoms. We hope that this early detection of disease will lead to earlier treatment and that this, in turn, will lead to a better outcome. However, this is not always the case.

104
Continued symptom free life

105
This technology allows physicians to proactively manage chronic illnesses, including notifying the patient and physicians regarding required labs and preventive services, and use that information to manage your patient population and identify those needing more aggressive mangement

107
This is the use of multiple medications by a patient, especially when too many forms of medication are used by a patient, when more drugs are prescribed than is clinically warranted, or even when all prescribed medications are clinically indicated but there are too many pills to take (pill burden).
.")
109
In large doses, this can cause serious tissue damage and increase a person’s risk of later developing cancer. In low doses it is used for imaging tests and might increase a person’s cancer risk slightly. The effect of this is cumulative so while a single exam only raises the risk slightly, over time the effect may be more worrisome

113
These are at the center of a major public health crisis of addiction, misuse, abuse, overdose and death. They have come to the attention of the FDA. The agency is paying close attention, trying to reach a balance between continued access to these necessary medications and while developing stronger measures to reduce their risks.

115
This activity of the FDA assists prescribers and distributors of high risk medications to provide appropriate information and monitoring to patients clude, as a goal, informing or educating patients or health care providers of the serious risks of a drug. The information includes a Medication Guide, a communication plan, or a communication-related Element to Assure Safe Use

117
This is an inadvertent adverse effect or complication resulting from medical treatment or advice, including that of psychologists, therapists, pharmacists, nurses, physicians and dentists. Causes include chance, medical error, negligence, social control, unexamined instrument design, anxiety or annoyance related to medical procedures, and the adverse effects or interactions of medications.

119
This is an emerging movement in health insurance where providers are rewarded for meeting pre-established targets for delivery of healthcare services. This payment model rewards physicians, hospitals, medical groups, and other healthcare providers for meeting certain performance measures for quality and efficiency. Disincentives, such as eliminating payments for negative consequences of care (medical errors) or increased costs, have also been proposed.
 or increased costs, have also been proposed..")
121
This process focuses on eliminating waste from processes and increasing process speed by focusing on what customers actually consider quality, and working back from that. It also aims to eliminate process variation and make process improvements based on the customer definition of quality, and by measuring process performance and process change effects.

122
Lean Six Sigma

Similar presentations























 County Health Department.>")





>")