Download presentation
Presentation is loading. Please wait.

1
2015 Maryland Activity Coordinators Society Conference

2
Today’s Agenda O Review the Federal Regulations O (F248) §483.15(f)(1), O (F249) §483.15(f)(2) O Look at the Stage 2 Critical Element Pathway for QIS surveying of activities programming O Examples of citations issued for non-compliance O Discuss key industry changes, challenges, and future considerations
 §483.15(f)(1), O (F249) §483.15(f)(2) O Look at the Stage 2 Critical Element Pathway for QIS surveying of activities programming O Examples of citations issued for non-compliance O Discuss key industry changes, challenges, and future considerations")
3
Federal Regulations O F248 Activities O Regulatory Text O Interpretive Guidelines O Investigative Protocol O Determination of Compliance O Deficiency Categorization O F249 Activities Director O Regulatory Text O Interpretive Guidelines O Determination of Compliance O Deficiency Categorization

4
Regulatory Language Activities F248 (f) Activities (1) The facility must provide for an ongoing program of activities designed to meet, in accordance with the comprehensive assessment, the interests and the physical, mental, and psychosocial well-being of each resident.
 Activities (1) The facility must provide for an ongoing program of activities designed to meet, in accordance with the comprehensive assessment, the interests and the physical, mental, and psychosocial well-being of each resident.")
5
Activities Interpretive Guidelines

6
Interpretive Guidelines Intent O The facility identifies each resident’s interests and needs; and O The facility involves the resident in an ongoing program of activities that is designed to appeal to his or her interests and to enhance the resident’s highest practicable physical, mental, and psychosocial well-being.

7
Interpretive Guidelines Overview O The activities program for a resident is based on the resident’s comprehensive assessment O Residents’ views on activities O Relevant and valuable to their quality of life and considered part of their dignity, O Activities need to amount to something and be meaningful to the residents’ lives, O Residents with dementia are happier and less agitated in homes with many planned activities for them.

8
Interpretive Guidelines Overview O Alternative Approaches to Activities – activities can look very different in a non- traditional facility that is changing it’s culture to be more like a home. Activities there can look more like daily life for people in their own homes.

9
Interpretive Guidelines Assessment O Information gathered is used to develop the activities component of the comprehensive care plan Questions asked are: O What are the resident’s life long interests? O What does the resident prefer? O Are adaptations needed?

10
Interpretive Guidelines Care Planning O Information from the individualized assessment is used to develop the activities component of the comprehensive care plan O Objectives should be measurable and should focus on the resident’s desired outcomes O All relevant departments collaborate—not just activities department O Remember– Activities can occur at any time, not just during formal activities provided by activities staff

11
Interpretive Guidelines Care Planning O Facilities need to consider accommodations in schedules, supplies, and timing to optimize participation. For example, O Alter therapy or bath schedule O Modify meal schedule O Assist residents in dressing, toileting, and transportation O Provide supplies and adaptive equipment/supplies if needed

12
Interpretive Guidelines Interventions Individualized interventions are based on assessment of each resident’s history, preferences, strengths, and needs. Reality orientation and large group activities that include residents with different levels of strengths and needs are not recommended.

13
Interpretive Guidelines Interventions When evaluating the provision of activities, it is important to identify whether the resident has issues for which staff should have provided adaptations. Types of impairments that might require adaptations include visual, hearing, physical, and cognitive.

14
Interpretive Guidelines Interventions: Addressing Behavioral Symptoms O Facilities should take into account resident’s pattern of behavior symptoms O Activities should be presented prior to when symptoms usually present themselves O WHY? Once a behavior escalates, activities may be less effective or may cause further stress

15
Interpretive Guidelines Interventions: Addressing Behavioral Symptoms Examples of interventions to address behavioral symptoms include: O Encouraging physical exercise for a resident who is constantly walking O Providing organizing tasks for a resident who goes through other’s belongings O Offering social programs and opportunities for leadership for a resident who is attention seeking

16
Activities Investigative Protocol

17
Investigative Protocol Objectives To determine if: O The facility has provided and ongoing program of activities designed to accommodate the individual resident’s interests and help enhance his/her physical, mental, and psychosocial well-being, according to his/her comprehensive resident assessment.

18
Investigative Protocol Procedure Investigation involves: O Observations O Interviews O Record review O To determine whether the facility is in compliance, use this procedure for each resident sampled

19
Investigative Protocol Procedure: Observations What to look for….. Is the staff: O Taking preferences and needs into account? O Using adaptive equipment? O Providing timely transportation? O Providing activities that are compatible with residents’ interests, needs and abilities?

20
Investigative Protocol Procedure: Interviews O Interviews are an important facet of the investigation of compliance for F248. O Start with the resident (or their representative, if applicable). Their opinion of their activities participation is important for determining if activities are individualized according to the resident’s preferences.
. Their opinion of their activities participation is important for determining if activities are individualized according to the resident’s preferences..")
21
Investigative Protocol Procedure: Interviews Which staff should be interviewed? O Activity Staff O Certified Nursing Aides (CNAs) O Social Services Staff O Nurses
 O Social Services Staff O Nurses.")
22
Investigative Protocol Procedure: Record Review - Assessment O Has the facility found out about the resident’s past life activities choices, preferences, needs for adaptations? What do the records indicate?

23
Investigative Protocol Procedure: Record Review – Care Plan O Review the activities component of the comprehensive care plan to determine if the resident participated in its development and if the plan matches the resident’s interests and goals, and if it specifies who provides needed services. O Determine if the facility periodically reviewed the plan with resident input and made needed changes.

24
Challenges to Meeting Regulatory Requirements O Staffing O Resident mix O Resident behaviors O Training programs O Clinical acuity of residents

25
Activities Determination of Compliance

26
The facility is in compliance if they: O Recognized and assessed for preferences, choices, specific conditions, causes and/or problems, needs and behaviors O Defined and implemented activities in accordance with resident needs and goals O Monitored and evaluated the resident’s response O Revised the approaches as appropriate

27
Determination of Compliance O Compliance must be determined separately for each resident sampled O Activity interventions must be individualized to the resident’s needs and preferences O The facility must have provided necessary adaptations to facilitate the resident’s participation

28
Determination of Compliance Non-compliance might look like: O Facility does not have an activity program or doesn’t offer any activities O A resident with special needs doesn’t receive adaptations needed to participate O Planned activities were not conducted to meet the resident’s care plan O What else might non- compliance look like?

29
Deficiency Categorization Deficiencies at F248 are most likely to have psychosocial outcomes. The survey team should compare their findings to the various levels of severity on the Psychosocial Outcome Severity Guide at Appendix P, Part V.

30
Activities Director Guidance Training (F249) §483.15(f)(2)
 §483.15(f)(2)")
31
What is the purpose of the guidance? The intent is to ensure that the activities program is directed by a qualified professional O What does being qualified entail?

32
Regulatory Language Activities Director The activities program must be directed by a qualified professional who— (i) is a qualified therapeutic recreation specialist or an activities professional who- O (A) is licensed or registered, if applicable, by the State in which practicing; and O (B) is eligible for certification as a therapeutic recreation specialist or an activities professional by a recognized accrediting body on or after October 1990; or
 is a qualified therapeutic recreation specialist or an activities professional who- O (A) is licensed or registered, if applicable, by the State in which practicing; and O (B) is eligible for certification as a therapeutic recreation specialist or an activities professional by a recognized accrediting body on or after October 1990; or")
33
Regulatory Language Activities Director (ii) Has 2 years of experience in a social or recreational program within the last five years, 1 of which was full time in a patient activities program in a health care setting; or (iii) Is a qualified occupational therapist or occupational therapy assistant; or (iv) Has completed a training course approved by the State.
 Has 2 years of experience in a social or recreational program within the last five years, 1 of which was full time in a patient activities program in a health care setting; or (iii) Is a qualified occupational therapist or occupational therapy assistant; or (iv) Has completed a training course approved by the State.")
34
Activities Director Responsibilities O Directing the development, implementation, supervision and ongoing evaluation of the activities program O Completing or delegating the completion of the activities component of the comprehensive assessment O Contributing to, directing or delegating the contribution to the comprehensive care plan goals

35
Activities Director Responsibilities O Directing the activities program also includes: O Scheduling activities O Monitoring the reactions of each resident to care planned activities O Revising interventions as necessary

36
Determination of Compliance The facility is in compliance if they have employed a qualified activity director who: O has developed an activities program that meets the interests of the residents O ensures that the activities component of the comprehensive assessment is completed for every resident and contributes to care plan goals O monitors residents’ responses to interventions and has made necessary changes to care plans and/or to the program offerings

37
Non-compliance for F249 Non-compliance may include: O Lack of a qualified activity director O Lack of direction for planning, scheduling, implementing, monitoring and revising the activity program O Lack of monitoring the response of residents in order to modify care plans as needed

38
Deficiency Categorization O Determine the severity for a deficiency at F249 based on the effect or potential for harm to the resident.

39
Possible Psychosocial Outcomes O Anger O Apathy O Anxiety O Dehumanization O Depressed mood O Humiliation “Reasonable Person Standard” How would a “reasonable person” react if he/she were in the resident’s situation?

40
Severity Determination The key elements for severity determination are: O Presence of harm or potential for negative outcomes O Degree of harm or potential harm related to noncompliance O Immediacy of correction required

41
Severity Levels Level 4: Immediate Jeopardy to resident health or safety Level 3: Actual harm that is not immediate jeopardy Level 2: No actual harm with potential for more than minimal harm that is not immediate jeopardy Level 1: No actual harm with potential for minimal harm

42
Examples of Outcomes Immediate Jeopardy O Examples Of Outcomes To A Deficient Practice: O Suicide attempt, suicidal thoughts, preoccupation, planning (e.g., refusing to eat or drink in order to kill oneself) O Engaging in self-injurious behavior O Sustained & intense crying, moaning screaming O Expression of severe, unrelenting, excruciating pain
 O Engaging in self-injurious behavior O Sustained & intense crying, moaning screaming O Expression of severe, unrelenting, excruciating pain")
43
Examples of Outcomes Actual Harm Examples Of Outcomes To A Deficient Practice: O Significant decline in former social patterns that does not rise to the level of immediate jeopardy O Depressed mood that may be manifested as: O Loss of interest or ability to feel pleasure O Psychomotor agitation accompanied by sadness O Expressions of feelings of worthlessness O Recurrent thoughts of death or statements such as, “I wish I were dead” or “my family would be better off without me”.

44
Examples of Outcomes Actual Harm O Expressions of persistent pain or physical distress that has compromised the resident’s functioning. O Chronic or recurrent anxiety; sleeplessness due to fear. Expression of fear not to level of immobilization as in level 4. O Ongoing expression of humiliation that persists after precipitating event has ceased. O Aggression that could lead to injuring self or others.

45
Examples of Outcomes Potential for Harm Examples Of Outcomes To A Deficient Practice: O Intermittent sadness, as reflected in facial expression, tearfulness. O Feelings or complaints of discomfort or moderate pain; irritability. O Fear or anxiety manifested as signs of minimal discomfort that has the potential to compromise well-being. O Feeling of shame or embarrassment without loss of interest in the environment and self. O Complaints of boredom accompanied by expressions of periodic distress, that do not result in maladaptive behaviors (e.g. verbal or physical aggression). O Verbal or nonverbal expressions of anger that do not lead to harm.
. O Verbal or nonverbal expressions of anger that do not lead to harm..")
46
Severity Level 1 Severity Level 1 is not an option because any facility practice that results in a reduction of psychosocial well-being diminishes the resident’s quality of life. The deficiency is, therefore, at least a Severity Level 2 because it has the potential for more than minimal harm.

47
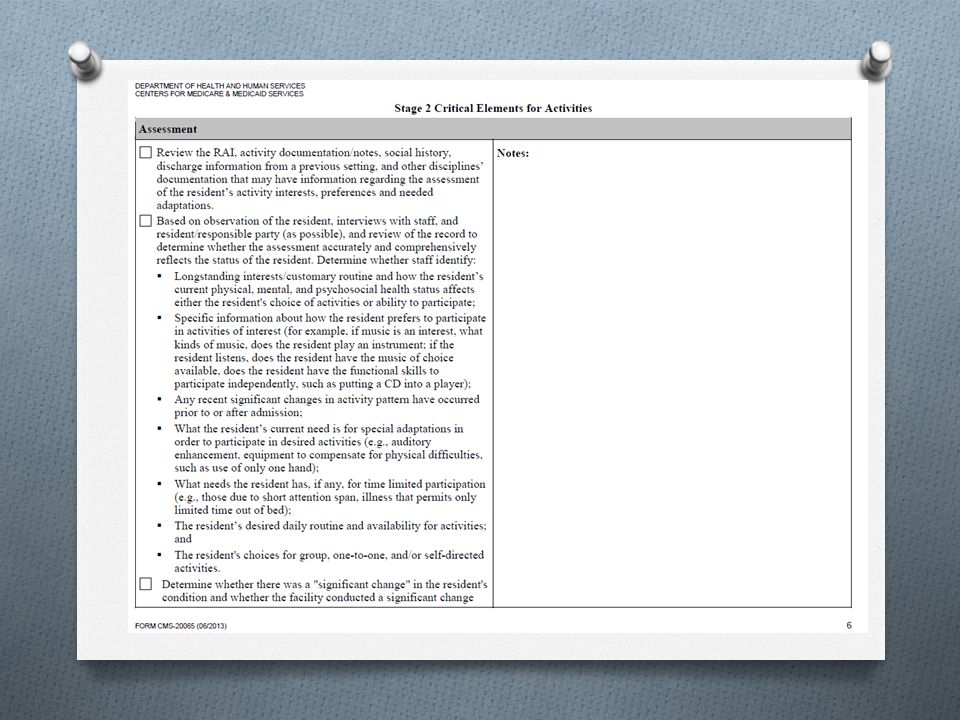
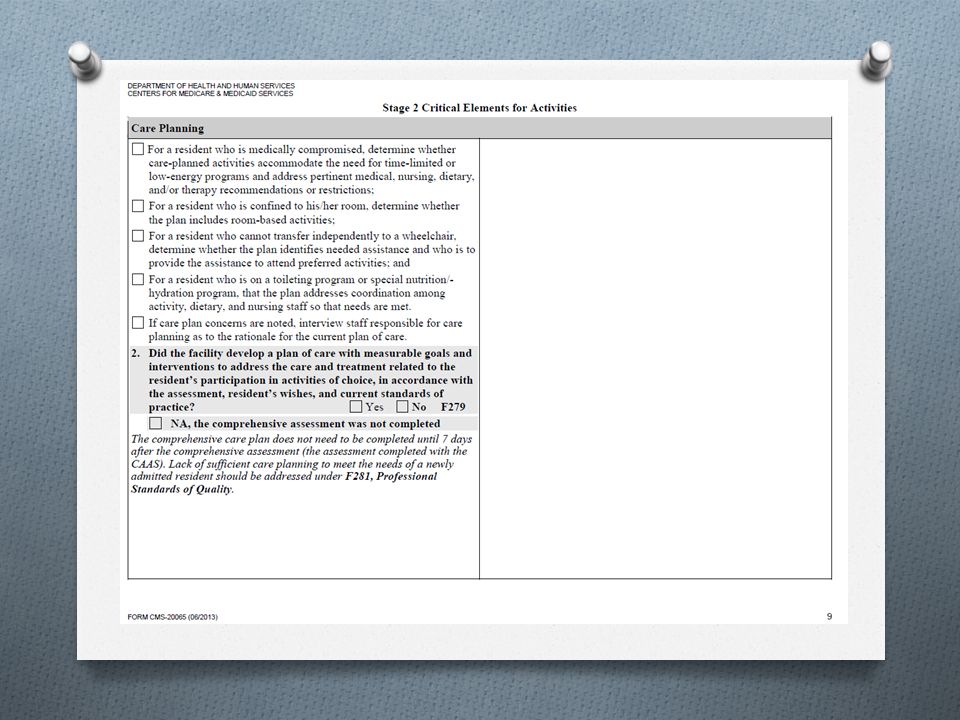
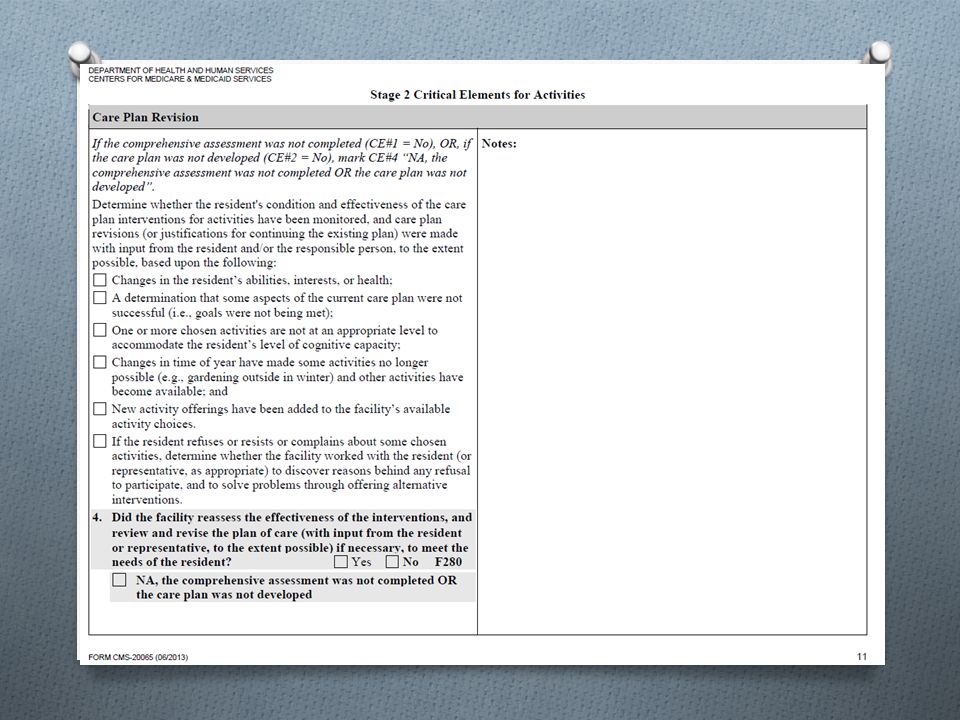
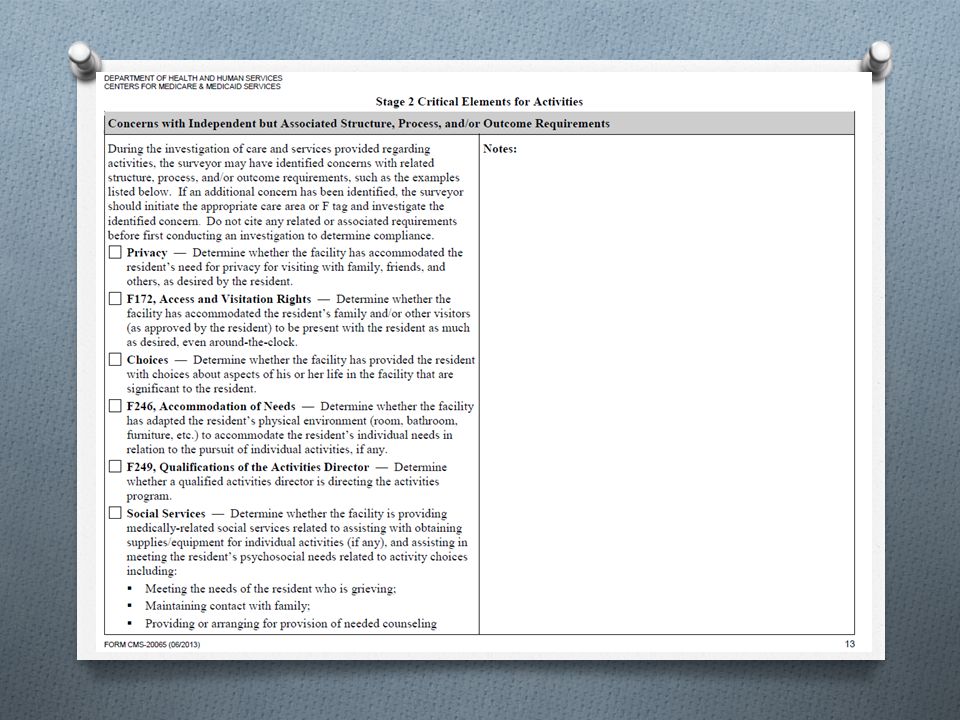
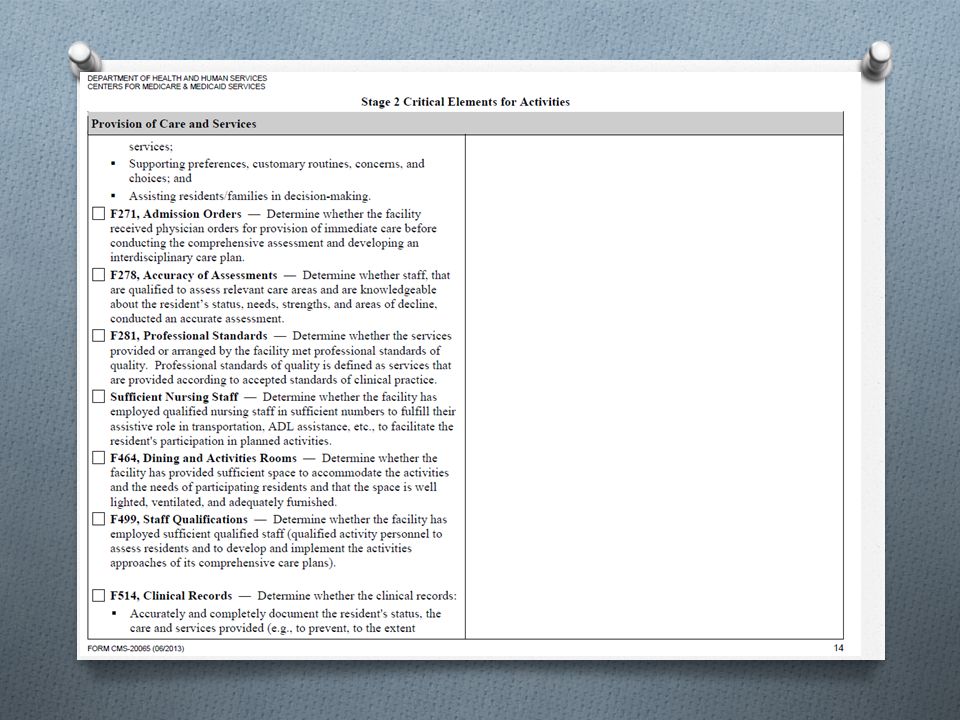
QIS Stage 2 Critical Elements for Activities FORM CMS-20065 (06/2013) Use this protocol for a resident triggered through O Stage 1 resident or family interviews due to a concern with activity participation; O Stage 1 observation of activity participation concerns; O MDS assessment information that the resident spends little or no time in activities.
 Use this protocol for a resident triggered through O Stage 1 resident or family interviews due to a concern with activity participation; O Stage 1 observation of activity participation concerns; O MDS assessment information that the resident spends little or no time in activities.")
63
Real Citations F TAG 248 Citations 2012-June 2015 Total Citations Issued:296 Total Maryland Homes:31 Scope and SeverityNumber of Citations B / Level I1 citation D/Level II89 citations E/Level II57 citations G/Level III1 citation

64
G Level FTAG 248 Facility failed to: O Develop and implement ongoing activity program O Assess / record each resident’s interests O Recognize and address 1 resident’s activity programming needs that resulted in the social isolation for this resident.

65
Other 248 Citation Examples O Resident observed during initial facility tour and at various times throughout the survey to be sleeping or isolated in her room. Activities assessment identified previous likes/hobbies/prior activities but no attempt made during the survey to involve the resident. No documentation to explain.

66
Citation O During survey, several residents sitting in a common area space with the TV on. Residents not engaged with the TV….wandering in / out of the room, some residents agitated. TV was on Russian station. Residents did not appear to understand the program.

67
O 3 residents dependent on staff for mobility and limited ability to communicate. O Observations at various times throughout survey revealed residents in bed or chair in room. No activities programming provided at bedside or in group setting. O Activity care plan stated that “resident will participate in group activities with peers who have like interests to promote socialization.” O MDS marked “little or no activity” Citation

68
O Alert and oriented resident told surveyor that there were not enough planned activities to keep residents busy. O Observation of activities room and common areas daily throughout the survey noted no planned activities occurring. O Observation noted residents sitting in great room with TV playing. No staff person in attendance.

69
O Resident with English as second language. Understands English language but verbally communicates with combination of primary language and English. O Resident activities care plan stated he would be assisted to group activities of his choice. O Observation by surveyor during 4 days of survey noted no attempts from staff to assist resident to group activities. No 1:1 provided. O Telephone interview with daughter notes that staff rarely assist her father to group activities. Citation

70
O Interview with resident noted he enjoyed playing bingo but due to his Parkinson’s Disease, he had difficulty playing b/c hand tremors. O Observed resident sitting back from the table during bingo not actively participating. Falling asleep intermittently. O Interview with the activities aide confirmed that resident loved bingo and stated she “had it covered” O Observation noted another resident playing multiple cards and when interviewed by surveyor stated he was playing cards for the resident who couldn’t play. O Lack of appropriate accommodations to assist residents with participating in activities program. Citation

71
O Activities calendar revealed multiple activities scheduled throughout the day from 10AM through 8PM. O Observation of activities areas noted lack of activities provided according to schedule. O Interview with alert and oriented residents revealed church service scheduled on Sunday mornings never occurs. O Residents also noted that activities schedule cannot be relied upon as true and accurate. O Activities Director stated lack of staffing to follow schedule. Citation

72
O TV set in main dining room broke. O Maintenance removed main TV set for repair. O 3 months later, lack of TV in main dining room. O Residents council requested a replacement TV on 2 separate occasions. O Complaint survey occurred. O Observed no TV in dining room. O Review of residents council meetings noted residents voiced unhappiness several meetings since removal. Citation

73
O Resident with MDS noting significant visual impairment. O Care plan goal notes that resident will have appropriate visual aids to facilitate participation with activities programming of her choice. O Intervention includes, “ensure appropriate visual aids are available to support the residents participation in activities.” Citation

74
Challenges to Meeting Regulatory Requirements O Staffing O Resident mix O Resident behaviors O Training programs O Clinical acuity of residents

75
Key Challenges, Changes, Considerations O CMS’ proposed revisions to Appendix PP O Ever-changing customer expectations O Bundled payment and value based payment initiatives O Declining Medicare and Medicaid reimbursement O Push for HCBS

76
Candace McMullen, RN, NHA, MHA, CLNC VP of Operations/Chief Operating Officer Homewood Retirement Centers, Inc. Homewood at Williamsport Homewood at Frederick Homewood at Plum Creek Homewood at Martinsburg Homewood at Spring House Estates

Similar presentations






 Forms 2007 Illinois State Board of Education June 2007.>")











(1)(2) F428.>")






