Download presentation
Presentation is loading. Please wait.

2
Titration Protocols BY AHMAD YOUNES PROFESSOR OF THORACIC MEDICINE Mansoura Faculty of Medicine

3
INDICATIONS TO TREAT WITH POSITIVE AIRWAY PRESSURE Administration of positive airway pressure therapy is the treatment of choice for most patients with OSA. CPAP treatment is generally recommended for all patients with an AHI greater than or equal to 15/hour and for symptomatic patients (eg, excessive daytime sleepiness, insomnia, impaired cognition, mood disorder, hypertension, ischemic heart disease, or stroke) with an AHI between 5– 15/hour.
 with an AHI between 5– 15/hour..")
4
Treatment modalities for positive airway pressure Continuous positive airway pressure Provides a constant pressure throughout the respiratory cycle Bi-level positive airway pressure Provides two pressure levels during the respiratory cycle: a higher level during inspiration and a lower pressure during expiration Autotitrating positive airway pressure Provides variable pressures using device-specific diagnostic and therapeutic algorithms. (Auto CPAP, Auto BPAP ) Nocturnal noninvasive positive pressure ventilation Provides two pressure levels at a set rate to assist ventilation.
 Nocturnal noninvasive positive pressure ventilation Provides two pressure levels at a set rate to assist ventilation..")
6
Mechanism of Action Positive airway pressure, via a fan or turbine generated flow of air, function as a pneumatic splint that maintains the patency of the vulnerable portions of the nasopharyngeal airway. Positive airway pressure increases nasal pressure above critical pressure ( Pcrit).
..")
7
Determining optimal CPAP A variety of methods have been used to determine a single optimal CPAP level. These include: 1. In-laboratory attended polysomnographically guided CPAP titration –Full-night studies. –Split-night studies (consists of an initial diagnostic portion and a subsequent CPAP titration on the same night); 2. Unattended laboratory or home titration 3. Use of autotitrating devices. 4. Formula-derived pressures from clinical, polysomnography (PSG), and/or anthropometric variables
; 2. Unattended laboratory or home titration 3. Use of autotitrating devices. 4. Formula-derived pressures from clinical, polysomnography (PSG), and/or anthropometric variables.")
8
Determining optimal CPAP The current standard of practice involves an attended pressure titration during a laboratory PSG, during which sleep stages and respiratory variables are monitored. The goal is to determine a single fixed pressure that eliminates apneas, hypopneas, snoring, and respiratory effort–related arousals (RERAs); maintains adequate oxygen saturation; and improves sleep architecture and quality in all sleep positions and in all sleep stages. It is generally accepted that higher pressures are required to reverse airway occlusion during REM sleep and during sleep in a supine position. Split-night studies can potentially underestimate the severity of OSA
; maintains adequate oxygen saturation; and improves sleep architecture and quality in all sleep positions and in all sleep stages. It is generally accepted that higher pressures are required to reverse airway occlusion during REM sleep and during sleep in a supine position. Split-night studies can potentially underestimate the severity of OSA.")
9
Criteria for split night CPAP titration At least 2 hours of recorded sleep time during the initial diagnostic portion of the study Apnea- hypopnea indices during the diagnostic portion of the study: AHI >40 OR AHI =20–40 (accompanied by significant oxygen desaturation. At least 3 hours are available for CPAP titration with the presence of REM sleep during a supine sleep position

10
American Academy of Sleep Medicine (AASM) recommendations for CPAP and BPAP therapy for adult patients with sleep related breathing disorders The presence of OSA based on an acceptable diagnostic method should be established prior to CPAP therapy (standard). Indications for CPAP therapy include: a. Moderate to severe OSA (standard) b. Mild OSA (option) c. Improvement of subjective sleepiness in patients with OSA (standard) d. Improvement of quality of life in patients with OSA (option) e. As an adjunctive therapy to lower blood pressure in patients with OSA (option) The preferred CPAP titration method to determine optimal positive airway pressure is an in-laboratory, full-night, attended polysomnography, but split-night (initial diagnostic and subsequent titration portion) studies are usually adequate (guideline). Objective monitoring of CPAP use is recommended to ensure optimal utilization (standard).
 b. Mild OSA (option) c. Improvement of subjective sleepiness in patients with OSA (standard) d. Improvement of quality of life in patients with OSA (option) e. As an adjunctive therapy to lower blood pressure in patients with OSA (option) The preferred CPAP titration method to determine optimal positive airway pressure is an in-laboratory, full-night, attended polysomnography, but split-night (initial diagnostic and subsequent titration portion) studies are usually adequate (guideline). Objective monitoring of CPAP use is recommended to ensure optimal utilization (standard)..")
11
American Academy of Sleep Medicine (AASM) recommendations for CPAP and BPAP therapy for adult patients with sleep related breathing disorders Close monitoring of CPAP utilization and any problems that might develop, especially during the first few weeks of use, is important, as is the correction of problems if needed (standard). Addition of heated humidification and a systematic educational program enhance adherence to CPAP use (standard). Patients with OSA treated with CPAP therapy should be followed up yearly or more frequently as needed to correct problems related to its use (option). CPAP and bilevel positive airway pressure (BPAP) therapy are generally safe with minor adverse effects (standard). BPAP can be considered as an optional therapy to CPAP in selected patients who require high pressures, who report difficulty exhaling against a fixed CPAP pressure, or who have coexisting central hypoventilation (guideline). BPAP may also be beneficial in patients with some forms of restrictive lung disease or hypoventilation syndromes with daytime hypercapnia (option).
. Patients with OSA treated with CPAP therapy should be followed up yearly or more frequently as needed to correct problems related to its use (option). CPAP and bilevel positive airway pressure (BPAP) therapy are generally safe with minor adverse effects (standard). BPAP can be considered as an optional therapy to CPAP in selected patients who require high pressures, who report difficulty exhaling against a fixed CPAP pressure, or who have coexisting central hypoventilation (guideline). BPAP may also be beneficial in patients with some forms of restrictive lung disease or hypoventilation syndromes with daytime hypercapnia (option)..")
12
Beneficial effects of positive airway pressure therapy in OSA Upper airway anatomy and function Reduction or elimination of upper airway collapse Reduction or elimination of snoring Decrease in apnea-hypopnea index (AHI) Increase in arterial oxygen saturation (SaO2) Sleep quality Decrease in sleepiness (subjective and objective) Decrease in number of arousals and improvement in sleep quality. Enhancement of neuro-cognitive function Improvement in mood and quality of life

13
Beneficial effects of positive airway pressure therapy in OSA Improvement in driving simulator steering performance. Improvement in blood pressure and heart rate profiles. Improvement in cardiac function. Reversal of the increase in mortality associated with sleep apnea. Reduction in physician claims and hospital stay

14
Adverse consequences of positive airway pressure therapy Aerophagia and gastric distention Barotrauma (eg, pneumothorax, pneumomediastinum, pneumocephalus) Chest discomfort and tightness Claustrophobia, sensation of suffocation or difficulty with exhalation Eye irritation (conjunctivitis) Facial skin irritation, rash or abrasion Mask and mouth leaks Nasal congestion, dryness, epistaxis or rhinorrhea Sleep disruption due to noise from the device Sinus discomfort or pain
 Chest discomfort and tightness Claustrophobia, sensation of suffocation or difficulty with exhalation Eye irritation (conjunctivitis) Facial skin irritation, rash or abrasion Mask and mouth leaks Nasal congestion, dryness, epistaxis or rhinorrhea Sleep disruption due to noise from the device Sinus discomfort or pain")
15
Adherence to Positive Airway Pressure Therapy A large proportion of patients report not being able to tolerate the device. Self-reports often over estimate actual CPAP use. Therapeutic adherence in the different studies has varied from 46% to 80% of patients who use CPAP for 4 or more hours nightly on at least 70% of monitored nights. Factors influencing long-term use include snoring history, severity of illness (AHI), perceived benefit from therapy, and self-reported sleepiness (Epworth Sleepiness Scale [ESS]).
, perceived benefit from therapy, and self-reported sleepiness (Epworth Sleepiness Scale [ESS])..")
16
Adherence to Positive Airway Pressure Therapy Patterns of nightly use are often discernible by the first few days or weeks of initiating treatment. Adherence to CPAP therapy may be improved with education (eg, additional home visits, participation in group clinics, periodic phone calls to uncover any problems and to encourage use, and even simple written information on the importance of regular CPAP use), airway humidification, proper selection of the CPAP interface, desensitization procedures for CPAP, early follow-up, prompt and aggressive management of adverse effects related to CPAP use, and regular assessment of CPAP adherence.
, airway humidification, proper selection of the CPAP interface, desensitization procedures for CPAP, early follow-up, prompt and aggressive management of adverse effects related to CPAP use, and regular assessment of CPAP adherence..")
17
Techniques that may increase CPAP utilization CPAP education and support Humidification Correction of nasal problems Nasal vs. full-face masks Sedative-hypnotics C-flex BPAP

18
Other Modes of Positive Airway Pressure A ) Autotitrating positive airway pressure Because the required positive airway pressure can differ considerably with sleeping posture and sleep stages, optimal positive airway pressure may have significant intra-night and inte-rnight variability. The causes of this variability are 1-Changes in percentage of REM sleep 2-Changes in percentage of different sleep positions (supine vs. non supine) 3-Changes in nasal resistance (eg, congestion) 4-Use of muscle relaxants, sedatives and opioids. 5-Change in weight
 3-Changes in nasal resistance (eg, congestion) 4-Use of muscle relaxants, sedatives and opioids. 5-Change in weight.")
19
Auto-titrating positive airway pressure (APAP) Auto-titrating positive airway pressure (APAP) devices automatically and continuously Adjust the delivered pressure, as required, to maintain airway patency. Pressure is increased if apneas, hypopneas, airflow limitation or snoring are present, or is gradually reduced if no respiratory events are detected over a predetermined period. These devices have been used to help identify a fixed single pressure for subsequent treatment with a conventional CPAP device (APAP titration) or in a self- adjusting mode for nightly therapy of OSA (APAP treatment).
 or in a self- adjusting mode for nightly therapy of OSA (APAP treatment)..")
20
Studies have shown no significant differences between conventional in-laboratory CPAP titration and APAP titration in reductions of AHI and arousal indices, changes in sleep architecture, oxygenation, or subsequent CPAP acceptance. APAP treatment has been demonstrated to be comparable to conventional constant-pressure CPAP therapy. Different devices may utilize different algorithms for monitoring respiratory events (eg, snoring, airflow limitation, apnea-hypopneas, or impedance) and for altering delivered pressures. Auto-titrating positive airway pressure
 and for altering delivered pressures. Auto-titrating positive airway pressure.")
21
Advanced methods of auto-titration Newer generation devices can increase the IPAP alone in order to ameliorate obstructive events (Auto Bi-level PAP),correct hypoventilation (averaged volume assured pressure support [AVAPS], Intelligent Volume Assured Pressure Support (iVAPS ) or combine Auto Bi-level PAP with auto-CPAP (Auto-trilevel) or combat central apneas in patients with complex sleep apnea (Servo- Ventilation). Devices may also introduce a back-up rate to prevent central apneas and although in general they are not referred to as APAP devices, they function using similar principles and can be judged as the latest generation of APAP devices.
![Advanced methods of auto-titration Newer generation devices can increase the IPAP alone in order to ameliorate obstructive events (Auto Bi-level PAP),correct hypoventilation (averaged volume assured pressure support [AVAPS], Intelligent Volume Assured Pressure Support (iVAPS ) or combine Auto Bi-level PAP with auto-CPAP (Auto-trilevel) or combat central apneas in patients with complex sleep apnea (Servo- Ventilation).](http://images.slideplayer.com/36/10566244/slides/slide_21.jpg "Devices may also introduce a back-up rate to prevent central apneas and although in general they are not referred to as APAP devices, they function using similar principles and can be judged as the latest generation of APAP devices..")
22
Autobilevel positive airway pressure with a minimum EPAP of 6 cm H2O and a maximum IPAP of 25 cm H2O.

23
BiPAP AVAPS and VPAP™ ST with iVAPS

24
BiPAP AVAPS

25
BiPAP A40 Ventilator BiPAP A40 comes with well-known and clinically proven Philips Respironics technology such as Auto-Trak, AVAPS and a Dry Box humidifier design. The device is capable of non invasive and invasive pressure ventilation, up to 40 cmH 2 O, providing treatment for your chronic respiratory insufficiency patients. The device features AVAPS-AE, the first fully automatic ventilation mode, designed to help clinicians during titration process, while maintaining comfort and therapy optimization at the lowest pressures.

26
BiPAP A40 Ventilator This new innovative ventilation mode helps in providing long term therapy compliance regardless of changes to the body position, sleep stages and respiratory mechanics. Detachable Battery with up to 5 Hours Backup AVAPS-AE Automatically Adjust Ventilation to the Patients Need Compatible with PSG Systems Optional Oximetry Module Intuitive, User Friendly & Colored Interface Integrated Heated Humidifier Graphical & Statistical Data Management on Encore Pro & Direct View Soft wares

27
Ventilation modes : CPAP, S, S/T, PC, T, AVAPS-AE Hybrid ventilation AVAPS (Average Volume Assured Pressure Support) AVAPS-AE IPAP 4 – 40 cm H 2 O EPAP 4 – 25 cm H 2 O Target tidal volume (when AVAPS enabled) 200 – 1500 ml Breath rate 0 – 40 bpm (4 – 40 bpm in T mode) Inspiratory time 0.5 – 3 sec. Triggering and cycling Auto-Trak,Sensitive Auto-Trak, Flow triggering. Rise time 1 (100 ms) – 6 (600 ms) Size 21.6 cm W x 19 cm L x 11.5 cm H Weight 2.1 Kgs (with power supply) SPECIFICATIONS
 – 6 (600 ms) Size 21.6 cm W x 19 cm L x 11.5 cm H Weight 2.1 Kgs (with power supply) SPECIFICATIONS.")
28
Humidification System One humidity control and ‘Dry Box’ technology Alarms Patient disconnection Apnea,Low minute ventilation,Low tidal volume (with AVAPS/AVAPS-AE only),High RR Monitoring Pressure, tidal volume, minute ventilation, respiratory rate, leak, I/E ratio Battery back up Detachable battery module: 5 hours DC power source 12 VDC, 5.0 A (external battery), 24 VDC, 4.2 A (power supply) Data management Encore Pro 2 and Direct View software Compatible with oximetry module Advanced detection of residual respiratory events(Obstructed Airway Apnea, Clear Airway Apnea, Hypopnea, Periodic Breathing, RERA, Large Leak and Snore)
,High RR Monitoring Pressure, tidal volume, minute ventilation, respiratory rate, leak, I/E ratio Battery back up Detachable battery module: 5 hours DC power source 12 VDC, 5.0 A (external battery), 24 VDC, 4.2 A (power supply) Data management Encore Pro 2 and Direct View software Compatible with oximetry module Advanced detection of residual respiratory events(Obstructed Airway Apnea, Clear Airway Apnea, Hypopnea, Periodic Breathing, RERA, Large Leak and Snore)")
29
VPAP™ ST with iVAPS

30
Why Alveolar Ventilation? Gas exchange only occurs at alveolar level We have a continuous demand for a supply of O2 and removal of CO2 Conducting airways do NOT participate in gas exchange

31
Anatomical Dead space Inspired/expired air remaining in conducting airways Not involved in gas exchange Correlation between patient’s height and dead space (Vd) Height is used to calculate anatomical dead space (Vd) for each breath of air (Tidal Volume) Example dead space volume (Vd) : 120 ml for height 175 cm or 70 inches
 Height is used to calculate anatomical dead space (Vd) for each breath of air (Tidal Volume) Example dead space volume (Vd) : 120 ml for height 175 cm or 70 inches")
32
Anatomical dead space in relation to height of the patient

33
Alveolar Ventilation Vt (500ml) – Vd (120ml) = alveolar ventilation for one breath 500 - 120 = 380 ml participates in gas exchange for each breath Vta x RR (respiratory rate) = Va (minute alveolar ventilation) = 0.380 x 15 = 5.7L/min Benefits Of Alveolar Ventilation Supply of O2 (PaO2).Normal = 80 – 100 mm Hg Removal of CO2 (PaCO2). Normal = 35 – 45 mm Hg Alveolar ventilation provides necessary gas exchange to satisfy metabolic demand

34
As alveolar ventilation drops, iVAPS rapidly increase pressure support until target Va is reached, and as alveolar ventilation increase, iVAPS rapidly decrease pressure support.

35
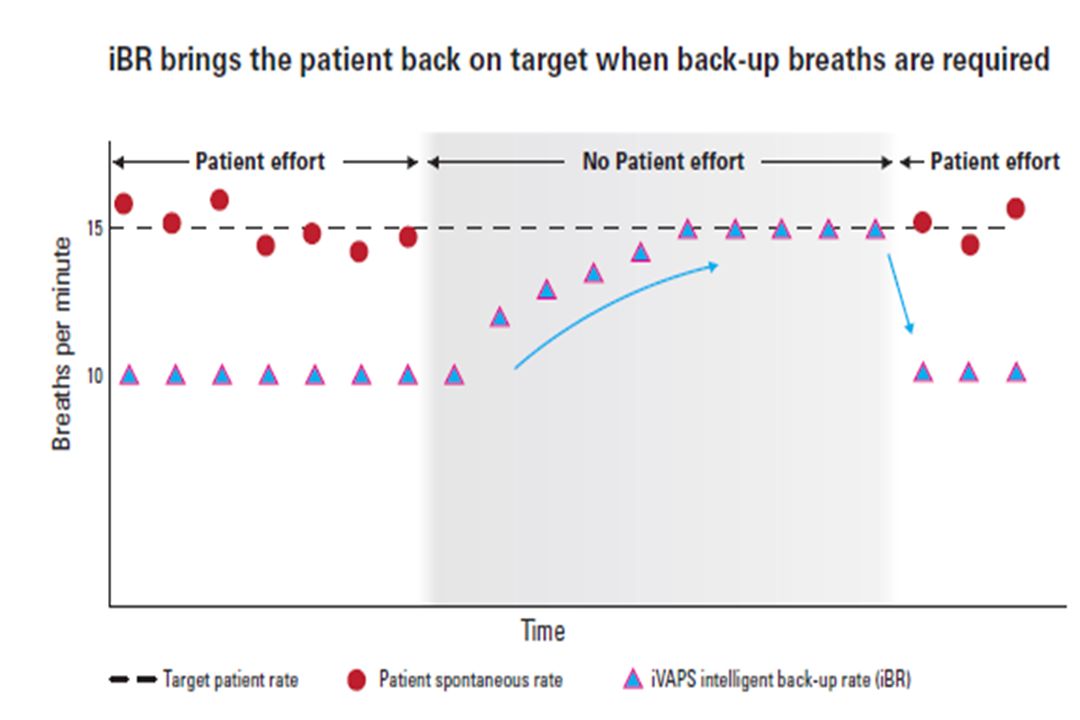
Intelligent back up rate (iBR) stays out of the way at 2/3 spontaneous rate whenever the patient spontaneously triggers above 2/3 of the target. once the patient rate reach minimum back up rate (2/3 of the target ) iBR increase towards patient spontaneous rate to maintain alveolar ventilation.Once spontaneous trigering returns, iBR drops back to 2/3 of the target / spontaneous rate.
 iBR increase towards patient spontaneous rate to maintain alveolar ventilation.Once spontaneous trigering returns, iBR drops back to 2/3 of the target / spontaneous rate..")
36
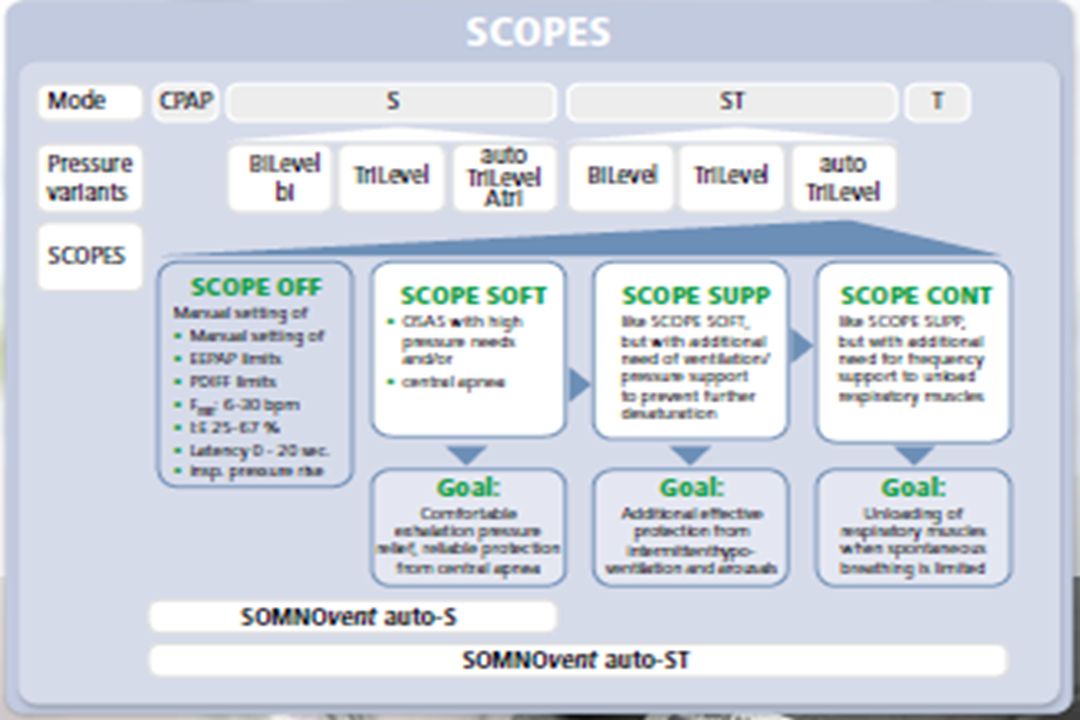
Auto-TriLevel The auto-TriLevel principle by Weinmann combines two proven types of therapy – auto-CPAP and BiLevel – into a synthesis that offers the most therapy effectiveness. Your benefits with these products: Therapeutically effective maximum and mean pressures that are lower than BiLevel with the same tidal volume for fewer side effects such as leakage. It‘s like a new titration every day – adjusts to patient‘s high variability. Effortless titration and monitoring.

37
Auto-TriLevel IPAP: inspiratory pneumatic splinting of the airways (ventilation) EPAP: easier exhalation at a low expiratory pressure level for a pleasant breathing sensation Additional end-expiratory pressure (EEPAP): required minimum pressure for adequate splinting of airways during phase when risk of collapse is highest PDIFF (Δ IPAP-EPAP): need- oriented ventilation support by means of changes between inspiratory (IPAP) and expiratory (EPAP) pressure levels
 EPAP: easier exhalation at a low expiratory pressure level for a pleasant breathing sensation Additional end-expiratory pressure (EEPAP): required minimum pressure for adequate splinting of airways during phase when risk of collapse is highest PDIFF (Δ IPAP-EPAP): need- oriented ventilation support by means of changes between inspiratory (IPAP) and expiratory (EPAP) pressure levels")
38
Auto-TriLevel Reduced mean and maximum therapy pressure under TriLevel: Results of a bench test comparison with BiLevel therapy. SOMNOvent auto-ST is the world‘s first automatic BiLevel device that permits goal-oriented therapy settings(SCOPES). With the combination of the autoTriLevel principle and the automatic trigger WM trak, this device delivers the greatest effectiveness, reliability and breathing comfort – simply the fastest therapy results. Particularly for cases of complicated SDB, SOMNOvent auto-S, convinces with its intelligent combination of automatic BiLevel S therapy and auto-CPAP.
. With the combination of the autoTriLevel principle and the automatic trigger WM trak, this device delivers the greatest effectiveness, reliability and breathing comfort – simply the fastest therapy results. Particularly for cases of complicated SDB, SOMNOvent auto-S, convinces with its intelligent combination of automatic BiLevel S therapy and auto-CPAP..")
40
Auto-TriLevel Auto-bilevel spontaneous (SOMNOvent auto-S ). Auto-bilevel spontaneous/timed (SOMNOvent auto-ST ). Anti-cyclic modulated ventilation (SOMNOvent auto-CR ).
. Anti-cyclic modulated ventilation (SOMNOvent auto-CR )..")
41
Stellar TM 150

42
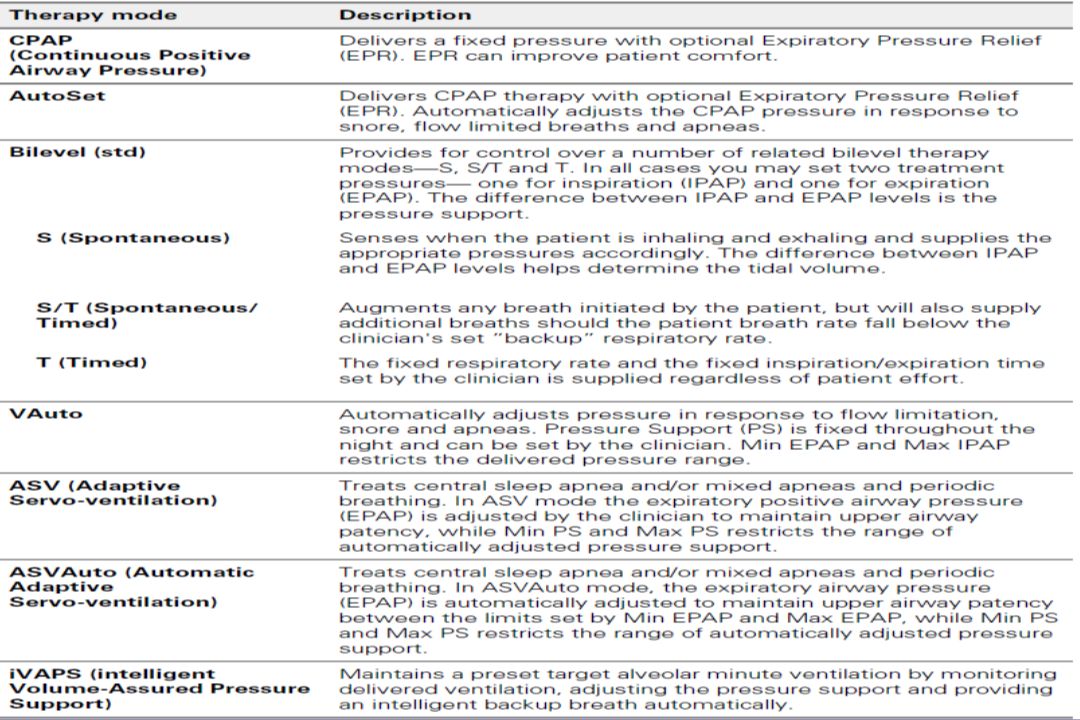
Stellar provides the following modes: CPAP mode—a fixed pressure is delivered. S (Spontaneous) mode—the device senses the patient breath and triggers IPAP in response to an increase in flow, and cycles into EPAP at the end of inspiration. The breath rate and the respiratory pattern will be determined by the patient. ST (Spontaneous/Timed) or PS (Pressure Support) mode—the device augments any breath initiated by the patient, but will also supply additional breaths should the patient breath rate fall below the clinician's set ’backup’ breath rate. T (Timed) mode—the fixed breath rate and the fixed inspiration time set by the clinician are supplied regardless of patient effort.
 mode—the device senses the patient breath and triggers IPAP in response to an increase in flow, and cycles into EPAP at the end of inspiration. The breath rate and the respiratory pattern will be determined by the patient. ST (Spontaneous/Timed) or PS (Pressure Support) mode—the device augments any breath initiated by the patient, but will also supply additional breaths should the patient breath rate fall below the clinician s set ’backup’ breath rate. T (Timed) mode—the fixed breath rate and the fixed inspiration time set by the clinician are supplied regardless of patient effort..")
43
Stellar provides the following modes: PAC (Pressure Assist Control)—the inspiration time is preset in the PAC mode. There is no spontaneous/flow cycling. The inspiration can be triggered by the patient when respiratory rate is above a preset value, or time triggered breaths will be delivered at the backup breath rate. iVAPS (intelligent Volume Assured Pressure Support) designed to maintain a preset target alveolar ventilation by monitoring delivered ventilation, adjusting the pressure support and providing an intelligent backup breath automatically. The iVAPS therapy mode is indicated for patients 66 lb (30 kg) and above.
 designed to maintain a preset target alveolar ventilation by monitoring delivered ventilation, adjusting the pressure support and providing an intelligent backup breath automatically. The iVAPS therapy mode is indicated for patients 66 lb (30 kg) and above..")
44
iVAPS (intelligent Volume Assured Pressure Support) The iVAPS therapy mode is indicated for patients 30 kg and above. You may prefer some assurance that the patient's ventilatory needs will be maintained if their condition varies. A variety of ‘dual mode’ schemes exist, that aim to combine the benefits of pressure target and volume target, most of which can be categorized generically as volume assured pressure support, or VAPS modes. With VAPS devices in general, the ventilatory assistance (pressure support) aims to automatically adjust to changes in patient condition over time, typically to maintain a target tidal volume.
 aims to automatically adjust to changes in patient condition over time, typically to maintain a target tidal volume..")
45
iVAPS (intelligent Volume Assured Pressure Support) iVAPS offers the comfort and synchrony of pressure support, but with the assurance offered by a volume target. iVAPS has the following advantages over traditional VAPS schemes: iVAPS is a unique combination for a servo-controlled ventilator, in that iVAPS has the goal of regulating alveolar ventilation to a prescribed target, and iVAPS has a rapid but gentle servo-control response. iVAPS is tuned to be fast enough to avoid blood-gas derangement associated with most breathing challenges, including during sleep, but is gentle enough to avoid disruption. iVAPS has an intelligent Backup Rate (iBR) which aims to keep ‘out of the way’ while the patient is breathing, yet during sustained apnea will mimic the patient's own breath rate.
 which aims to keep ‘out of the way’ while the patient is breathing, yet during sustained apnea will mimic the patient s own breath rate..")
48
Pathology Defaults A choice of disease-specific preset values, based on commonly-used clinical values for obstructive, restrictive, obesity hypoventilation and normal lung mechanics. Advanced settings are optimized so medical staff can focus on fine-tuning primary settings for each patient. Before use you will need to review the set parameters on the Clinical Settings screen.

49
Pathology Defaults

50
SomnoVent CR Respironics autoSV ResMed VPAP Adapt SVRespironics autoSVResMed VPAP Adapt SV

51
ASV is a variant of BPAP that was developed to treat Cheyne-Stokes central apnea. Both ASV and BPAP devices with a backup rate are approved for use with patients with central apnea and complex sleep apnea

52
AASM recommendations for autotitrating CPAP for OSA (STANDARD) 1. The presence OSA must be diagnosed using an acceptable method. 2. APAP titration or treatment is not indicated for patients with the following medical conditions: Congestive heart failure, Significant respiratory diseases such as COPD or daytime hypoxemia and respiratory failure from any cause, nocturnal arterial oxygen desaturation secondary to disorders other than OSA (eg, OHS) 3. Non snorers should not be titrated with APAP devices using diagnostic algorithms that rely on vibration or sound production.
 3. Non snorers should not be titrated with APAP devices using diagnostic algorithms that rely on vibration or sound production..")
53
AASM recommendations for autotitrating CPAP for OSA (STANDARD) 4. APAP devices are not recommended for split- night CPAP titration. 5. Patients who are being treated with APAP or with fixed CPAP based on APAP titration should be monitored for effectiveness and safety of therapy. 6. If APAP or CPAP therapy is considered ineffective (ie, symptoms fail to resolve), re- evaluation and standard attended CPAP titration should be performed.
, re- evaluation and standard attended CPAP titration should be performed..")
54
AASM recommendations for autotitrating CPAP for OSA (GUIDELINE) Certain APAP devices may be used to determine a single CPAP pressure during attended polysomnography for the therapy of OSA (APAP titration). Certain APAP devices may be used in a self-adjusting mode for the therapy of OSA after an initial successful attended polysomnography-guided CPAP or APAP titration (APAP treatment). OPTION 1. The use of unattended APAP to determine pressures for fixed CPAP or to treat CPAP-naive patients in a self- adjusting APAP mode has not been established.
. OPTION 1. The use of unattended APAP to determine pressures for fixed CPAP or to treat CPAP-naive patients in a self- adjusting APAP mode has not been established..")
55
B ) Bilevel positive airway pressure BPAP devices provide two pressure levels during the respiratory cycle, namely a higher level during inspiration (inspiratory positive airway pressure; IPAP) and a lower pressure during expiration (expiratory positive airway pressure; EPAP). Patients with OSA who have persistent oxygen desaturation due to hypoventilation despite CPAP therapy may benefit from BPAP. When used for patients with OSA, levels of EPAP are titrated to eliminate apneas, and IPAP is progressively increased until hypopneas and snoring are controlled.

57
Representative tracings of flow, tidal volume, and airway pressure (Paw) during administration of continuous positive airway pressure (CPAP) and bi-level PAP
 during administration of continuous positive airway pressure (CPAP) and bi-level PAP")
58
BPAP may also be considered for Patients with OSA who are unable to tolerate CPAP and complain of being unable to breathe out against high CPAP expiratory pressures, significant mouth leaks or aerophagia, Those with concurrent chronic obstructive pulmonary disease (overlap syndrome),or Those in whom hypoventilation (eg, OHS or neuromuscular weakness) is suspected.
,or Those in whom hypoventilation (eg, OHS or neuromuscular weakness) is suspected.")
59
C ) Noninvasive positive pressure ventilation Noninvasive positive pressure ventilation (NIPPV) may be required in selected patients with persistent sleep-related hypoventilation and CO2 retention despite therapy with CPAP and supplemental oxygen. NIPPV, which can be provided using a volume- cycled ventilator, can improve ventilation and arterial blood gas values during both wakefulness and sleep. Some patients on NIPPV are able to resume CPAP therapy at a later time.

60
TITRATION TECHNIQUES

61
General Titration Considerations The current standard of care dictates CPAP therapy be commenced and titrated under direct supervision by a trained technician. Direct supervision allows for immediate assessment of various sleep-related disturbances, direct determination of the optimal CPAP pressure, and identification of significant sleep-related co-morbidities, including but not limited to nocturnal seizures, cardiac arrhythmias, parasomnia activity, nocturnal myoclonus, persistent hypoxemia with PAP therapy in the absence of overt respiratory events, which may in turn require additional titration of supplemental oxygen.

62
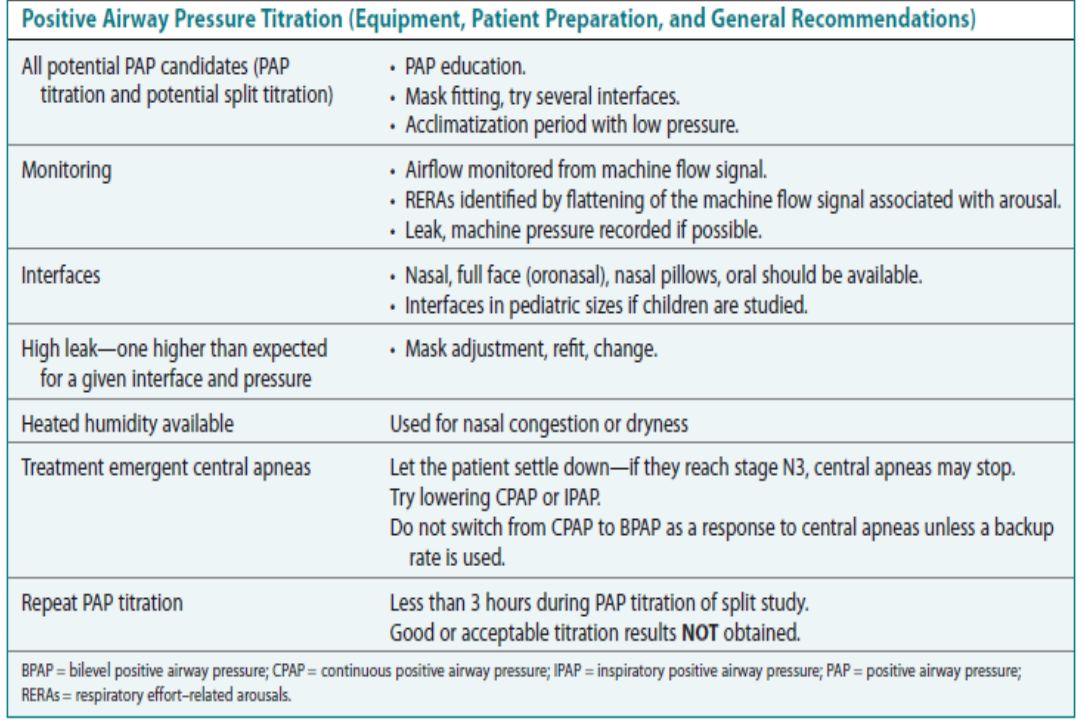
General Titration Considerations A polysomnography (PSG) is the standard method for PAP titration and is usually accomplished either as the second part of a split study or during an entire night after a previous diagnostic study. A split study is recommended only if the AHI is greater than 40/hr and 2 hours of monitoring have occurred. In addition, 3 hours of PAP titration is the minimum acceptable duration. If an adequate titration is not obtained, a repeat PSG titration is indicated.

65
Before the initiation of the PAP titration Extensive education about the pathophysiology of OSA, the consequences of untreated OSA, as well as PAP therapy should be given to the patient. Videotapes and supplemental reading are additional tools that may help patient adherence. Ensure optimal mask fit in order to improve comfort and reduce the potential for mask leak. In some cases, a chin strap or a full-face mask may be required to eliminate mouth breathing, which should be assessed once the titration study has begun.

66
The endpoint of the titration When determining a titration algorithm, it is essential to understand that elimination of apneas, hypopneas, and oxygen desaturations is the first objective, but not the endpoint of the titration. The endpoint of the titration should be elimination of snoring and respiratory-related arousals in all positions and all stages of sleep. Persistent inspiratory airflow limitation is evidenced by a flattened airflow pressure tracing and can best be demonstrated with titrations that are performed with nasal pressure-flow transducers, as opposed to thermistors or other indirect measures of airflow.

67
Assessing increased respiratory effort due to flow limitation Although esophageal pressure monitoring is the most accurate means of assessing increased respiratory effort due to flow limitation, this modality is often poorly tolerated which may in turn limitits routine use in CPAP titration studies. When inspiratory airflow limitation is associated with spontaneous arousals, it is likely due to upper airway resistance syndrome (UARS) and a further increase in airway pressure is indicated. Careful monitoring of esophageal pressures, and/or CPAP airflow signals, generally demonstrates continued evidence of airflow resistance until CPAP pressures have been increased to 2 cm H2O, on average, above that needed to eliminate apneas and hypopneas.
 and a further increase in airway pressure is indicated. Careful monitoring of esophageal pressures, and/or CPAP airflow signals, generally demonstrates continued evidence of airflow resistance until CPAP pressures have been increased to 2 cm H2O, on average, above that needed to eliminate apneas and hypopneas..")
68
Upward then downward titration Patients undergoing CPAP titration may display increased pressure requirements during titration from lower CPAP pressures upward, as compared to pressures required during downward titration from higher pressures. It is appropriate during a titration study to titrate pressures upward until elimination of respiratory events has been achieved and a normal airflow pattern is attained; and then titrate downward to the return of obstructive events. This method is of particular use in patients who have difficulty tolerating PAP therapy due to high pressure requirements.

69
Optimal pressure When performing a titration, it is important to note sleep stage and body position once optimal pressure is assumed as evidence that suggests that higher pressure requirements may be needed in the supine position and in REM sleep. Once an optimal pressure has been attained, in addition to resolution of sleep related breathing events, sleep continuity should theoretically improve, with a decrease in the number of spontaneous arousals and arousals associated with respiratory events. Commonly, slow- wave sleep rebound or REM sleep rebound will be seen with improved sleep continuity and this finding can be used as an indication that an effective pressure level is imminent.

70
Emergence of central apneas It has been shown that increased tidal volumes can induce central apneas in the setting of normocapnia due to neurochemical inhibition and possibly, baroreceptor activity. This finding has led to the practice of decreasing CPAP pressures when the emergence of central apneas is witnessed during an upward titration. It is important to continue to explore upward pressures with the appearance of central apneas, as there are several mechanisms that have been shown to elicit central apneas, including upper airway obstruction, which may be indicative of sub-therapeutic pressures.

71
Bilevel mode of delivery of breath It has been shown that lower expiratory pressures are required to maintain airway patency than with inspiration. The efficacy of using bilevel ventilation as a standard treatment modality in all patients with OSA is questionable; however, clinicians tend to consider unacceptably high CPAP pressures, as deemed by intolerance of the pressure by the patient during the study, as an indication to change to bilevel mode of ventilation. Clinicians generally feel that patients with lung disease, chest-wall disease, and/or neuromuscular disease may be most appropriate for bilevel mode of delivery of breath.

72
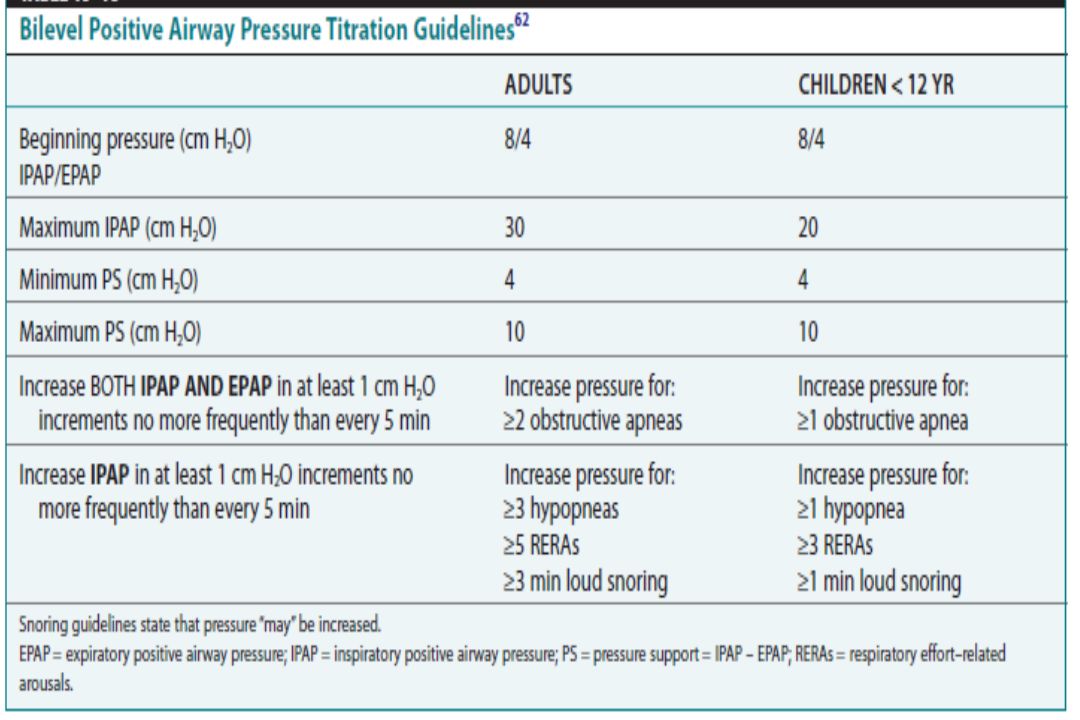
Standardized titration methods While CPAP therapy has been the standard of care for many years, there is a surprising lack of data validating standardized titration methods. In particular, details on the transition from CPAP therapy to bilevel therapy are lacking. In patients with OSA intolerant of CPAP, there exist primarily three different techniques employed: (i) an inspiratory pressure is chosen equal to the CPAP pressure where obstructive events were eliminated; (ii) an expiratory pressure is chosen equal to the CPAP pressure where obstructive events were eliminated; (iii) bilevel is initiated from a low starting pressure, beginning with baseline pressure settings and titrating upwards.
 an inspiratory pressure is chosen equal to the CPAP pressure where obstructive events were eliminated; (ii) an expiratory pressure is chosen equal to the CPAP pressure where obstructive events were eliminated; (iii) bilevel is initiated from a low starting pressure, beginning with baseline pressure settings and titrating upwards..")
73
Standardized titration methods Regardless of the technique followed, it is generally thought that a 4 cm H2O difference should be preserved in order to maintain airway patency during expiration. Commonly, expiratory pressure increases are performed in the setting of persistent or reappearing apneas, while inspiratory pressure increases are made in the setting of snoring, flow limitation, or hypopneas, maintaining a 4 cm difference between the two.

74
Standardized titration methods The use of BPAP in patients with OHS should be initiated in a similar fashion; however, if hypoxemia persists after resolution of respiratory events, in particular during REM sleep, the addition of supplemental oxygen in these patients is appropriate. Special consideration is needed when using BPAP in patients with central sleep apnea (CSA) not responsive to CPAP, especially patients with CSA-CSR in the absence of OSA. These patients will often need a “timed mode” of inspiration as the bilevel unit will not be triggered due to lack of inspiratory effort.
 not responsive to CPAP, especially patients with CSA-CSR in the absence of OSA. These patients will often need a timed mode of inspiration as the bilevel unit will not be triggered due to lack of inspiratory effort..")
75
Standardized titration methods Adaptive servo ventilation ( ASV) has been developed in the hope of creating a more effective means of treating CSA-CSR and improving adherence. ASV ventilation provides positive expiratory airway pressure and inspiratory pressure support that is servo-controlled based on the detection of CSR, with a backup respiratory rate. Initial studies show great promise for this device as means of effectively controlling CSA- CSR.

76
Standardized titration methods The use of “daytime” titrations is another method that has been proposed to derive optimal pressure settings. Limited efficacy and adherence data call this technique into question though initial nonrandomized cohort studies do show some comparable results to overnight titrations.

77
Factors contributing to the therapeutic efficacy of PAP therapy over time In the absence of significant clinical changes, a pressure level chosen during a single night’s titration is generally effective on longitudinal nights. However, CPAP non adherence, coexisting sleep fragmenting disorders, significant weight gain and chronic medical or psychiatric conditions and nasal congestion are all factors that can alter the efficacy of CPAP therapy.If a patient who initially responded to treatment begins to complain of recurrent symptoms, consider these contributing factors as a potential cause. It is imperative for the clinician to consider all causes of “residual hypersomnolence” in the treated OSA patient, and the most common cause of sleepiness is insufficient sleep.

78
PERIOPERATIVE MANAGEMENT Patients undergoing any surgical procedure are susceptible to postoperative complications due to respiratory compromise. Patients with OSA are at obvious risk for a postoperative complication due to the perioperative use of narcotics and benzodiazepines, which are known to blunt the respiratory response to hypercapnea and to hypoxia as well as exacerbate upper airway obstruction Unfortunately, many patients undergoing surgical procedures are not appropriately screened for OSA and may be put at risk for postoperative complications, in particular patients having outpatient surgical procedures who are sent home to a completely unmonitored environment.

79
PERIOPERATIVE MANAGEMENT The American Society of Anesthesiologists (ASA) have recognized the risk of postoperative complications associated with patients who have undiagnosed OSA and thereby published practice guidelines outlining recommendations of how to identify and treat patients at risk. The ASA practice parameters suggest that preoperatively, anesthesiologists should work with surgeons to develop a protocol whereby patients in whom the possibility of OSA is suspected on clinical grounds are evaluated long enough before the day of surgery to allow preparation of a perioperative management plan. The recommendations go on to include preoperative preparation where preoperative initiation of CPAP should be considered, particularly if OSA is severe.

80
PERIOPERATIVE MANAGEMENT Because of their propensity for airway collapse and sleep deprivation, patients with OSA are especially susceptible to the respiratory depressant and airway effects of sedatives,narcotics, and inhaled anesthetics. In selecting intraoperative medications, the ASA practice parameters suggest that the potential for postoperative respiratory compromise should be considered. Regional analgesic (pain relief) techniques should be considered to reduce or eliminate the requirement for systemic opioids (narcotics) in patients at increased perioperative risk from OSA. Before patients at increased perioperative risk from OSA are scheduled for surgery, a determination should be made regarding whether a given surgical procedure is most appropriately performed on an inpatient or outpatient basis.
 techniques should be considered to reduce or eliminate the requirement for systemic opioids (narcotics) in patients at increased perioperative risk from OSA. Before patients at increased perioperative risk from OSA are scheduled for surgery, a determination should be made regarding whether a given surgical procedure is most appropriately performed on an inpatient or outpatient basis..")
81
MONITORING

83
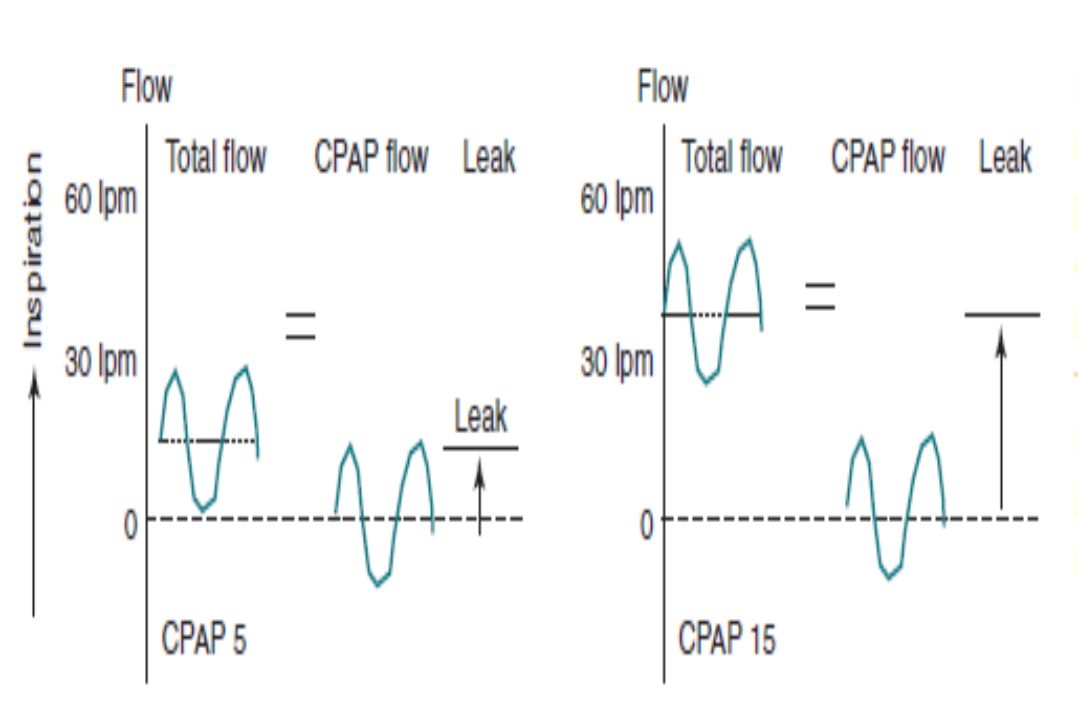
Monitoring during Positive Pressure Titration Most positive-pressure devices used in the sleep disorders center provide several analog or digital outputs that can be recorded. The total flow delivered by the machine is measured by an accurate flow sensor in the PAP device. Use of a thermal device under the mask to monitor flow is not recommended. The total flow is then divided by the device into two components that are supplied for monitoring: (1) the PAP flow (also known as CPAP flow, C flow, or machine flow), which varies with inspiration and expiration, and (2) the leak (bias flow), which is a fairly constant portion due to system leak.
 the PAP flow (also known as CPAP flow, C flow, or machine flow), which varies with inspiration and expiration, and (2) the leak (bias flow), which is a fairly constant portion due to system leak..")
84
Monitoring during Positive Pressure Titration Total flow = PAP flow + Leak Total flow increases with pressure but is separated into a variable component (CPAP flow) and a more constant component (leak). The leak includes intentional (mask orifice) and unintentional leak. Leak = Intentional leak + Unintentional leak On higher CPAP, the total flow increases as the intentional flow increases (even if unintentional leak does not increase). All CPAP mask interfaces have a built-in orifice system consisting of small holes to provide an intentional leak that washes out exhaled CO2 from the mask and prevents rebreathing.
 and unintentional leak. Leak = Intentional leak + Unintentional leak On higher CPAP, the total flow increases as the intentional flow increases (even if unintentional leak does not increase). All CPAP mask interfaces have a built-in orifice system consisting of small holes to provide an intentional leak that washes out exhaled CO2 from the mask and prevents rebreathing..")
86
Monitoring during Positive Pressure Titration This intentional leak increases with the amount of pressure and varies between different masks. The unintentional leak is due to mask or mouth leak (in the case of a nasal mask). Leak is seen by the machine as bias or constant baseline inspiratory flow onto which the variations in patient flow is superimposed. The leak signal provided by some devices is the total leak whereas others provide an estimate of unintentional leak by subtracting the expected leak given the mask and pressure (mask type must be specified). Absolute values are less useful than relative increases in leak.
. Leak is seen by the machine as bias or constant baseline inspiratory flow onto which the variations in patient flow is superimposed. The leak signal provided by some devices is the total leak whereas others provide an estimate of unintentional leak by subtracting the expected leak given the mask and pressure (mask type must be specified). Absolute values are less useful than relative increases in leak..")
87
Intentional leak increases with pressure and depends on the mask type (A, B, or C). Information is available with each mask.

89
Monitoring during Positive Pressure Titration The PAP flow signal provides not only an estimate of the magnitude of flow but also information from the inspiratory flow contour. High upper airway resistance is manifested by a flattened profile.The normal profile is a rounded one. Snoring can be detected by a snoring sensor placed on the neck or from pressure vibrations in mask pressure. Nearly all sleep center PAP units will also provide a signal of the “machine pressure.” This is the pressure at the machine outlet and can differ slightly from the set pressure (value entered by technologist). Mask pressure may be somewhat lower during inhalation and sometimes slightly higher during exhalation. Mask pressure can also be directly measured by connecting the mask to a pressure transducer.
. Mask pressure may be somewhat lower during inhalation and sometimes slightly higher during exhalation. Mask pressure can also be directly measured by connecting the mask to a pressure transducer..")
90
A drop in CPAP; arrow, results in change of flow signal (becoming flattened consistent with airflow limitation )and increased pressure gradient across the upper airway (increased resistance).
and increased pressure gradient across the upper airway (increased resistance).")
91
Flattening in the CPAP flow signal (arrow) suggests high upper airway resistance, and this is consistent with the appearance of snoring. After only 1 cm H2O increase in pressure, the CPAP flow signal is now round and the snoring has stopped.

92
Monitoring during Positive Pressure Titration Recording of the leak signal is useful for the physician reviewing a PAP titration. The trend in the leak is more useful than the absolute number. If the patient has not moved and leak suddenly increases, this could be a hint that mouth leak is occurring (assuming the patient is wearing a nasal mask). Sometimes, an increase in leak can occur with the onset of REM sleep. Relaxation in the facial musculature can sometimes produce mask or mouth leaks.
. Sometimes, an increase in leak can occur with the onset of REM sleep. Relaxation in the facial musculature can sometimes produce mask or mouth leaks..")
93
The patient was wearing a nasal mask and chin strap. At the transition to stage R, a large increase in leak was noted. Note that the increase in leak signal lags behind the obvious change in flow that occurs a few seconds earlier. If the flow

94
Monitoring during Positive Pressure Titration If the flow signal becomes truncated during expiration, this means that part or all of flow during exhalation is not sensed by the machine flow sensor (no flow returning to the hose / device system) consistent with an expiratory leak from either the mask or the mouth. If the patient is wearing a nasal mask (which has not moved), the sudden appearance of truncated expiratory flow (often associated with vibration in the snoring sensor) is suggestive of expiratory mouth leak. The technician does not necessarily have to intervene unless mouth leak is arousing the patient or preventing PAP from maintaining a patent airway. If mouth leak is a problem, either using a chin strap or an oro-nasal mask or lowering the pressure could be considered.
, the sudden appearance of truncated expiratory flow (often associated with vibration in the snoring sensor) is suggestive of expiratory mouth leak. The technician does not necessarily have to intervene unless mouth leak is arousing the patient or preventing PAP from maintaining a patent airway. If mouth leak is a problem, either using a chin strap or an oro-nasal mask or lowering the pressure could be considered..")
95
A change in expiratory flow combined with expiratory snoring is suggestive of an expiratory leak. Compare the truncated expiratory flow in epoch 602 with the normal expiratory flow in epoch 600. This is due to expiratory mask or mouth leak (if a nasal mask is being used).
..")
96
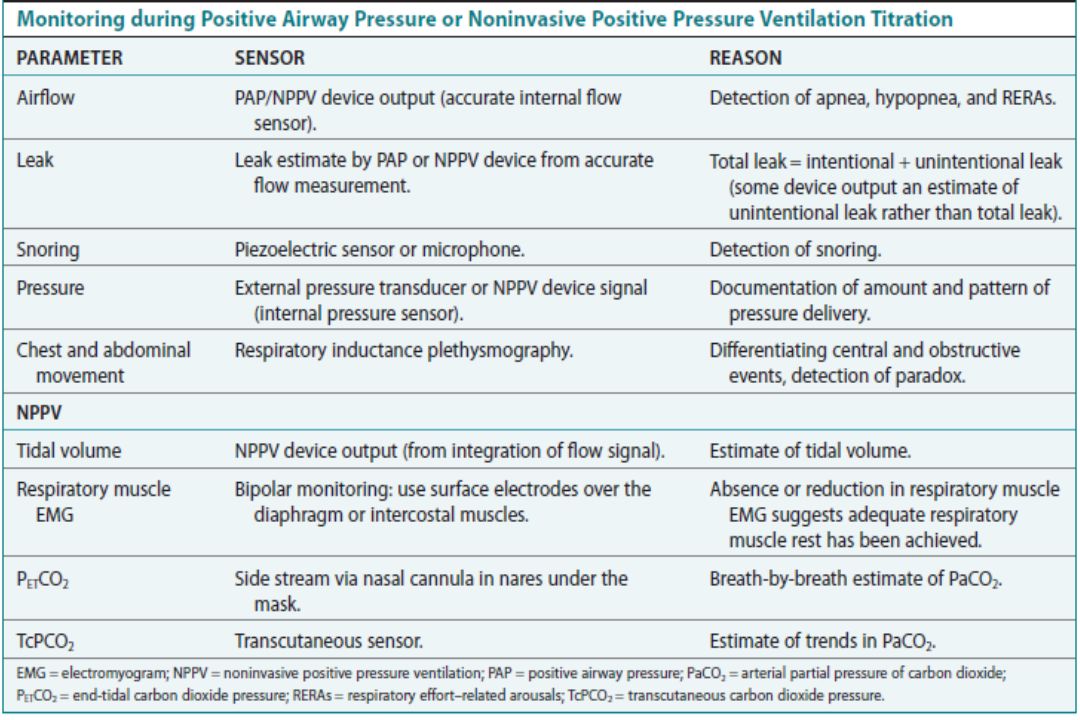
Additional Monitoring for NPPV Titration For NPPV titration, it is useful to record the tidal volume signal from the PAP device that is derived from integration of the flow signal. Tidal volume depends both on flow and inspiratory time. Therefore, monitoring the flow signal alone may not provide an accurate estimate of ventilation.

97
Patient is breathing on BPAP spontaneous timed (ST) mode with a backup rate of 12 breaths/min. Breaths A and C are patient initiated and breaths B and D are machine-cycled breaths. The tidal volume differs between breaths A, B and C,D due to a different IPAP time.

98
Additional Monitoring for NPPV Titration Some sleep centers that perform NPPV in patients with neuromuscular disorders also record an intercostals electromyogram (EMG) or surface diaphragmatic EMG with techniques similar to those for leg EMG. If the signal decreases, tidal volume increases and respiratory rate decreases; these changes suggest that adequate respiratory muscle rest is being delivered by the current level of PS.

99
When the level of pressure support was increased, there was a decrease in the respiratory rate and in the intercostal electromyogram (EMG)
")
100
Additional Monitoring for NPPV Titration Some sleep centers record either the end-tidal partial carbon dioxide pressure (PETCO2) or trans-cutaneous carbon dioxide pressure (TcPCO2). A PETCO2 tracing should show a plateau. The exhaled gas sampled for the PETCO2 measurement can be diluted by NPPV flow. A common method is to use a small nasal cannula under the mask that suctions exhaled air at the nares before it can be diluted. A downside is that this can cause problems with the mask seal. Another option is to record is the TcPCO2. These surrogate measures of PCO2 are useful only if calibrated and validated (ideally with an arterial or capillary blood gas).
..")
101
The CO2 tracing is delayed relative to exhaled airflow in the side stream method.

102
Note the simultaneous increase in transcutaneous PCO2 and the decrease in SpO2 during episodes of rapid eye movement (REM) sleep.
 sleep.")
103
ACCURACY OF PETCO2 AND TcPCO2 The measurement of PETCO2 and TcPCO2 was not found to be accurate for determining changes in PaCO2 during sleep. PETCO2 was especially inaccurate during simultaneous administration of supplemental oxygen or during positive airway pressure treatment. Of note, exhaled gas was sampled from a mask rather than using a nasal cannula. PETCO2 or TcPCO2 may be acceptable if validated and calibrated. In the pediatric rules, it states that “acceptable methods for assessing alveolar hypoventilation are either transcutaneous or end-tidal PCO2 monitoring.” Of course, the goal standard to validate the accuracy of their measurements is a simultaneous ABG measurement.

104
Titration for CPAP Therapy Set mode to CPAP Initial pressure: 4–5 cm H2O

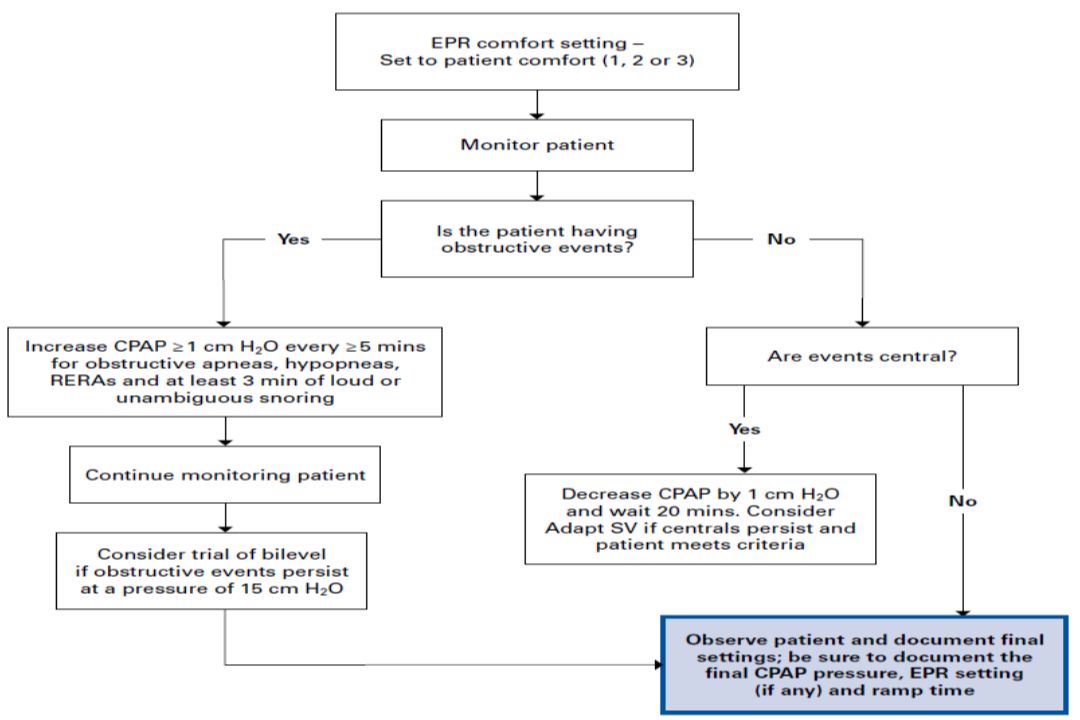
106
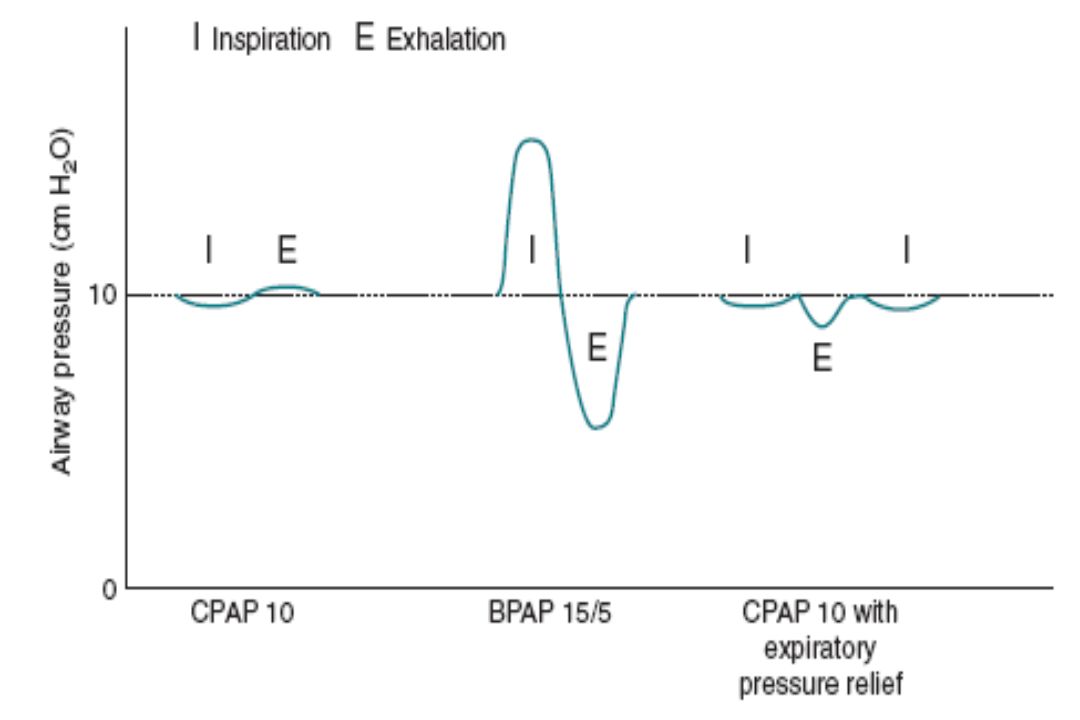
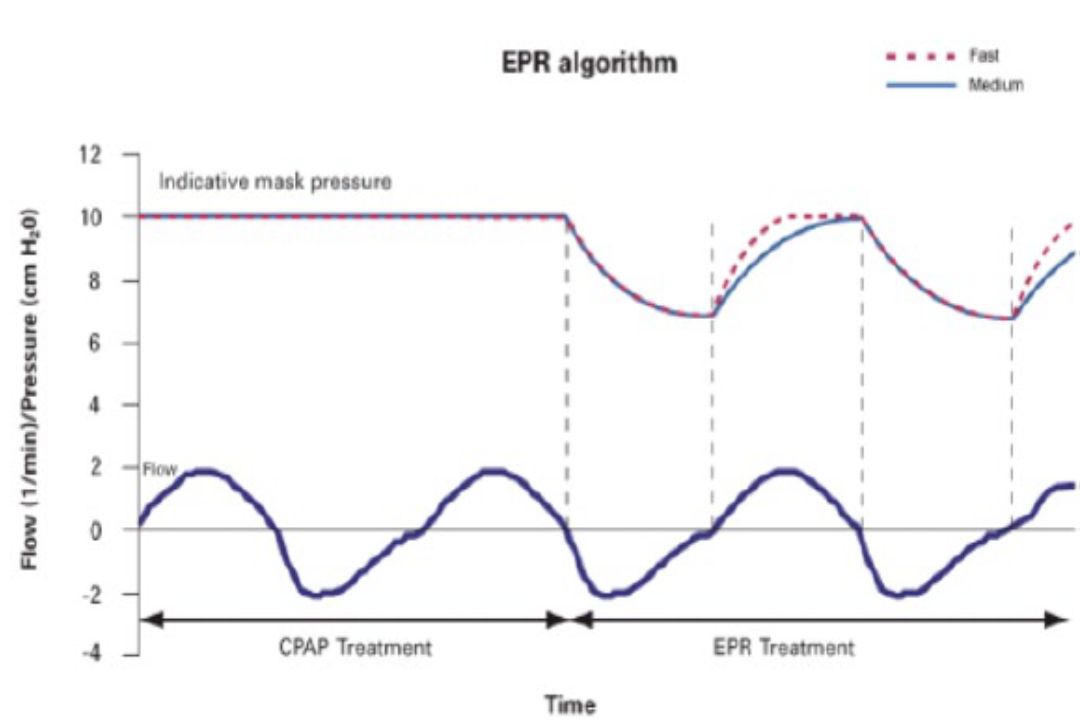
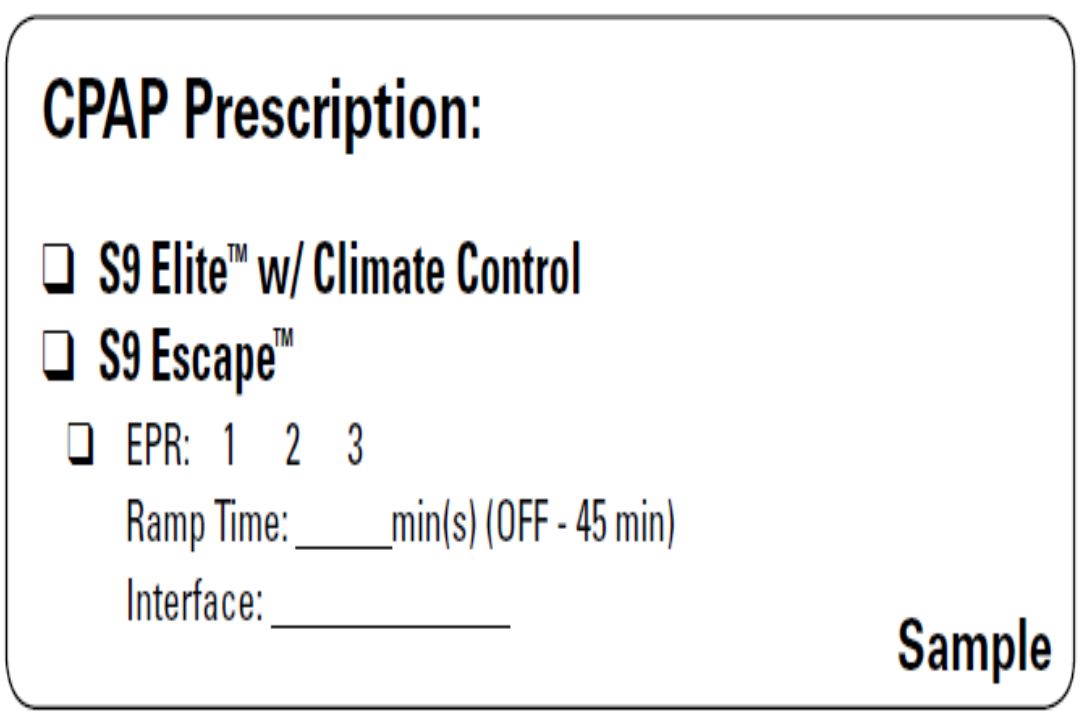
EPR™ and Easy-Breathe (CPAP and AutoSet™) EPR is designed to maintain optimal treatment for the patient during inhalation and reduce the delivered mask pressure during exhalation in the CPAP or AutoSet mode. The desired result of EPR is to decrease the pressure the patient must breathe out against, making the overall therapy more comfortable. EPR LEVEL of OFF, 1, 2, or 3 cm H2O can be selected. In CPAP mode, the EPR INHALE can be set to medium or fast. The delivered pressure will not drop below a minimum pressure of 4 cm H2O, regardless of the settings.

109
Pressure-intolerant patients If the patient awakens and complains of excessive pressure, pressure should be lowered. If this does not work, use of flexible PAP or a switch from CPAP to BPAP may be tried. When switching from CPAP to BPAP, one approach is to use IPAP 2 cm H2O higher than CPAP and EPAP 2 cm H2O lower. Another approach is to use EPAP = CPAP, and IPAP = EPAP + 4 cm H2O and titrate pressure upward if needed.

110
Pressure-intolerant patients In pressure-intolerant patients, sleep in the lateral position or with the head elevated can be tried to reduce the required level of pressure. If mouth leak is a problem, a chin strap can be tried followed by an oro-nasal mask. If there is excessive mask leak, a readjustment of the mask, change in mask size, or change in mask type is indicated. Over tightening of the mask straps is strongly discouraged. In patients with allergic rhinitis or nasal congestion, use of heated humidification from the start of the study is suggested.

113
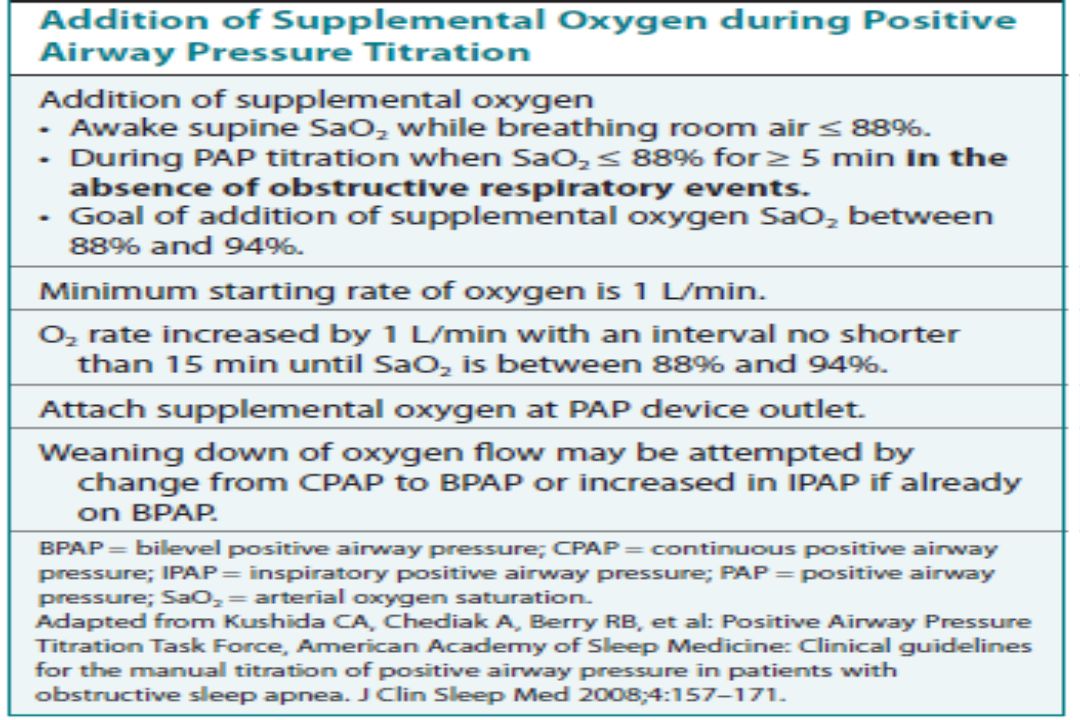
PAP and Supplemental Oxygen Some patients will exhibit significant arterial oxygen desaturation despite adequate airflow, especially during REM sleep. Persistent hypoxemia in these conditions may be due to hypoventilation or ventilation-perfusion mismatch (often due to chronic lung disease). In some studies of titration in patients with OHS, a substantial number of patients required the addition of supplemental oxygen. If the awake supine patient has an SaO2 of 88% or lower or is already on supplemental oxygen to maintain an acceptable awake SaO2, the addition of supplemental oxygen will definitely be needed. Before adding supplemental oxygen, one can attempt to adjust the PAP pressure settings to prevent the need for this additional treatment.
. In some studies of titration in patients with OHS, a substantial number of patients required the addition of supplemental oxygen. If the awake supine patient has an SaO2 of 88% or lower or is already on supplemental oxygen to maintain an acceptable awake SaO2, the addition of supplemental oxygen will definitely be needed. Before adding supplemental oxygen, one can attempt to adjust the PAP pressure settings to prevent the need for this additional treatment..")
114
PAP and Supplemental Oxygen If the patient is requiring high oxygen flows, optimizing PAP may allow reduction in the required oxygen flow rate. First, an increase in CPAP can be tried to eliminate unrecognized high upper airway resistance. If this is not successful or not tolerated, CPAP can be changed to BPAP. If the patient is already on BPAP, the level of PS can be increased. If these interventions do not increase the SaO2 to an acceptable level or if higher pressure is not tolerated, supplemental oxygen can be added to PAP. with a goal of attaining an acceptable SaO2 (88–94%). Most clinicians would use a target 92% to 94% to allow for variability and a margin of safety.
. Most clinicians would use a target 92% to 94% to allow for variability and a margin of safety..")
117
PAP and Supplemental Oxygen It is important to recognize that the effective oxygen concentration will depend on both the supplemental oxygen flow (L/min) and the machine flow. Increases in machine flow associated with higher pressure or mask /mouth leak can dilute a given flow of supplemental oxygen. For example, if a patient with chronic lung disease requires supplemental oxygen at 2 L/min to maintain an SaO2 of 94% while awake without CPAP, on CPAP the required supplemental oxygen flow will likely be much higher (assuming the same fractional concentration of oxygen on CPAP treatment is still required).
..")
118
Approximate change in effective fractional concentration of oxygen in inspired gas (FiO2) with supplemental oxygen and various CPAP levels in a model system
 with supplemental oxygen and various CPAP levels in a model system")
119
Complex Sleep Apnea

120
Complex Sleep Apnea (Comp SA) is defined as a form of central apnea specifically identified by the persistence or emergence of central apneas or hypopneas upon exposure to CPAP or a BPAP without a backup rate when obstructive events have disappeared. Patient with CompSA have predominantly obstructive or mixed apneas during the diagnostic sleep study (or diagnostic portion of a split study) occurring at 5/hr or greater. The CMS definition of Comp SA requires that 1- Greater than 50% of the residual respiratory events on PAP are central apneas or central hypopneas, 2- The central AHI is 5/hr or greater, and 3- The total AHI is 5 or greater.
 occurring at 5/hr or greater. The CMS definition of Comp SA requires that 1- Greater than 50% of the residual respiratory events on PAP are central apneas or central hypopneas, 2- The central AHI is 5/hr or greater, and 3- The total AHI is 5 or greater..")
121
Complex Sleep Apnea Patients with a combination of OSA and Chyne- Stokes breathing (CSB)may manifest CSB-central apneas when CPAP eliminates obstructive events. These patients meet the definition of Comp SA. Patients taking potent opiates develop central apneas on CPAP (treatment emergent central apneas) or central apneas persist on CPAP. Other patients may manifest CompSA without an obvious cause (idiopathic CompSA). Patients with Cheyne-Stokes central apnea or idiopathic CompSA tend to have high ventilatory drives or difficulty maintaining sleep. Central apnea occurs because the PaCO2 drops below the apneic threshold.
 or central apneas persist on CPAP. Other patients may manifest CompSA without an obvious cause (idiopathic CompSA). Patients with Cheyne-Stokes central apnea or idiopathic CompSA tend to have high ventilatory drives or difficulty maintaining sleep. Central apnea occurs because the PaCO2 drops below the apneic threshold..")
122
The approach to CompSA and PAP titration protocol for handling central apneas varies between sleep centers. One approach is to increase CPAP only until the obstructive apneas and hypopneas are eliminated. CPAP is increased further only if RERAs are believed to be causing central apneas (after the arousals). Many patients will stabilize if they enter stage N3 sleep (i.e., patience rather than increasing the CPAP). A small reduction in pressure to one not associated with central apneas can also be tried. Some patients will also improve in the lateral sleeping position. NB :Switching from CPAP to BPAP without a backup rate is NOT indicated and may actually contribute to ventilatory instability.
. Many patients will stabilize if they enter stage N3 sleep (i.e., patience rather than increasing the CPAP). A small reduction in pressure to one not associated with central apneas can also be tried. Some patients will also improve in the lateral sleeping position. NB :Switching from CPAP to BPAP without a backup rate is NOT indicated and may actually contribute to ventilatory instability..")
123
The approach to CompSA and PAP titration protocol for handling central apneas varies between sleep centers. Many patients with Comp SA when treated with CPAP on a chronic basis will have a resolution of the central apneas. Others with CSB or narcotics as a cause for ventilatory instability may continue to have frequent central events on chronic CPAP treatment. These patients should undergo another PAP titration with ASV or BPAP with a backup rate. It is better to utilize an entire night to perform an ASV titration

124
ASV Titration Protocol For the Adapt SV, EPAP = 4 cm H2O, PS max of 10 cm H2O or greater, PS min of 3 cm H2O. EPAP should be increased slowly to allow the patency of upper airway. For the BiPAP auto SV advanced, recommended settings are EPAP min = 4 cm H2O, EPAP max = 15 cm H2O, PS min = 0 cm H2O, PS max = 20 cm H2O, Max pressure = 25 cm H2O, rate = auto. If it is known that CPAP greater than 10 cm H2O is needed to prevent obstructive apnea, EPAP min of 6 to 8 cm H2O could be tried. For those with a component of hypoventilation (narcotics), PS min of 4 cm H2O could be used. Most insurance providers have definite criteria for reimbursement for ASV or BPAP with a backup rate Usually more than 50% of the events on CPAP must be either central apneas or central hypopneas.
, PS min of 4 cm H2O could be used. Most insurance providers have definite criteria for reimbursement for ASV or BPAP with a backup rate Usually more than 50% of the events on CPAP must be either central apneas or central hypopneas..")
125
ASV Titration Protocol Servo-ventilation made by different manufacturers can successfully detect and treat central apneas. During servo-ventilation, the expiratory positive airway pressure is set at a level to treat obstructive apneas and obstructive hypopneas. Combining APAP and servo-ventilation, with APAP determining the EPAP level automatically, whereas the servo-ventilation controlling periodic breathing and central apneas has been recently reported to be effective in ameliorating SRBD.

126
SomnoVent CR Respironics autoSV ResMed VPAP Adapt SVRespironics autoSVResMed VPAP Adapt SV

127
Score a hypopnea as obstructive if ANY of the following criteria are met: 1. Snoring during the event 2. Increased inspiratory flattening of the nasal pressure or PAP device flow signal compared to baseline breathing 3. Associated thoracoabdominal paradox occurs during the event but not during pre-event breathing. Score a hypopnea as central if NONE of the following criteria are met: 1. Snoring during the event 2. Increased inspiratory flattening of the nasal pressure or PAP device flow signal compared to baseline breathing 3. Associated thoraco-abdominal paradox occurs during the event but not during pre-event breathing.

129
Adequacy of PAP Titration 1)An optimal titration is one that reduces the AHI to less than 5/hr for at least 15 minutes and should include supine REM sleep at the final pressure without repeated arousals. 2) A good titration results in an AHI < 10/hr or at least a 50% reduction in the AHI if the baseline AHI is less than 15/hr. A good titration should include supine REM sleep at the selected pressure that is not continually interrupted by arousals. 3) An adequate titration is one that does not reduce the AHI < 10/hr but does reduce the AHI by 75% from baseline, or one in which criteria for optimal or good titration is met with the exception that supine REM sleep did not occur at the selected pressure.
 A good titration results in an AHI < 10/hr or at least a 50% reduction in the AHI if the baseline AHI is less than 15/hr. A good titration should include supine REM sleep at the selected pressure that is not continually interrupted by arousals. 3) An adequate titration is one that does not reduce the AHI < 10/hr but does reduce the AHI by 75% from baseline, or one in which criteria for optimal or good titration is met with the exception that supine REM sleep did not occur at the selected pressure..")
130
Adequacy of PAP Titration 4) An unacceptable titration does not meet any of these criteria. A repeat titration should be ordered. In optimal, good, and acceptable titrations, the SaO2 should remain above 90% at the treatment pressure selected for chronic use. If a titration shows borderline oxygenation, it is then prudent to check nocturnal oximetry while the patient uses PAP at home.

132
A portion of overnight oximeter of patient with both snoring and COPD. The baseline is reduced during sleep but the saw-tooth patteren is suggestive of obstructive sleep apnea A = Period of REM sleep.

133
ALTERNATIVE METHODS OF STARTING PAP TREATMENT

134
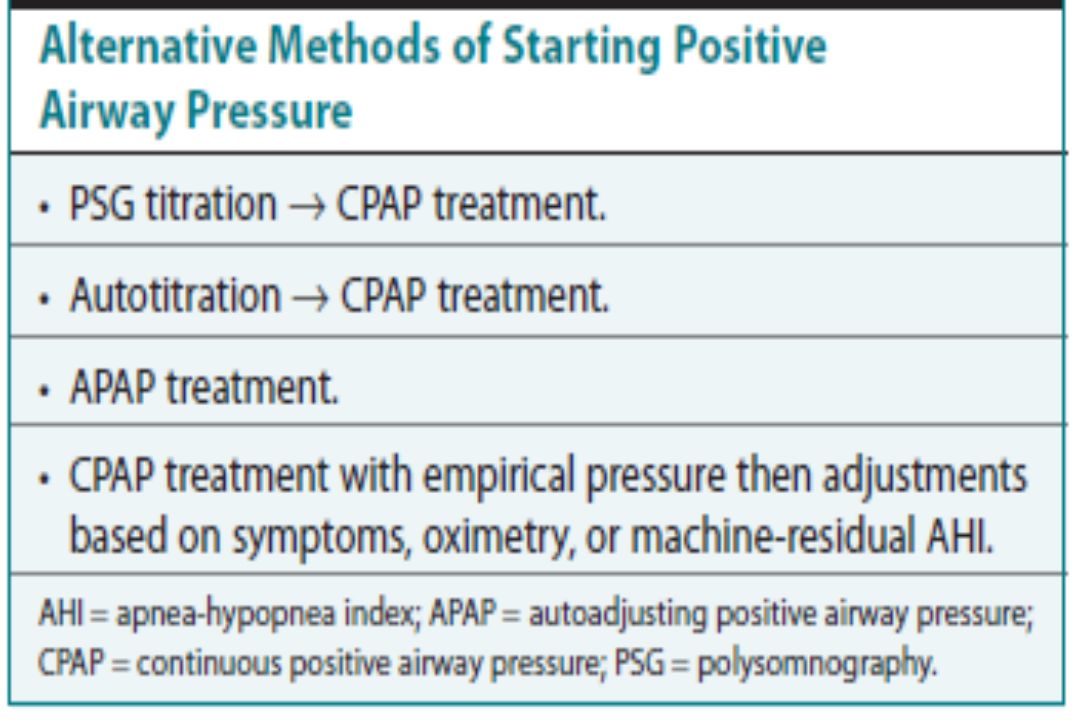
The titration alternatives can be used for patients who are unwilling or unable to have a standard PSG titration. These alternatives include Treating the patient with an APAP device (titration not needed) Performing autotitration at home for several days to a week (at least 3 days optimum) with subsequent CPAP treatment based on the results, and Starting PAP treatment based on a prediction equation with subsequent adjustment based on symptoms, machine readings, and nocturnal oximetry.
 Performing autotitration at home for several days to a week (at least 3 days optimum) with subsequent CPAP treatment based on the results, and Starting PAP treatment based on a prediction equation with subsequent adjustment based on symptoms, machine readings, and nocturnal oximetry..")
136
ALTERNATIVE METHODS OF STARTING PAP TREATMENT The prediction equation can provide an empirical treatment level or a reasonable starting point for a PAP titration. The optimal treatment pressure may differ substantially from the predicted pressure. The formula considerably underestimates the required pressure, especially in men. CPAP predicted =0.16XBMI +0.13 X NC + 0.04 XAHI – 5.12 where BMI = body mass index and NC = neck circumference in centimeters.

137
ALTERNATIVE METHODS OF STARTING PAP TREATMENT Most PAP devices provide an estimate of the residual AHI. Some devices also separate apneas into “clear airway apneas” and “obstructive apneas.”. Comparing standard PSG titration, autotitration for one night followed by CPAP treatment based on the results, and CPAP based on a prediction formula with subsequent adjustments based on symptoms and at the end of a 12-week period, all patients were studied on their current CPAP pressure. All three methods resulted in equivalent CPAP adherence, control of the AHI, and improvement in subjective sleepiness.

138
Patient Selection for Alternative Titrations Patients with a number of conditions are not suitable for APAP titration or treatment. These include 1-patients who require or are likely to require supplemental oxygen (low baseline SaO2) 2-patients with hypoventilation 3-patients likely to have central apneas (narcotics, congestive heart failure), and 4-patients who may require very high pressures. Patients with severe pressure intolerance or moderate to severe COPD who may require BPAP should also undergo a PSG titration if possible.
 2-patients with hypoventilation 3-patients likely to have central apneas (narcotics, congestive heart failure), and 4-patients who may require very high pressures. Patients with severe pressure intolerance or moderate to severe COPD who may require BPAP should also undergo a PSG titration if possible..")
139
Technique of Autotitration The patient is educated about OSA and PAP treatment and has mask fitting and instructions on use of an APAP device. It is often useful for the patient to take a brief practice nap during which she or he applies the interface, activates the APAP device, and “naps” for about 15 or 20 minutes. The patient then sleeps on the APAP device at home for several nights. Usually, the pressure limits of the device are set from 4 to 20 cm H2O. In large patients likely to require high CPAP, starting with pressure of 4 cm H2O may be uncomfortable, so a higher low-pressure limit is chosen (8–10 cm H2O). For the pressure-intolerant patient, a lower upper limit of pressure can be chosen. A telephone hotline is available for interventions.
. For the pressure-intolerant patient, a lower upper limit of pressure can be chosen. A telephone hotline is available for interventions..")
140
Technique of Autotitration The device is then returned and the information transferred to a computer. The quality of the autotitration can be noted including amount of use (adherence), residual AHI, and amount of leak. Either the 95th percentile pressure or the 90th percentile pressure (depending on device) is chosen for chronic PAP treatment. If the APAP titration is suboptimal owing to poor adherence, high leak, or high residual AHI, another attempt can be made using a different mask, heated humidfication, or other interventions. If two attempts at an APAP titration are unsuccessful, the patient can be referred for a PSG titration.
, residual AHI, and amount of leak. Either the 95th percentile pressure or the 90th percentile pressure (depending on device) is chosen for chronic PAP treatment. If the APAP titration is suboptimal owing to poor adherence, high leak, or high residual AHI, another attempt can be made using a different mask, heated humidfication, or other interventions. If two attempts at an APAP titration are unsuccessful, the patient can be referred for a PSG titration..")
142
Follow-up of Patients on PAP Treatment Because the pattern of adherence is set early, obtaining a download within the first week and having a face-to-face visit at or soon after 4 weeks of use is recommended. CMS rules require at least 1 month of 70% of nights with greater than 4 hours of use. This month of adherence must occur within the first 3 months of CPAP use for treatment to continue to be reimbursed. Most PAP machines give information on leak and residual AHI. Some can give detailed information about residual events including clear airway events (central apneas).
..")
143
High proportion of patients “well treated” with CPAP who had elevated AHI values on their current treatment pressures. A high residual AHI found on CPAP machine download would suggest that 1- the current pressure was inadequate (unless the events were central apneas) or 2- that an inadequate mask seal significantly reduced the delivered pressure. Some CPAP and APAP devices present the residual AHI, hypopnea index (HI), and a snoring index. If the residual apnea index exceeds the HI, this is a clue that central apnea may be present. Follow-up of Patients on PAP Treatment
 or 2- that an inadequate mask seal significantly reduced the delivered pressure. Some CPAP and APAP devices present the residual AHI, hypopnea index (HI), and a snoring index. If the residual apnea index exceeds the HI, this is a clue that central apnea may be present. Follow-up of Patients on PAP Treatment.")
144
Recently, CPAP and APAP devices can separate apneas into obstructive apneas and “clear airway apneas.” A high residual AHI in a patient with congestive heart failure or potent narcotic use would suggest the possibility of central apneas. High leak would suggest need for better interface fit. The interface could be adjusted or changed to a different size or interface type. If extreme dryness is present and a reasonable humidity must be prescribed.

145
CA = clear airway apnea; FL = flow limitation; H = hypopnea; OA = obstructive airway apnea; PB = periodic breathing; RE = respiratory effort–related arousal; VS = vibratory snore.

146
NPPV Titration and Treatment The titration of NPPV focuses on providing ventilator support in addition to maintaining an open airway. Patients with neuromuscular disorders, thoracic cage disorders, or disorders of inadequate ventilatory control may not be obese and may not require as high an EPAP as patients with OSA or OHS. IPAP and EPAP are titrated as per the protocol discussed previously to eliminate obstructive events. However, the goal is to provide adequate PS without using excessive pressure. Therefore, BPAP of 16/4 or 20/5 cm H2O might be typical pressures.

147
NPPV Titration and Treatment The ST mode is used for treatment of all patients with central ventilatory control disorders and is also recommended for patients with neuromuscular disorders and thoracic cage disorders. These patients may not reliably cycle the BPAP device from EPAP to IPAP. The ST mode is also needed if central apneas are noted during the NPPV titration. The backup rate is usually set 1 to 2 breaths below the sleeping spontaneous breathing rate (8–10 breaths/min minimum). The Ti is chosen between 30% and 40% of the cycle time, this is also known as the % IPAP time.
. The Ti is chosen between 30% and 40% of the cycle time, this is also known as the % IPAP time..")
148
NPPV Titration and Treatment In general, patients with airflow obstruction (COPD) are best treated with 30% %IPAP time and those with restrictive disorders may do better with 40% %IPAP time. One manufacturer recommends using 1.5 seconds as the default inspiratory time for BPAP-ST. The rise time is the time from start of the IPAP cycle until IPAP pressure is reached. It is typically around 200 msec (200–600 msec) but can be varied for patient comfort.
 but can be varied for patient comfort..")
149
Rise time

151
Goals of NPPV Titration and Treatment 1- Improving sleep quality and preventing nocturnal dyspnea, 2- Preventing nocturnal hypoventilation (or worsening of hypoventilation during sleep if daytime hypoventilation is present), and 3- Providing respiratory muscle rest. For patients with daytime hypoventilation, use of NPPV can improve the quality of life and delay or prevent the progression of respiratory failure.

152
Goals of NPPV Titration and Treatment The nocturnal PaCO2 goal is a value equal to or less than the daytime PaCO2. However, sufficient PS may not be tolerated initially. NPPV can be started on an outpatient basis at low pressure (BPAP 8/4) and increased as tolerated based on patient symptoms and oximetry, daytime PETCO2 measurements, or daytime arterial blood gas measurements. NPPV PSG titration is recommended and allows a treatment to be chosen (IPAP, EPAP, backup rate) that will eliminate obstructive apnea/hypopnea and deliver optimal PS. Some patients will also require the addition of supplemental oxygen.
 and increased as tolerated based on patient symptoms and oximetry, daytime PETCO2 measurements, or daytime arterial blood gas measurements. NPPV PSG titration is recommended and allows a treatment to be chosen (IPAP, EPAP, backup rate) that will eliminate obstructive apnea/hypopnea and deliver optimal PS. Some patients will also require the addition of supplemental oxygen..")
153
Goals of NPPV Titration and Treatment Close follow-up is needed because the given level of pressure support may prove inadequate if respiratory muscles weaken. Titration using VT-BPAP (BiPAP AVAPS) is performed to determine an effective EPAP. The ST mode is commonly used. The device will automatically adjust PS to provide a desired tidal volume. If pressure intolerance is a problem, a lower tidal volume target with a higher respiratory rate (spontaneous or machine-triggered) may be better tolerated.
 is performed to determine an effective EPAP. The ST mode is commonly used. The device will automatically adjust PS to provide a desired tidal volume. If pressure intolerance is a problem, a lower tidal volume target with a higher respiratory rate (spontaneous or machine-triggered) may be better tolerated..")
154
AVAPS averages Vt and changes PS value gradually. This occurs over several minutes. The rate of change is slow, so the patient is not aware of breath to breath change.

Similar presentations


























>")


