Download presentation
Presentation is loading. Please wait.

1
Lucas Thornblade, MD Resident Physician Department of Surgery University of Washington

2
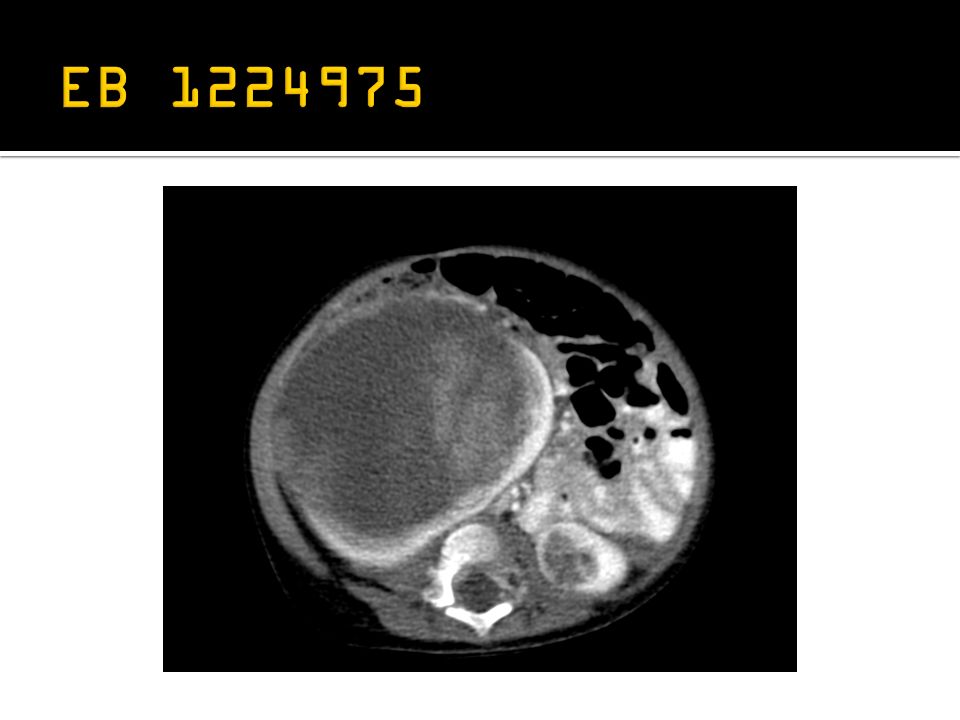
13 month old F Jan. 2013 - presented w/ abdominal distension, pain, fever, constipation -U/S demonstrated bilateral renal masses Feb. – March – six weeks vincristine, dactiomycin, doxorubicin (VDD) Mar. 15 th – bilateral open renal biopsies (R- WT w/o anaplasia, L-intralobular nephrogenic rests) March – May – additional six weeks VDD May 8 th – right radical nephrectomy, left partial nephrectomy, lymphadenectomy -R – stromal type WT w/o anaplasia, direct invasion of adrenal -L – treated nephrogenic rests -negative nodes May 15 th – discharged home, plan for continued chemo
 Mar. 15 th – bilateral open renal biopsies (R- WT w/o anaplasia, L-intralobular nephrogenic rests) March – May – additional six weeks VDD May 8 th – right radical nephrectomy, left partial nephrectomy, lymphadenectomy -R – stromal type WT w/o anaplasia, direct invasion of adrenal -L – treated nephrogenic rests -negative nodes May 15 th – discharged home, plan for continued chemo.")
4
embryonal renal neoplasm -primarily metanephric blastema 7.6 per 1 million children < 15 peak onset at 2 to 3 years Mutations of WT1 WT1 – tumor suppressor gene, 11p13 – zinc finger transcription factor – development of kindey, gonads, spleen, peritoneum

5
WAGR - Syndrome of WT, aniridia, genitourinary abnormalities and MR Denys-Drash Syndrome Beckwith-Wiedemann Syndrome Li-Fraumeni Syndrome Perlman Syndrome Frasier Syndrome

6
incidentally on exam abdominal pain hematuria hypertension 10% - varicocele, hepatomegaly, ascites, CHF

7
Favorable – blastemal, stromal, epithelial Unfavorable – anaplasia, clear cell sarcoma, rhabdoid tumor blastema anaplasia http://www.humpath.com

8
Chung, 2012

9
Accounts for ~5% of Wilms Tumors synchronous or metachronous Management challenge – -maximal renal parenchymal preservation -complete resection for cure of malignancy -historical practice of ablative surgery -resulting renal insufficiency

10
Bishop (1977) – difference in incidence of renal failure -9% (synch) and 18% (meta) BWT -1% unilateral WT Risk of renal failure -loss of renal parenchyma -hyperfiltration injury -nephrotoxic chemotherapy Recommendation NWTSG for preoperative chemotherapy to avoid total nephrectomy
 – difference in incidence of renal failure -9% (synch) and 18% (meta) BWT -1% unilateral WT Risk of renal failure -loss of renal parenchyma -hyperfiltration injury -nephrotoxic chemotherapy Recommendation NWTSG for preoperative chemotherapy to avoid total nephrectomy")
11
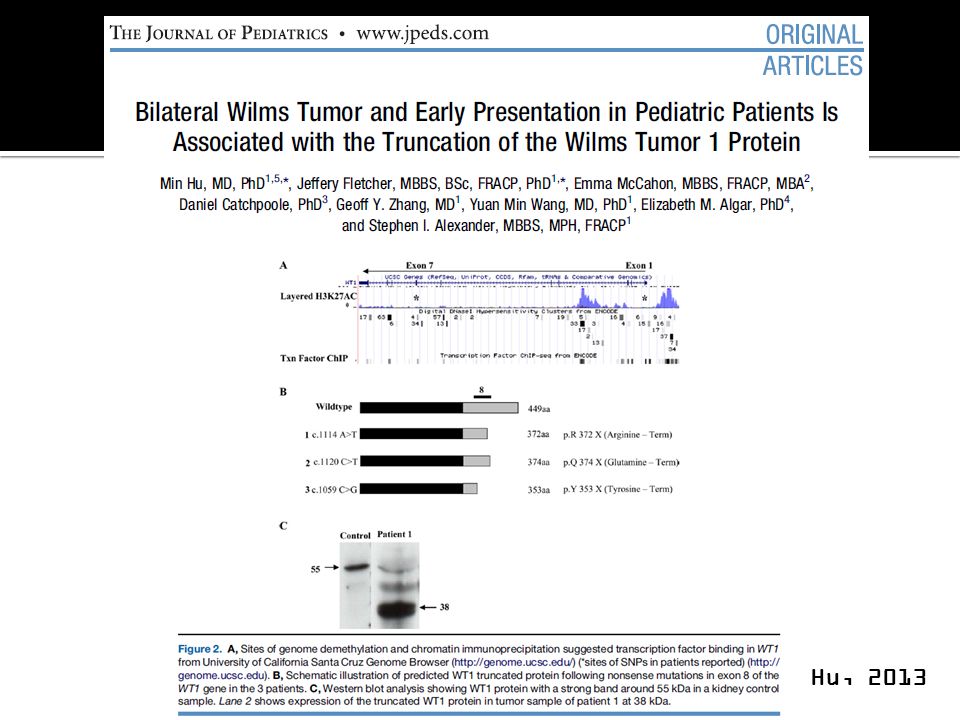
8 patients with bilateral WT (4 mos – 17 yrs) Mutation screening with Western blot 3 of 8 (37%) found nonsense mutations of WT1 Hu, 2013
 Mutation screening with Western blot 3 of 8 (37%) found nonsense mutations of WT1 Hu, 2013")
13
Association of earlier presentation of disease with nonsense mutations -loss of the end portion of WT1 leads to more rapid development of tumors compared with SNP’s Hu, 2013

14
22 patients in a series of 246 WT over 15 years 19 synchronous, 3 metachronous bilateral WT Case series assessed by two treatment arms Sarhan, 2010

15
Group 1: radical nephrectomy with contralateral nephron sparing surgery (6) Group 2: surgery 1.5-6 months after chemo (16) Sarhan, 2010
 Group 2: surgery months after chemo (16) Sarhan, 2010")
16
Preserved renal mass greater in preop chemotherapy group 44% vs. 35% In group 2: 13 of 16 (81%) were down staged following chemotherapy Sarhan, 2010
 were down staged following chemotherapy Sarhan,")
17
NWTS-4 (1986 – 1994) 3335 patients 188 bilateral WT (5.6%) retrospective review Hamilton, 2011 Annals of Surgery
 3335 patients 188 bilateral WT (5.6%) retrospective review Hamilton, 2011 Annals of Surgery")
18
23 of 188 developed ESRD (12%) -6 bilateral nephrectomy -8 did not have nephron sparing approach 22 of 188 had <50% renal parenchyma post-operatively *ESRD is significantly higher in BWT than in unilateral patients Hamilton, 2011 Annals of Surgery
 -6 bilateral nephrectomy -8 did not have nephron sparing approach 22 of 188 had <50% renal parenchyma post-operatively *ESRD is significantly higher in BWT than in unilateral patients Hamilton, 2011 Annals of Surgery")
19
Removal of all gross tumor was successful in 118 of 134 (88%) kidneys after parenchymal sparing surgery -local recurrence in 8% Overall survival for stage V cancer 84% -unfavorable histology as adverse prognostic factor *Survival in BWT is lower than all unilateral WT other than stage IV Hamilton, 2011 Annals of Surgery
 kidneys after parenchymal sparing surgery -local recurrence in 8% Overall survival for stage V cancer 84% -unfavorable histology as adverse prognostic factor *Survival in BWT is lower than all unilateral WT other than stage IV Hamilton, 2011 Annals of Surgery")
20
38 of 188 had progressive or nonresponsive disease after chemotherapy 14% anaplasia in BWT *recommend earlier biopsy if no response to chemotherapy Hamilton, 2011 Annals of Surgery

21
48% reduction in tumor volume after 4 weeks 68% after 8 weeks *continuing preoperative chemotherapy greater than 12 weeks is unlikely to facilitate resection Hamilton, 2011 Annals of Surgery

22
Hamilton, 2011 Annals of Surgery

23
Sarhan, Osama M, El-Baz, Mahmoud, Sarhan, Mohamed M, Ghali, Ahmed M & Ghoneim, Mohamed A. 2010. Bilateral Wilms' tumors: Single-center experience with 22 cases and literature review. Urology 76: 946-951. Hamilton, T. E., Ritchey, M. L., Haase, G. M., Argani, P., Peterson, S. M., Anderson, J. R., Green, D. M. & Shamberger, R. C.. 2011. The management of synchronous bilateral Wilms tumor: a report from the National Wilms Tumor Study Group. Ann Surg 253: 1004-10. doi: 10.1097/SLA.0b013e31821266a0. Hu, M., Fletcher, J., McCahon, E., Catchpoole, D., Zhang, G. Y., Wang, Y. M., Algar, E. M. & Alexander, S. I.. 2013. Bilateral Wilms Tumor and Early Presentation in Pediatric Patients Is Associated with the Truncation of the Wilms Tumor 1 Protein. J Pediatr doi: 10.1016/j.jpeds.2012.12.080. Chung, DH. 2012. Pediatric Surgery. Sabiston Textbook of Surgery: The Biologic Basis of Modern Surgical Practice, 19 th ed. Townsend et al. Saunders/Elsevier Inc.

Similar presentations






>")












